 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 6, September, 2009, pp. 897-900 ARTICLES Relationship among epidemiological parameters of six childhood infections in a non-immunized Brazilian community Marcos AmakuI, +; Raymundo Soares AzevedoII; Ruy Morgado de CastroIII; Eduardo MassadII; Francisco Antonio Bezerra CoutinhoII IDepartamento
de Medicina Veterinária Financial support: CNPq, FAPESP Received 10 March
2009 Code Number: oc09188 ABSTRACT Epidemiological parameters, such as age-dependent force of infection and average age at infection (ā) were estimated for rubella, varicella, rotavirus A, respiratory syncytial virus, hepatitis A and parvovirus B19 infections for a non-immunized Brazilian community, using the same sera samples. The for the aforementioned diseases were 8.45 years (yr) [95% CI: (7.23, 9.48) yr], 3.90 yr [95% CI: (3.51, 4.28) yr], 1.03 yr [95% CI: (0.96, 1.09) yr], 1.58 yr [95% CI: (1.39, 1.79) yr], 7.17 yr [95% CI: (6.48, 7.80) yr] and 7.43 yr [95% CI: (5.68, 9.59) yr], respectively. The differences between average ages could be explained by factors such as differences in the effectiveness of the protection conferred to newborns by maternally derived antibodies, competition between virus species and age-dependent host susceptibility. Our seroprevalence data may illustrate a case of the above-mentioned mechanisms working together within the same population. Key words: seroprevalence - viral diseases - epidemiology - average age - force of infection - Monte Carlo method Certain viral infections are more likely to occur around a given age. For example, rotavirus and respiratory syncytial virus (RSV) typically occur in children under three years of age, while rubella affects 5-9-year-olds (Knipe & Howley 2007). Utilizing seroprevalence data, it is possible to estimate epidemiological parameters and subsequently analyse the dynamics of an infectious disease in different populations. Examples of this approach include analyses of measles, mumps and rubella seroprevalence in different European countries (Edmunds et al. 2000) and in countries in Europe and Latin America (Amaku et al. 2003). A complementary approach is to analyse the dynamics of different infectious diseases within the same community. Information about the average age at infection (ā) will help us characterize the dynamics of an infection in a population. A higher incidence of cases in people of younger or older ages may be associated with several factors, such as sanitary conditions, population density (Almeida et al. 2002), age at which children enter the school system (Yu et al. 2001) and other social and economic variables. For instance, improvements in sanitation as well as the introduction of a vaccination programme may lead to changes in the , which demonstrates the importance of this parameter in the assessment of both the effects of an environmental control programme and the efficacy of a vaccination strategy. To characterise the dynamics of different infectious diseases in the same population, we have estimated the force of infection (λ (a)) and the ā , based on data from a seroprevalence survey carried out in a Brazilian community for antibodies against the following viruses: rubella, varicella, group A rotavirus (rotaA), human RSV, hepatitis A (HAV) and human parvovirus B19 (parvoB19). We have also estimated confidence intervals for using Monte Carlo simulations. SUBJECTS, MATERIALS AND METHODS Data consisted of seroprevalence surveys for IgG antibodies against rubella (Azevedo Neto et al. 1994), varicella (Valentim et al. 2008), rotaA (Cox et al. 1998b), RSV (Cox et al. 1998a), HAV (unpublished data) and parvoB19 (Huatuco et al. 2008) carried out in the community of Caieiras, a small town in the state of São Paulo (SP), Brazil. The population of Caieiras was about 30,000 inhabitants in 1990, most of them inhabiting an urban area occupying 104 km2. Samples were collected from 476 individuals randomly selected by cluster sampling from November 1990-January 1991. The seroprevalence study was carried out in dwellings from 30 of the 60 administrative regions to obtain a sample representative of the population living in Caieiras, including newborns to adults 40 years of age. More details are published elsewhere (Azevedo Neto et al. 1994). Let S+(a) be the proportion of seropositive individuals with age a. An estimate of the function S+(a) resulted from fitting the serological data to each disease (Farrington 1990, Amaku et al. 2003)
