 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 104, No. 8, 2009, pp. 1139-1147 ARTICLES Clinical and laboratory status of patients with chronic Chagas disease living in a vector-controlled area in Minas Gerais, Brazil, before and nine years after aetiological treatment Marta de LanaI, +; Leonardo A LopesII; Helen R MartinsII; Maria T BahiaIII; Girley F Machado-de-AssisII; Ana P WendlingIV; Olindo A Martins-FilhoIV; Roberto A MontoyaV; João CP DiasIV; Pedro Albajar-ViñasVI; José R CouraVI IDepartamento
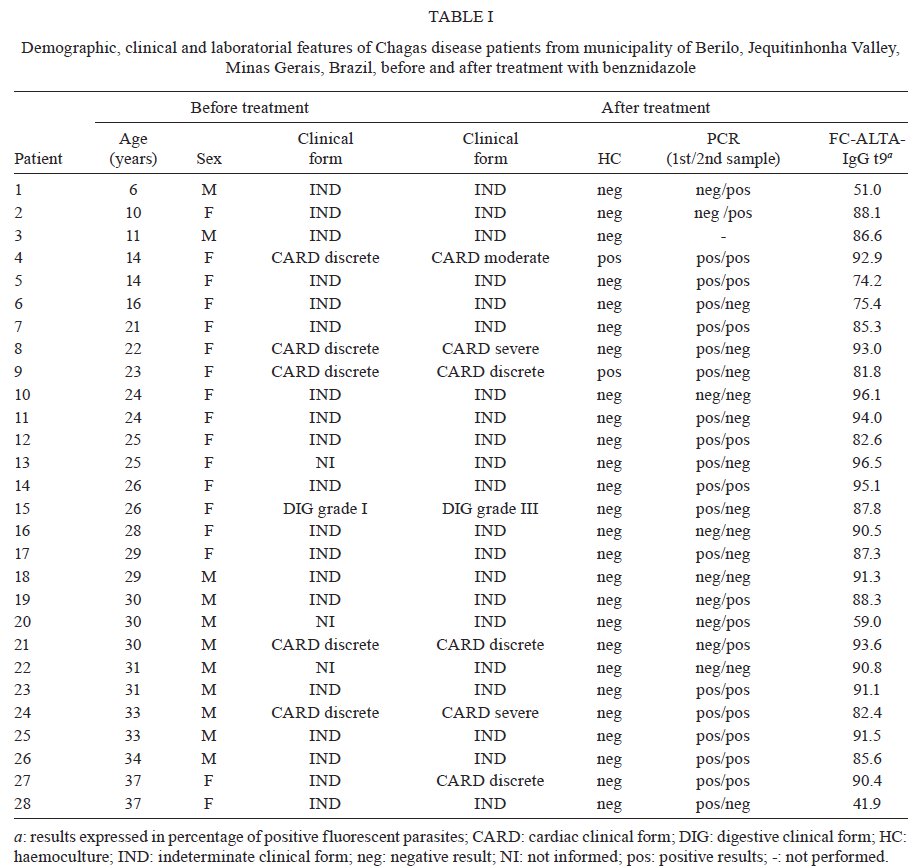
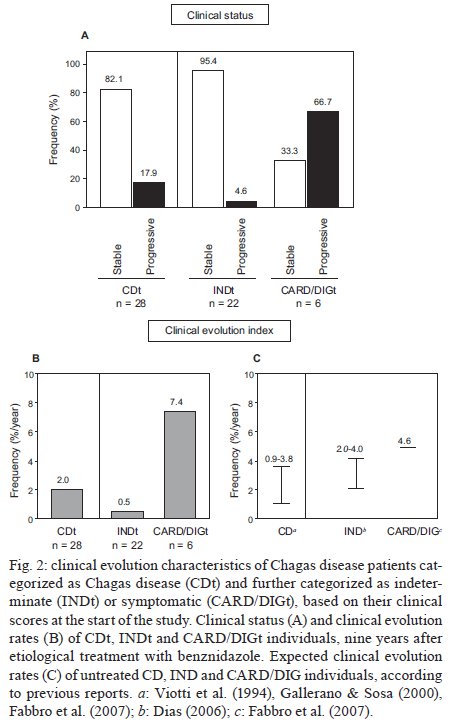
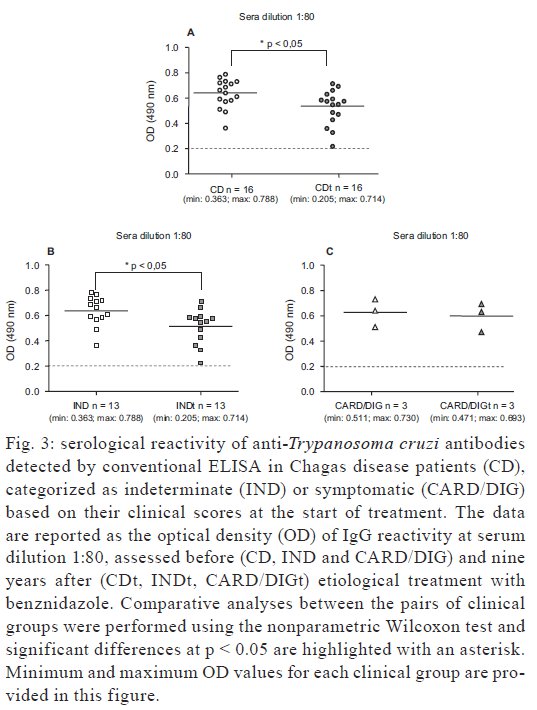
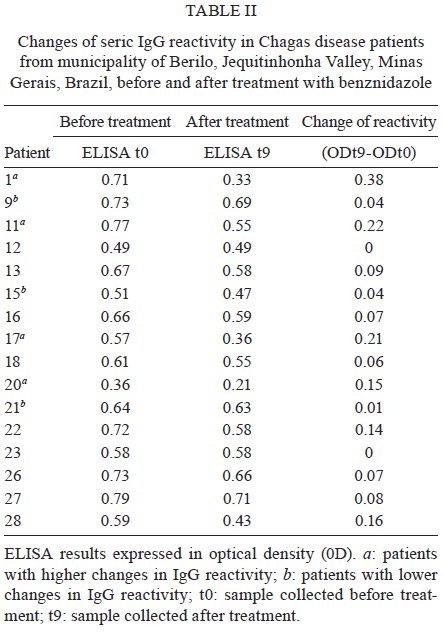
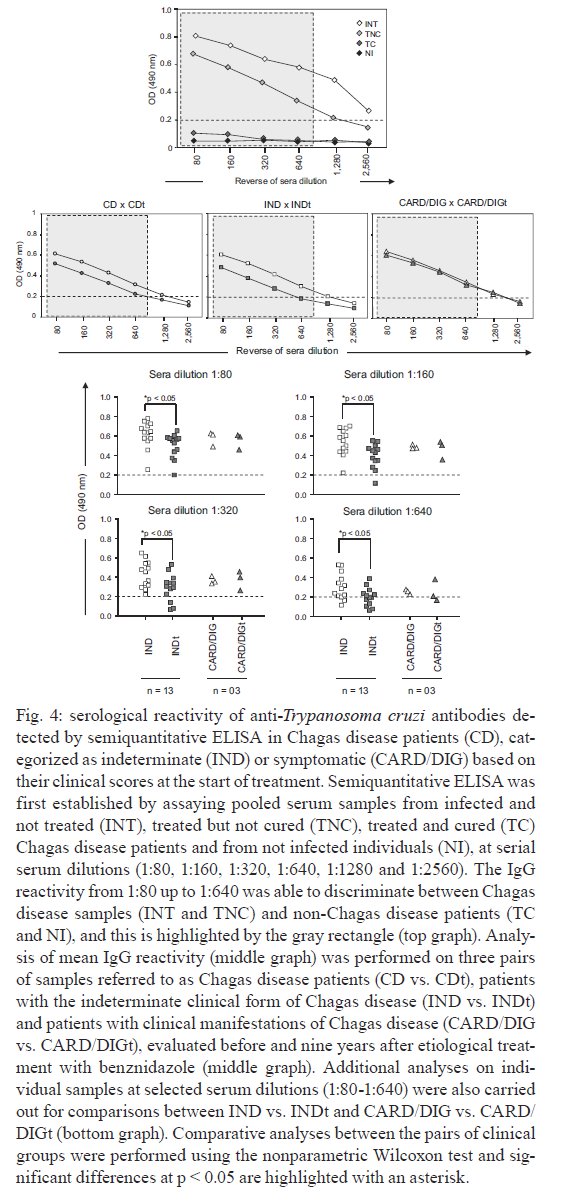
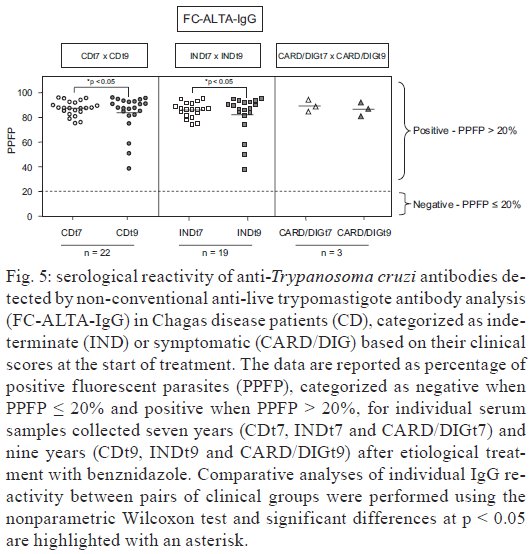
de Análises Clínicas, Escola de Farmácia Financial support: FAPEMIG (PPSUS/05, 3242/06), CNPq (481097/2004-0), SESU/MEC, PROEX/UFOP Received 13 February 2009 Code Number: oc09229 ABSTRACT Twenty-eight Chagas disease patients (CD), 22 with the indeterminate clinical form (IND) and six with the cardiac or digestive form (CARD/DIG), were treated with benznidazole and underwent clinical and laboratorial analysis before (IND and CARD/DIG) and nine years after [patients after treatment (CDt), patients with the indeterminate clinical form at treatment onset (INDt) and with the cardiac or digestive form at treatment onset (CARD/DIGt)] treatment. The data demonstrate that 82.1% of CDt patients (23/28) remained clinically stable and 95.4% of the INDt (21/22) and 33.3% of the CARD/DIGt (2/6) patients showed unaltered physical and laboratorial examinations. The clinical evolution rate was 2%/year and was especially low in INDt patients (0.5%/year) relative to CARD/DIGt patients (7.4%/year). Positive haemoculture in treated patients was observed in 7.1% of the cases. None of the INDt (0/21) and 33.3% of the CARD/DIGt (2/6) patients displayed positive cultures. The PCR presented a positive rate significantly higher (85.2%, 23/27) than haemoculture and two samples from the same patient revealed the same result 57.7% of the patients. Conventional serology-ELISA on 16 paired samples remained positive in all individuals. Semi-quantitative ELISA highlighted significant decreases in reactivity, particularly in INDt relative to IND. Non-conventional serology-FC-ALTA-IgG, after treatment, showed positive results in all sera and 22 paired samples examined at seven and nine years after treatment, demonstrated significantly lower reactivity, particularly in INDt patients. This study was retrospective in nature, had a low number of samples and lacked an intrinsic control group, but the data corroborate other results found in the literature. The data also demonstrate that, even though a cure has not been detected in the none-treated patients, the benefits for clinical evolution were selectively observed in the group of INDt patients and did not occur for CARD/DIGt patients. Key words: Chagas disease - aetiological treatment - benznidazole - clinical-laboratorial evaluation - clinical evolution Chagas disease has been brought under control in several Latin American countries due to successive vector control programs along with successful blood transfusion control (WHO 2005). Nevertheless, the large numbers of individuals infected with Trypanosoma cruzi still represent a serious public health problem and an important challenge for physicians and the scientific community. Therefore, continuing epidemiological surveillance activities relating to Chagas disease are recommended (Dias 2002). Despite the urgent need to develop drugs that are more effective for aetiological treatment of Chagas disease, the only compounds currently available are benznidazole and nifurtimox (Coura & Castro 2002). The general consensus is that there is greater