 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 1, 2010, pp. 103-106 SHORT COMMUNICATIONS Prevalence and genotyping of hepatitis C virus in blood donors in the state of Pará, Northern Brazil Aldemir B Oliveira-FilhoI; Adriana SC PimentaII; Márcia FM RojasII; Márcia CM ChagasII; José Ângelo B CrescenteIII; Deborah M CrespoIV; José Alexandre R LemosI, II, + IInstituto
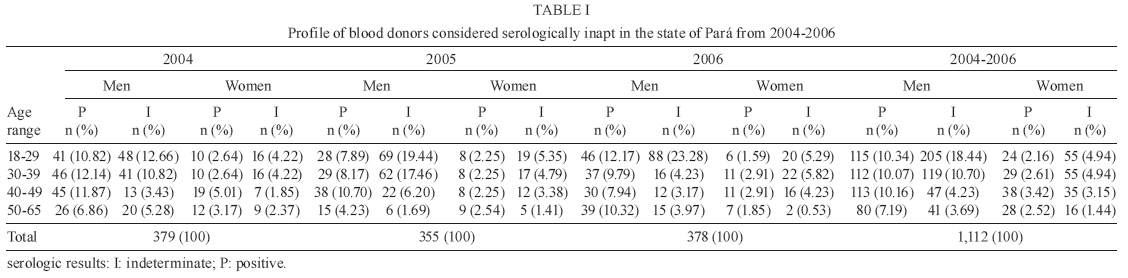
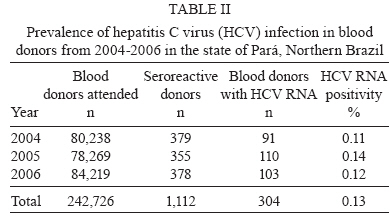
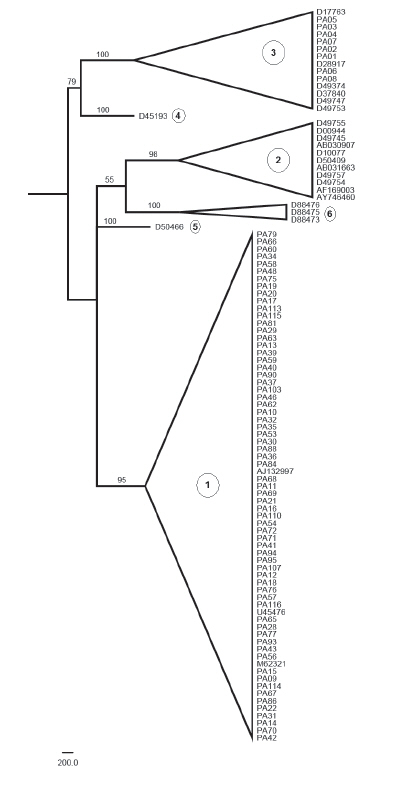
de Ciências Biológicas Financial support: SECTAM, FUNTEC, CNPq, PN-DST/AIDS Received 6 April 2009 Code Number: oc10016 ABSTRACT Given the scarcity of epidemiological information on hepatitis C virus (HCV) infection in Northern Brazil, we determined the prevalence and genotypic frequency in blood donors in the state of Pará (PA). Blood samples from all of the blood donors at the Fundação HEMOPA (blood bank of PA) from 2004-2006 were screened for the presence of antibodies to anti-HCV and samples seroreactive to anti-HCV were further tested for HCV RNA using real-time PCR. In total, 116 HCV-RNA samples were genotyped, based on maximum likelihood phylogenetic analyses, using BioEdit, Modelgenerator, PHYML and FigTree software. The population consisted of 242,726 volunteers who donated blood from 2004-2006; the most common subgroup was males between the ages of 18-29 years old (37.30%). Within the whole group, 1,112 blood donors (0.46%) had indeterminate or positive serology; among these, 28.78% were males whose ages ranged from 18-29 years. A diagnosis of chronic HCV infection was confirmed for 304 donors (60.20% males; 66.45% were 30-49 years old), resulting in a prevalence of HCV RNA in 0.13% of the samples (304 of 242,726). HCV genotyping revealed a high frequency of genotype 1 (108/116) followed by genotype 3 (8/116). This study found HCV infection to be relatively infrequent in PA; genotype 1 was most commonly isolated. This information can help guide prevention and control policies aimed at efficient diagnosis and control measures. Key words: HCV - epidemiology - blood donors - Pará - Northern Brazil Currently, the estimated prevalence of hepatitis C virus (HCV) infection in the world is approximately 2.2% (approximately 130 million); most of the victims are asymptomatic and unaware of their own viral infection (Alter 2007). Official data on the prevalence of HCV in the Brazilian population are limited. It is estimated that the seroprevalence in blood donors is approximately 1.6%, characterizing Brazil as an area with low endemicity (GESBH 1999). However, seroprevalence differs among regions of the country, with the highest rate being in the Northern Region (2.2%). In Northern Brazil, the seroprevalence among blood donors has been determined in the states of Acre (AC) (5.9%), Pará (PA) (0.5-2%), Roraima (1.2%) and Amazonas (AM) (0.8%) (GESBH 1999, Da Fonseca & Brasil 2004). Epidemi-ological studies conducted of indigenous, riverside and immigrant populations in Northern Brazil indicate a range of 0.38-2.4% seroprevalence (Soares et al. 1994, Ferrari et al. 1999, De Paula et al. 2001, Tavares-Neto et al. 2004, El Khouri et al. 2005). The molecular epidemiology of HCV in Northern Brazil is similar to what is known to be present in the rest of the country: a predominance of genotype 1 followed by genotypes 3 and 2. The known genotypic distribution in Northern Brazil is based on HCV strains found in AC and AM (Busek & Oliveira 2003, Campiotto et al. 2005, Paraná et al. 2007). Given the scarcity of epidemiological information about HCV in PA and in Northern Brazil, we determined the prevalence and genotypic frequency of HCV in blood donors in PA, Northern Brazil. We selected blood donors who were recruited by the blood bank of PA (Fundação HEMOPA) during routine blood collection at nine hematology and hemotherapy units and in blood donation campaigns held in public and private institutions in PA from January 1, 2004-December 31, 2006. All of the plasma samples were tested for HCV antibodies using an immunoenzymatic test (Murex anti-HCV version 4.0, Murex Biotech