where k1 and k2 are fitting parameters, estimated by either the Maximum Likelihood or the Least Squares technique. In our model, the seropositive individuals correspond to those who are either infected or immune. The λ (a) was estimated from the seroprevalence data for the so-called catalytic approach (Griffiths 1974):
Equation (2), expressed in terms of equation (1), is
From the λ (a), we can define the average age at which susceptibles acquire infection:
We have taken the highest age observed in the seroepidemiological survey (L = 40 years) as the upper integration limit of the integrals of equation (4). In this paper, we are assuming that the immune response is not lost over time for the diseases studied. Monte Carlo simulations - From the fitting procedure, we have estimated the variance-covariance matrix V for the parameters of the seroprevalence function [equation (1)]
where Sk2i
(i = 1,2) is the variance of the parameter ki (i
= 1,2) and cov(k1, k2) the covariance between
the two parameters. The fitted parameters will be indicated as The correlation coefficient between k1 and k2 is defined as
and it always lies in the interval -1 < ρ < 1. If ρ =0, k1 and k2 are said to be uncorrelated, if ρ > 0, they are positively correlated and, if ρ < 0, negatively correlated. As we have an estimate of the variance-covariance matrix V, we can randomly generate pairs of values (k1, k2) and calculate the ā. The Monte Carlo
algorithm we have adopted is based on the generation of random numbers for k1
and k2 and on the substitution of these values in equation
(4) for the . We have supposed that k1 and k2
are normally distributed with the means
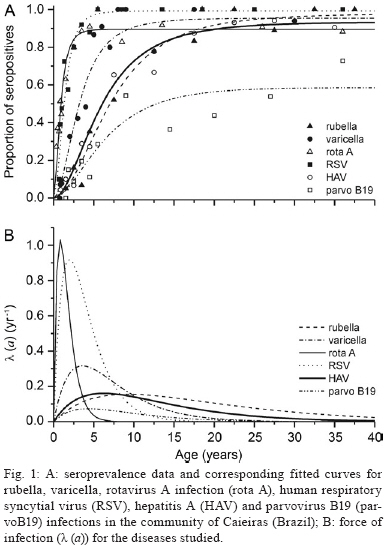
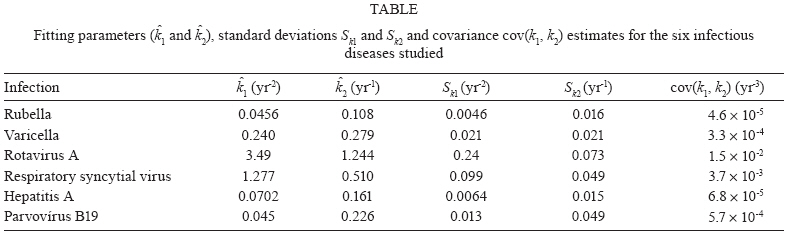
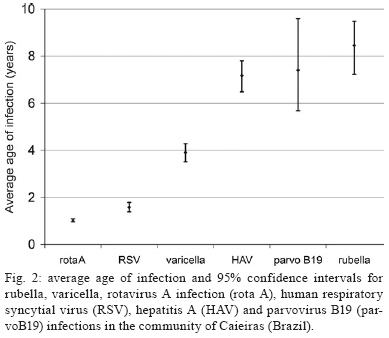
where g1() and g2() are two different normal random generators with mean zero and variance 1. The computational routines we have used to generate random numbers are those described by Press et al. (1992). RESULTS Fig. 1 shows the fitted seroprevalence curves (Fig. 1A) for the six infectious diseases considered and the respective forces of infections (Fig. 1B). The estimates for the fitting parameters are shown in Table. The ā and the 95% confidence intervals estimated using the Monte Carlo method for rubella, varicella, rotavirus A, human RSV, HAV and parvoB19 were 8.45 years (yr) [95% CI: (7.23, 9.48) yr], 3.90 yr [95% CI: (3.51, 4.28) yr], 1.03 yr [95% CI: (0.96, 1.09) yr], 1.58 yr [95% CI: (1.39, 1.79) yr], 7.17 yr [95% CI: (6.48, 7.80) yr] and 7.43 yr [95% CI: (5.68, 9.59) yr], respectively. The highest values for the λ (a) were observed for rotavirus A and RSV, followed by varicella, all of which had an of less than five years. The λ (a) curve for rotavirus A showed a sharp peak around one year of age, followed by a steep decrease and vanished after five years of age. The sharp peak for RSV occurred around two years and was followed by a decrease slower than that observed for rotavirus A, vanishing only after the age of 10 years. The λ (a) curve for parvo B19 showed the smallest intensity among the infections studied. The λ (a) curves for rubella and HAV indicated intermediate intensity, being higher than that of parvo B19, but not reaching the intensity of the RSV and rotavirus A curves. The average ages observed for rubella and HAV were 8.45 yr and 7.17 yr, respectively. By visual inspection, taking into account the confidence intervals, differences between values for the infections studied are noticeable, with the exception of parvo B19 when compared to HAV and rubella (Fig. 2). DISCUSSION We analyzed seroepidemiological data for six viral infectious diseases in the same population. Our results for rotavirus A are in agreement with the prevalence observed by Candeias et al. (1989) in the city of São Paulo from data obtained in outpatient departments of hospitals, showing this disease occurs early during infancy. The same is true for RSV, as shown by Vieira et al. (2007). In the case of varicella, two different samples from Caieiras (Yu et al. 2001, Valentim et al. 2008) showed similar seroprofile patterns. However, the seroprevalence for Caieiras is different than that of city of São Paulo (Yu et al. 2001) due to differences in the children's social behaviour. The HAV seroprevalence found in our analysis is very similar to the profile observed in the Rio de Janeiro metropolitan area (Almeida et al. 2002) and is typical of urban areas. As for parvoB19, serological data published for Rio de Janeiro (Nascimento et al. 1990) showed a higher prevalence in young adults (80%) compared with the data presented here for Caieiras. The rubella seroprevalence