therapeutic effectiveness during the acute phase of the disease (70-90% of cure), in recent infections (present for less than 12 years) and among young patients compared with individuals treated during late chronic infection (Cançado 1997, Anonymous 2005). In addition to the lower efficacy of chemotherapy applied to chronic infection, the belief that autoimmune events play an important underlying role in Chagas pathogenesis, even after the post-therapeutic parasite clearance (Coura et al. 1997), has led several investigators to conclude that it is not worth treating chronic Chagas disease patients (CD). However, a few follow-up studies on treated CD have pointed out that, in fact, despite the autoimmune mechanisms triggered by T. cruzi infection, most tissue damage is indeed dependent on the presence of the parasite (Viotti et al. 1994). In fact, several authors have also demonstrated that real benefits are observed following specific chemotherapy, regardless of whether a parasitological cure is achieved (Segura et. al. 1994, Viotti et al. 1994, 2006, Galerrano & Sosa 2000, Suasnábar et al. 2000, Streiger et al. 2004, Fabbro et al. 2007). These effects have been observed especially when specific treatment was offered to young patients or to those with mild disease, such that better prognosis for the infection or even regression of the lesions or clinical cardiac or digestive symptoms was observed (Fabbro et al. 2007). Similar findings have also been observed following treatment of experimental T. cruzi infections (Andrade et al. 1991). However, controversy still exists regarding the real effects of these drugs on the clinical evolution of Chagas disease, especially during the chronic phase of the disease (Macedo & Silveira 1987, Braga et al. 2000, Lauria-Pires 2000). The controversy is most likely due to the use of different treatment schemes and/or evaluation protocols (Bahia et al. 2006). Consequently, despite the evidence that trypanocidal therapy may impact positively on the clinical course of the disease in chronic patients (Sosa & Segura et al. 2006, Bern et al. 2008), there is neither a consensus nor sufficient data to support the routine use of the aetiologic treatment of this condition (Marin-Neto et al. 2009). In fact, the major concern to be considered with regard to truly demonstrating the efficacy of treatment and the beneficial impact of aetiological treatment on the clinical evolution of Chagas disease is the need for long-term follow-up of treated patients (Coura & Castro 2002). In this context, a recent randomised double-blind controlled clinical trial (BENEFIT) was launched in countries with a high incidence of Chagas disease to clarify the role of trypanocidal therapy in preventing cardiac disease progression and death using the standardised protocol for treatment, clinical evaluation and cure assessment (Marin-Neto et al. 2009). Extending the work on this issue, the intention of the present investigation was to perform a comparative evaluation of CD in a vector-controlled area [the municipality of Berilo, Minas Gerais (MG), Brazil] before and nine years after aetiological treatment. This study covered important aspects of post-therapeutic cure criteria, including the parasitological/serological status and clinical scores of treated CD. PATIENTS AND METHODS Patient sample - Twenty-eight individuals, 6-37 years old (9 males and 19 females), were evaluated. All of the subjects were living in the Jequitinhonha Valley, a vector-controlled area within the municipality of Berilo, MG, Brazil (Fig. 1). The major demographic, clinical and laboratory characteristics of all the subjects, obtained before and nine years after treatment with benznidazole, are summarised in Table I. Clinical and laboratory evaluation - Before treatment, the