SA, Kyalami, South Africa). A confirmatory test for viral infection was made on the seroreactive samples using real-time PCR (ABI Prism 7000, Applied Biosystems). The viral RNA was extracted using the commercial extraction kit QIAmp Viral RNA Mini Kit (Qiagen). Molecular diagnosis was based on detection of the 67 base pairs of 5' UTR with the commercial kit TaqMan EZ RT-PCR Core Reagents (Applied Biosystems), following the manufacturers protocol, with the addition of the primers DET1 (5'→3':CGCTCAATGCCTGGAGATTT) and DET2 (TTTCGCGACCCAACACTACTC) and the probe PRB (FAM-TGCCCCCGCAAGACTGCTAGC-TAMRA). After molecular diagnosis of viral infection, 116 samples of HCV RNA were randomly selected for amplification of the 5' UTR of HCV using nested-PCR. The first reaction consisted of synthesis and amplification of cDNA in a single step, using the thermocycler GeneAmp PCR System 9700 (Applied Biosystems) and the commercial kit SuperScript One-Step RT-PCR with Platinum Taq (Invitrogen) and following the manufacturers protocol, with addition of 1.0 μL EAP1 (ACACTCCGCCATGAATCACTCCC) and 1.0 μL EAP2 (TGCACGGTCTACGAGACCT). The second reaction mixture consisted of 15.8 μL ultra-pure water, 2.5 μL 10 x PCR buffer, 1.5 μL MgCl2 (50 mM); 1.0 μL dntp mix (G,C,T,A; 10 mM), 0.2 μL Taq polymerase (5 U/μL), 3.0 μL of the product of the first PCR, 0.5 μL IAP1 (GGAACTACTGTCTTCACGCAGAAA) and 0.5 μL IAP2 (ACTCGCAAGCACCCTATCA). The parameters of this second amplification were: 1 cycle: 94ºC/5 min and 60ºC/2 min; 25 cycles: 72ºC/1 min, 94ºC/40 s, 60ºC/30 s; 1 cycle: 72ºC/30 min. The product of this second amplification was run on a 2% agarose gel buffered with TBE; the gel was stained with ethidium bromide and visualised with ultraviolet light. The amplified fragment was sequenced in both directions using the dideoxynucleotide chain terminator method with an ABI Prism 377 and the commercial kit Big Dye Cycle Sequencing Standard, both from Applied Biosystems. All nucleotide sequences obtained were edited and aligned using BioEdit software (http://www.mbio.ncsu.edu/BioEdit/bioedit.htm). The final alignment was submitted to the Modelgenerator software (Keane et al. 2006) to select, according to the corrected Akaike information criterion, the best model to apply to phylogenetic analyses. These parameters were used in the PHYML program version 2.4.4 (Guindon & Gascuel 2003) to infer trees according to the maximum likelihood method. To test the robustness of the tree topologies, 1,000 bootstrap replicates were performed. The final phylogenetic tree was obtained by majority rule consensus and after editing using the graphic resources contained in the FigTree software (http://tree.bio.ed.ac.uk/software/figtree). Nucleotide sequences obtained from the National Center of Biotechnology Information were added to the alignment and used to construct the phylogenetic tree to identify HCV genotypes. The nucleotide sequences obtained in this study were deposited in the National Center of Biotechnology Information (FJ696418-FJ696533). This study was approved by the Ethical in Research Committee of the Núcleo de Medicina Tropical of the Universidade Federal do Pará, Belém, PA, Brazil. From 2004-2006, the Fundação HEMOPA attended to 242,726 voluntary blood donors in PA. The largest group of donors was males ranging in age from 18-29 years (38.29%). Among these, 1,112 (0.46%) were serologically reactive for anti-HCV antibodies (539 positive and 573 indeterminate); this group was predominantly composed of males between 18-29 years old (28.78%). All 1,112 blood donors who were considered inapt for donation were invited to visit one of the nine state hematology and hemotherapy units of the Fundação HEMOPA to perform a confirmatory test. HCV RNA was detected in 304 of these blood donors (13.82% had indeterminate ELISA). These infected donors were mostly males (60.20%) and 66.45% of these infected donors (of both sexes) were from 30-49 years old (30-39 years: 27.63%; 40-49 years: 38.82%) (Table I). Moreover, we observed increasing rates of RNA detection according to the signal-to-cutoff (S/CO) ratio. In summary, the