described here for Caieiras is similar to data published by Souza et al. (1994) for the city of São Paulo from a survey carried out on sera collected in 1987, which suggests that the Caieiras population is representative of the São Paulo metropolitan region population. Based on seroprevalence data, we estimated the age-dependent λ (a) and the average age of first infection. These epidemiological parameters were used in previous publications to verify the effect of different vaccination strategies (Amaku et al. 2003). The average age at first infection is an important reference for determining the optimum age for vaccine introduction. It was demonstrated that immunization for rubella is not effective if proposed for ages around or above the ā (Amaku et al. 2003). Although this is a relative simple parameter, as shown by our results, it can support health authorities' decisions around establishing a vaccination schedule. The application of the parameters estimated in this paper proved to be useful when the immunization campaign against rubella was designed for SP in 1992 (Massad et al. 1994, 1995). This campaign was successful at reducing the incidence of rubella. The differences observed among the epidemiological parameters estimated for these six infectious diseases may not be solely due to the contact pattern among individuals because the individuals sampled are the same. Therefore, other factors should be considered as influential to the epidemiology of each disease by mathematical modelling. If we consider that all viruses are circulating in the population, why don't we observe constant proportions of population infected across all age groups? Depending on the infection, factors such as protection by maternal derived antibodies, transmission route, age-dependent host susceptibility and competition among different virus species may also help to explain the observed age-dependent pattern of disease transmission. The decline of maternal derived antibodies from birth onwards may interfere with the acquisition of an infection in the first year of life, altering the average age at first infection. RSV, for example, requires a high titer of maternal derived antibodies to be neutralized, making infants susceptible after two months of age (Collins & Crowe 2007). This fact may explain the rapid spread of RSV infection in the first two years of life. It may also be the explanation for other diseases that spread among infants, such as rotavirus A infection. According to our results, the route of transmission did not seem to make a difference in terms of when an infection would occur. For instance, rotavirus A and HAV are both mainly transmitted by a faecal-oral route, but the former has an average age of first infection of one year and the latter seven years. Infectivity is another characteristic that varies among pathogens and it may be important in determining the success of rotavirus and RSV acquisition so early in an infant's life as compared to other illnesses such as rubella or parvoB19, for example. Regarding competition among viruses, it should be considered that nonspecific immune responses produced by one viral infection may inhibit a concomitant infection by another virus. Although simultaneous virus infection in the same host was demonstrated for RSV, adenovirus, metapneumovirus, rhinovirus, enterovirus, influenza and parainfluenza in different combinations (Calvo et al. 2008), concurrent infection is less likely to occur, making competition a good hypothesis to explain why some diseases like rubella and parvoB19 appear less frequently in infants and toddlers. We have observed that viral infections like rotavirus A and RSV have a lower average age of first infection as compared with varicella, which, in turn, is lower than HAV, parvoB19 and rubella. Our seroprevalence data may illustrate the above-mentioned mechanisms working together within the same population. If it is true that there is an interaction among virus and human populations that drives the observed age-dependent incidences, it is plausible that a change in the seroprevalence pattern of a disease may be instigated by the introduction of vaccine against another disease. Further investigation of the seroprevalence profiles of different diseases within the same population should be carried out to elucidate whether such an interaction occurs after the introduction of immunization. REFERENCES
Copyright 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09188f1.jpg] [oc09188t1.jpg] [oc09188f2.jpg] |
| |||||||||






{kind=link}
{kind=link}
{kind=link}