laboratory diagnosis of Chagas disease was confirmed by two serological tests [indirect immunofluorescence and indirect haemagglutination (IHA)](data not shown). Additional serological analysis was performed using conventional methods. All of the CD were physically and clinically examined and electrocardiograms and chest X-rays were recorded. Cases of cardiopathy were classified according to clinical and electrocardiographic criteria as recommended by OMS/OPAS (1974). Twenty-two out of the 28 patients presented the indeterminate clinical form of the disease, while five were classified as mild cardiac patients and one as a megaoesophagus group I digestive patient, in accord-ance with Resende et al. (1960). The patients were observed for any abnormal renal or hepatic conditions and they all received specific treatment with benznidazole. The treatment consisted of administration of the nitroderivative benznidazole (N-benzyl-2-nitroimidazole acetamide - Roche®). The therapeutic scheme consisted of 5-10 mg/kg/day for 40-60 consecutive days. During treatment, all patients were re-evaluated at regular intervals of 15 days or whenever any side effects were observed. The most frequent side effects observed were anorexia, muscle pain and exanthema. One case of severe adverse effects was documented and this individual's treatment was temporarily interrupted until the laboratorial parameters returned to normal. After treatment, the laboratory evaluation consisted of parasitological and serological tests, as follows: Parasitological tests - For parasitological tests, two samples from each patient (collected within a one-year interval) were employed. Blood culturing was performed using a volume of 30 mL of blood, processed as described by Chiari et al. (1989). Blood samples for PCR were collected in an equal volume of guanidine 6 M and EDTA 0.2 M, pH 8.0. The DNA extraction and PCR reaction were performed in accordance with Gomes et al. (1998). Positive, negative and reagent controls were processed in parallel in each assay in all stages. The first sample was subjected to two independent PCR analyses. Once the results were reproducible among the two different extractions in the first sample, the second sample was submitted to a single PCR analysis. The primers S35 and S36 were used for amplification of kDNA minicircles in the presence of Taq DNA polymerase (Platinum, Invitrogen). The products were verified on polyacrylamide gels and the PCR results were compiled after two tests, with the results reported as negative or positive. Serological tests - Conventional serological evaluations were performed by means of ELISA and IHA tests and they confirmed the diagnosis of Chagas disease for all the patients (data not shown). Additionally, conventional ELISA was performed on 16 samples paired with those stored at the Laboratório de Doenças Parasitárias (Instituto Oswaldo Cruz-Fiocruz, Rio de Janeiro, RJ, Brazil), with the aim of investigating whether there was any decrease in antibody levels after treatment. ELISA was performed essentially as described by Voller et al. (1976) but modified by using 4.5 μg/mL antigen, a serum dilution of 1:80 and peroxidase-conjugated anti-human IgG conjugate. The results are expressed as optical densities (OD) and as "changes in IgG reactivity" (i.e., ODt9-ODt0). Furthermore, semiquantitative ELISA was applied to characterise the changes in serological reactivity following aetiological treatment. The semiquantitative ELISA was first established using serial dilutions (1:80; 1:160; 1:320; 1:640; 1:1,280 and 1:2,560) of pooled serum samples from infected non-treated patients (INT), treated and not cured patients (TNC), treated and cured patients (TC) and non-infected individuals (NI) that were stored at the Laboratório de Doença de Chagas, Instituto