seroprevalence of antibodies to HCV was 0.22% (539 of 242,726) and 0.13% (304 of 242,726) of those tested had detectable HCV RNA (Table II). We also isolated nucleotide sequences of HCV 5' UTR from 116 of these blood donors. Based on the Modelgenerator software, the most adequate evolutionary model for this data matrix was the Tamura-Nei adjusted by the parameters "proportion of invariable sites" (0.540) and "rate of gamma distribution" (0.944). The base frequencies (A = 0.18658, C = 0.30219, G = 0.30683, T = 0.20440), transition/transversion ratio for purines (2.188) and transition/transversion ratio for pyrimidines (3.227) were estimated by the PHYML software during phylogenetic analysis. The phylogenetic tree (Figure) of HCV in the blood donors of PA indicated a significant prevalence of genotype 1 (93%, 108/116), followed by genotype 3 (8/116). The detection and treatment of HCV infected patients are essential public health measures for containing viral transmission (Lavanchy 2009). The low prevalence of HCV infections and the high frequency among infected individuals of genotype 1 gives the local health authorities incentive to establish a hepatitis C prevention and control program, which should include emphasis on the detection and efficient treatment of infected individuals. It was also observed that, though the largest fraction of donors was in the 18-29 year age group, 66.45% of those infected with HCV were from 30-49 years old. This association between HCV RNA and donor age was also observed in blood donors from AM (Torres et al. 2009). This suggests that, in Northern Brazil, older individuals with longer times of exposure to the various infection risks have a greater probability of being infected with HCV. Epidemiological studies on the prevalence of antibodies to HCV have been conducted in certain populations in the Northern region of Brazil (Soares et al. 1994, Ferrari et al. 1999, De Paula et al. 2001, Tavares-Neto et al. 2004, El Khouri et al. 2005). We found a seroprevalence of antibodies to HCV of 0.22%. These figures differ from what was reported in previous studies among blood donors in PA (0.5-2%) (GESBH 1999, Da Fonseca & Brasil 2004), but they confirm that PA can be considered to have low endemicity for infection with HCV (< 2%). Moreover, serological screening of blood donors with low indexes of infection, including HCV, accounts for a substantial percentage of false-positive results with consequent loss of non infected blood components (Garcia et al. 2008). The high number of blood donors with indeterminate serologic results and negative PCR HCV RNA detected in this study exemplifies this problem. This situation may be related to the need for transfusion safety of the blood bank, ruling out blood coming from donors whose serological results show a S/CO less than 1 or between 1-2. This procedure for transfusion safety has been evidenced by the blood bank of AM, Northern Brazil (Torres et al. 2009). Most hepatitis C infections in Brazil are caused by HCV genotypes 1, 2 and 3 (Busek & Oliveira 2003, Campiotto et al. 2005). We found a preponderance of infections by genotype 1 (93%) among blood donors in PA. The HCV genotype most commonly found throughout most of AC and AM was also genotype 1, with percentages of 78% and 64.3%, respectively (Campiotto et al. 2005, Paraná et al. 2007). Based on these results and those of our study, we can conclude that most hepatitis C infections in Northern Brazil are due to genotype 1, with the highest proportion (93%) found in PA. This result implies that patients infected with HCV in PA should preferentially be treated with a specific clinical protocol for genotype 1. Moreover, this study shows the need for sequencing of other regions of the HCV genome for better resolution of viral genetic dynamics in Northern Brazil. In summary, we observed that HCV prevalence among blood donors in PA is low; however, among positive cases, we detected a high frequency of genotype 1. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10016t2.jpg] [oc10016t1.jpg] [oc10016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}