René Rachou-Fiocruz, Belo Horizonte, MG, Brazil. Non-conventional serological testing was performed by means of analysing anti-live-trypomastigote antibodies (FC-ALTA-IgG) in sera from all 28 patients (collected 9 years after aetiological treatment), as described by Cordeiro et al. (2001). The test was considered positive when the percentage of positive fluorescent parasites (PPFP) was greater than 20%. Additionally, FC-ALTA-IgG was performed on 22 samples paired with those collected seven years after treatment, which were stored at the Laboratório de Doença de Chagas, Núcleo de Pesquisas em Ciências Biológicas, Universidade Federal de Ouro Preto, Ouro Preto, MG, Brazil. The clinical and physical examinations and the clinical classifications of the patients were performed by our clinical team following the same criteria that had been used prior to treatment. Statistical analysis - Comparative analyses of serological status before and after treatment with benznidazole, including the IgG level detected by conventional ELISA, semiquantitative ELISA and FC-ALTA-IgG, were performed using the Wilcoxon test. The results were considered significant when p < 0.05. For comparative analysis, three groups of subjects were used: CD, patients with the indeterminate clinical form of Chagas disease (IND) and patients with cardiac/digestive clinical manifestations of Chagas disease (CARD/DIG), evaluated before (CD, IND and CARD/DIG) and nine years after [CD after treatment (CDt), patients with the indeterminate clinical form of Chagas disease at treatment onset (INDt) and patients with the cardiac or digestive form of Chagas disease at treatment onset (CARD/DIGt)] treatment with benznidazole. Ethics - This study complied with resolution 196/1996 from the National Health Council for research involving humans and all of the patients and legal guardians read and signed the consent form (Committee on Human Experimentation from CPqRR, Fiocruz, Belo Horizonte, MG - process 007/2002). RESULTS Clinical evaluation after aetiological treatment - The comparative analysis of the clinical status of the 28 CD before and after aetiological treatment with benznidazole is summarised in Table I and Fig. 2. Although the number of patients evaluated was low, five out of the 28 patients (17.9%) had progressive disease (Fig. 2A), reaching a clinical evolution rate of 2% nine years after treatment (Fig. 2B). Disease progression was observed in only one out of the 22 patients (4.6%) who had presented the indeterminate clinical form before treatment (Fig. 2A). This individual's case evolved to a mild cardiac clinical form (patient 27) (Table I), leading to a clinical evolution rate of 0.5%/year (Fig. 2B). On the other hand, four out of the six patients (66.7%) who displayed clinical manifestations of Chagas disease (CARD/DIG) before treatment (Fig. 2A) evolved towards a more severe clinical status (patients 4, 8, 15 and 24) (Fig. 2A), resulting in a clinical evolution rate of 7.4%/year (Fig. 2B). Fig. 2C illustrates the expected natural clinical evolution rate for untreated Chagas disease according to previous reports (Viotti et al. 1994, 2006, Gallerano & Sosa 2000, Dias 2006, Fabbro et al. 2007). Parasitological analysis - Blood culturing was performed after treatment for all 28 of the treated CD (two blood samples from each patient). Two out of the 28 treated patients (7.1%) showed positive blood cultures: both of them presented clinical manifestations of Chagas disease before treatment (patients 4 and 9) (Table I). None of the patients who displayed the indeterminate clinical form of Chagas disease before treatment showed positive blood cultures nine years after treatment, whereas 33.3% (2/6) of the patients with clinical manifestations before treatment (CARD/DIG) presented positive blood cultures. PCR analysis demonstrated that four out of the 27 CD (14.8%) displayed negative PCR results nine years after aetiological treatment (patients 10, 16, 18 and 22) after evaluation of two different samples, while 85.2% (23/27) showed positive results (Table I). The percentages of agreement between the results of two distinct samples were 57.7%, with 69.2% positive in the first sample and 59.3% in the second. The percentages of indeterminate patients displaying negative or positive PCR were 20% (4/20) and 80% (16/20), respectively, whereas for patients with clinical manifestations before treatment, these frequencies were 0% (0/6) and 100% (6/6), respectively (Table I). Conventional and semiquantitative ELISA - The serological analyses performed by conventional ELISA on 16 paired serum samples are shown in Fig. 3. Interestingly, although positive results from ELISA were observed in all 16 samples tested, a significant decrease in IgG reactivity was detected after treatment, selectively in the group of IND patients (Fig. 3A, B). Four serum samples (patients 1, 11, 17 and 20) presented larger decreases in IgG reactivity (Table II) and all of them had the indeterminate clinical form of the disease (Table I). Smaller decreases in IgG reactivity were observed in three serum samples (patients 9, 15 and 21) (Table II) and all of them presented clinical manifestations of Chagas disease before treatment (Table I). The semiquantitative ELISA was first established by assaying pooled serum samples from INT, TNC and TC CD, along with samples from NI. The aims were to stand-ardise the methodology and establish the interpretation criteria for evaluating post-therapeutic cure (Fig. 4, top graph). Data analysis demonstrated that IgG reactivity from 1:80 up to 1:640 was able to discriminate between Chagas disease samples (INT and TNC) and non-CD (TC and NI) (Fig. 4, top graph). This approach was used to analyse the mean IgG reactivity from 16 paired serum samples obtained before and nine years after treatment. The results demonstrated changes in CD vs. CDt and IND vs. INDt, which were similar to the profile observed for INT vs. TNC. On the other hand, no changes in mean IgG reactivity were observed for CARD/DIG vs. CARD/DIGt (Fig. 4, middle graph). The analysis of IgG reactivity in individual samples at selected serum dilutions (1:80-1:640) demonstrated that 1:320 was the most promising serum dilution, capable of identifying all of the CD as positive before treatment (IND and CARD/DIG) and capable of discriminating between serological reactivities after treatment, particularly when comparing IND vs. INDt (Fig. 4, bottom graph). Specifically, at serum dilution 1:320, three serum samples (patients 1, 17 and 20) that all presented IND displayed IgG reactivity that was lower than the cut-off. No significant decrease in IgG reactivity was observed in the patients with clinical manifestations of Chagas disease (CARD/DIG vs. CARD/DIGt) (Fig. 4, bottom graph). Non-conventional anti-live trypomastigote antibody analysis - FC-ALTA-IgG - The serological analyses performed using non-conventional FC-ALTA-IgG on 22 paired serum samples are shown in Fig. 5. Although all 22 of the samples tested were positive using FC-ALTA-IgG, a significant decrease in mean IgG reactivity was detected after treatment, selectively in the group of IND patients (Fig. 5). A change in individual IgG reactivity was observed selectively in INDt (INDt7 vs. INDt9), with three serum samples (patients 1, 20 and 28) displaying the lowest PPFP values (Fig. 5). DISCUSSION One of the major challenges in investigating Chagas disease is the complexity of evaluating the impact of chemotherapy on the clinical and laboratory characteristics of treated patients. Controversy still exists in relation to data that show that aetiological treatment has a positive impact and leads to diminished clinical evolution, mainly due to the different approaches and methods used by different authors (Bahia et al. 2006). This situation is exacerbated when managing treated chronic CD, since a longer follow-up investigation becomes necessary. Additionally, despite the lack of consensual cure criteria, a large number of laboratory methodologies (Coura & Castro 2002)are still important for to determining whether a post-therapeutic cure has been achieved in Chagas disease cases. The purpose of the present investigation was to contribute to this important point by evaluating the clinical, parasitological and serological characteristics of a group of 28 CD who were treated with benznidazole during the chronic phase of the infection. Despite the low number of samples, the results demonstrate that, when all patients are considered together (CDt), the overall clinical evolution rate observed (2%/year) is very similar to what was previously described for untreated CD (Viotti et al. 1994, 2006, Gallerano & Sosa 2000, Fabbro et al. 2007), However, the data analysis indicates that INDt present a clinical evolution rate of only 0.5%/year. This is lower in comparison to what has been observed by other authors in epidemiological and clinical studies of the un-treated IND in Brazil, from which rates ranging from 2% to 4%/year were recorded (Prata 2001, Dias 2006). Moreover, the rate observed for INDt was lower than that measured for patients presenting previous clinical manifestations of the disease (CARD/DIGt = 7.4%/year). These findings are also lower than what was observed by Montoya (1998), who demonstrated an incidence of 1.5%/year (3 times higher than that observed in this study) for Chagas disease cardiopathy among untreated indeterminate patients in a 10-year follow-up study performed in Berilo. It is interesting to note that the only case among the INDt patients that evolved towards a symptomatic clinical form was from the oldest patient in this group (patient 27; age: 37 years). This corroborates previous observations from other authors, which stated that the impact of the aetiological treatment on late chronic infection is not as evident as the impact on younger patients (Gallerano & Sosa 2000, Cançado 2002), although treatment could interrupt or delay patients' clinical evolution. Consequently, these data reinforce the importance of aetiological treatment for IND, as recommended by previous authors and by the Brazilian consensus resolution (Anonymous 2005) regarding specific treatment for Chagas disease. The effect of the treatment on the chronic infection is controversial and difficult to demonstrate due to the limitation of the serological and parasitological methods available for cure detection. Several studies have demonstrated that treatment promotes remarkable reduction in the levels of antibodies and parasitaemia (Viotti et al. 1994, Fabro et al. 2007). Considering that the positive haemoculture rate in untreated patients in Berilo has been 36% (unpublished observations), herein the results also demonstrate that the effect of treatment significantly reduced parasitaemia because the rate of positive blood culture in the treated group was only of 71.4% (2/28). Despite the low number of patients in this study, it is also interesting to note that positive results in treated patients were observed only within the CARD/DIGt group, which represents clear evidence of therapeutic failure. Parasitological tests (e.g., xenoculture and haemoculture) typically have very low sensitivity in the chronic phase of the disease and may yield negative results, even when repeated several times post-treatment (Castro et al. 2002). On the other hand, it has been demonstrated that PCR is the most sensitive method for detection of the parasite in the peripheral blood of patients in this phase of the infection (Britto et al. 2001). Our results corroborated this observation, showing that PCR displays significantly higher sensitivity to demonstrate the presence of the parasite: only four out of the 28 patients (14.8%) consistently displayed negative results and 23 (85.2%) were positive when two different samples were evaluated. The first sample was 69.2% positive, while the second was 59.3% positive, yielding an agreement between the results of 57.7%. This demonstrates the importance of the examination of at least two samples to increase the rate of parasite detection, as previously verified by Castro et al. (2002). Considering that patients in the chronic phase present low and intermittent parasitaemia, the parasites may not be detected in only one sample. Thus, negative PCR results should be interpreted with caution. Here, negative PCR results were observed exclusively in the INDt group. Although the real meaning of PCR results as a cure control has not been definitively determined (Martins et al. 2008, Britto 2009), the negative blood culture and PCR results observed in four INDt patients may be considered at least indicative of a significant reduction of parasitaemia. We did not observe a correlation between the negative parasitological tests and a reduction in the antibody levels, but patients who presented the greatest reduction of IgG also presented at a least one positive PCR reaction. The serological evaluations using conventional ELISA and FC-ALTA-IgG demonstrate that all of the CDt patients presenting positive results may represent therapeutic failure, according to the cure criterion established by Krettly and Brener (1982) and Martins-Filho et al. (1995). With the aim of further focusing on the serological features of treated individuals, IgG reactivity was analysed using semiquantitative ELISA on serum samples from 16 paired samples, obtained before and nine years after treatment. The data analysis showed a significant decrease in antibody reactivity (particularly in INDt) in relation to IND, for all of the selected serum dilutions. It was demonstrated that the dilution of 1:320 is the most promising for discriminating the serological reactivities of anti-T. cruzi IgG antibodies. Three INDt (patients 1, 17 and 20) presented the highest decreases in IgG titers. No changes in OD values from semiquantitative ELISA were observed in the CARD/DIGt group. Interestingly, the patient who presented the largest decrease in IgG reactivity that was detected by ELISA (patient 1; age: 6 years) was the youngest patient treated. This represents an example of parasitological cure in progress, in accordance with the case mentioned by Luquetti & Rassi (1998). This result also corroborates the observation that chemotherapy for Chagas disease is more successful in young people, especially under the age of 12 (Sosa-Estani & Segura 2006). Interestingly, no significant changes in antibody levels were observed in patients within the CARD/DIGt group. This result also corroborates affirmations regarding the real benefit from specific treatment for those in the chronic phase of Chagas disease (Ianni & Mady 1998, Fabbro et al. 2006). Although no CDt patients presented negative results in the FC-ALTA-IgG analysis (carried out 7 and 9 years after treatment), a significant decrease in PPFP values was observed in three patients, selectively in the INDt group (patients 1, 20 and 28). Two of these patients (1 and 20) were the same ones that presented decreased IgG reactivity in the semiquantitative ELISA test. No changes in PPFP values were observed in the CARD/DIGt patients. When specific chemotherapy is administered to chronic patients, the decrease in serological titers of anti-T. cruzi antibodies occurs so slowly that the confirmation of cure assayed by conventional serology has only been achieved 10-25 years after treatment. These differences are due to the lower time of infection, methodological differences used in the evaluations and/or differences of the parasite's susceptibility to treatment of distinct geographical regions (Andrade et al. 1996, Coura & Castro 2002). In fact, Galvão et al. (2003) have already demonstrated the early negativity of parasitological methods used among treated patients, in relation to serological methods. Therefore, we hypothesise that the presence of positive conventional ELISA, along with positive non-conventional FC-ALTA-IgG, that was observed in all CDt patients should not be considered therapeutic failure. Moreover, further evaluations should be carried out in such cases to fulfil the cure criteria proposed by Krettli and Brener (1982), Martins-Filho et al. (1995), Cançado (2002) and Coura and Castro (2002). Taken together, after the cure criterion was adopted, no parasitological cure was observed in any of the treated CD patients whom we evaluated. However, considering the small number of samples, the data presented here suggest that even in the absence of cure, the treatment may have prevented or delayed the natural history of Chagas disease evolution in INDt, as demonstrated in other studies using considerable numbers of samples (Segura et al. 1994, Viotti et al. 1994, 2006, Galerrano & Sosa 2000, Suasnábar et al. 2000, Streiger et al. 2004, Fabbro et al. 2007). Additionally, meta-analyses with relevant data about Chagas disease treatment have been previously reported by Villar et al. (2002), Reyes and Vallejo (2005) and Coura (2009). Although this study was performed without evaluating a parallel standardised control group of untreated patients, our data suggest that benznidazole treatment produces beneficial effects selectively in the INDt group. This agrees with the view of the natural evolution of the disease described by Montoya (1998) in Berilo, who revealed that electrocardiographic alterations were present in 30.5% of CD patients, generally before 30 years old. This reality should be kept in mind by physicians when faced with newly diagnosed cases of Chagas disease. The data demonstrate that the benefits for clinical evolution are selectively observed in the group of INDt patients and did not occur within the CARD/DIGt group. However, it is important to mention that the comparative analysis of clinical evolution rates with previously reported historical controls should be performed with caution since several variables (e.g., age, sex and exposition to infected vectors) may vary in different geographical regions. In this context, most of the historical controls used for comparative analysis in our study included patients from both sexes with ages ranging from 17-50 years. Moreover, in general, all historical data came from studies performed in geographical areas where the vectorial re-exposition has been reported to be analogous to the one observed in our study population. We would also like to emphasise that due to its retrospective nature, this study presents some limitations, including the low number of available samples and the lack of an intrinsic control group. Further studies including a larger number of patients are still needed to validate the beneficial impact of specific treatment in chronic Chagas disease. ACKNOWLEDGEMENTS To the municipality of Berilo, for all the facilities offered for developing this study. REFERENCES
Copyright © 2009 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc09229t1.jpg] [oc09229f5.jpg] [oc09229t2.jpg] [oc09229f1.jpg] [oc09229f4.jpg] [oc09229f2.jpg] [oc09229f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}