 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 449-453 Clinical and laboratory evaluation of schistosomiasis mansoni patients in Brazilian endemic areas Luciano Fernandes PereiraI, +; Andrei Leite GazzaneoII; Roberta Maria Pereira Albuquerque de MeloIII; Hugo Cabral TenórioIII; Darlan Silva de OliveiraIV; Maria Sonia Correia AlvesI; Danielle Correia GamaI; Rozangela Maria de Almeida Fernandes WyszomirskaIII IInstituto
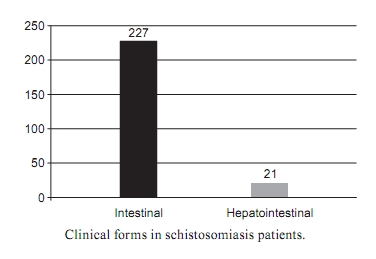
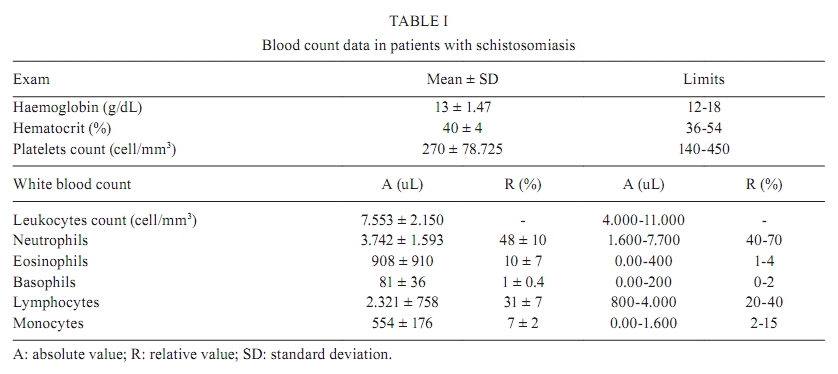
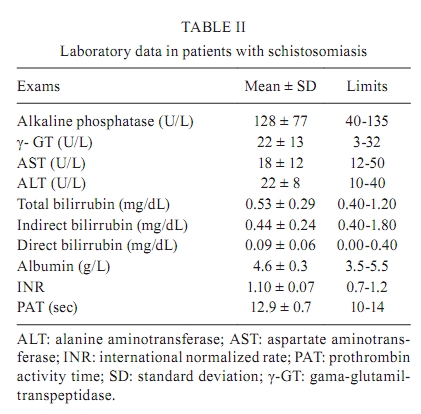
de Ciências Biológicas e da Saúde + Corresponding author: lucianofernandespereira@gmail.com Received 30 December 2008 ABSTRACT A total of 60% of the territory of Alagoas (AL) is considered endemic for the occurrence of schistosomiasis and the classification of clinical forms of the disease are not known. This paper aimed to evaluate an endemic schistosomiasis population in AL, taking into account the prevalence, classification of the clinical forms and the results of laboratory analyses. The sample consisted of residents in endemic areas. The participants were submitted to a stool examination by the Kato-Katz technique and the diagnosis was based on the reading of two microscopic slides for each sample. The patients whose examinations were positive for schistosomiasis mansoni were submitted to a clinical examination and blood collection. Based on this examination, 8.11% of the study population were positive for schistosomiasis. The medium parasite load was 79.1 ± 174.3 eggs. The intestinal (90.57%) and hepatointestinal (9.43%) forms were found at statistically significant levels (p < 0.001). The results of the present study update information on schistosomiasis in the city of Rio Largo. These data, although referring only to three locations in that city, suggest a decrease either in the parasite load or in the severity of clinical forms. Key words: schistosomiasis mansoni - clinical evaluation - laboratory evaluation Schistosomiasis is a disease that affects more than 200 million people distributed in 74 countries, mainly in South America, the Caribbean, Africa and the East Mediterranean, where it reaches countries on the Nile Delta, such as Egypt and Sudan. Among these, 10% present the severe form of the disease and 50-60% of infected people, more than 100 million people, present clinical manifestations of the disease. The disease causes an enormous public health problem that affects a large number of children and young adults in their productive life phase and is responsible for more than 500,000 deaths per year (Capron 1992). In Brazil, according to estimates, schistosomiasis affects almost three million people and approximately 30 million are exposed to the infection because they live in areas of risk. Schistosomiasis transmission occurs in a vast endemic area that extends along the seacoast from Rio Grande do Norte to Bahia, in the Northeast Brazilian Region, to the countryside of Espírito Santo and Minas Gerais, in the Southeast Region. There are also isolated foci in the Federal District and in the states of Pará, Piauí, Goiás, Rio de Janeiro, São Paulo, Paraná, Santa Catarina and Rio Grande do Sul (Passos & Amaral 1998). The former representation of schistosomiasis in Brazil shows that the endemic has lost its predominantly rural character, emerging even more in urban areas of diverse states, according to Amorim et al. (1997), who already made this observation in the 1990s. A prospective study by Graeff-Teixeira et al. (2004) between 1997-2000 demonstrates that the lack of infrastructure, migration and displacement of people from endemic to non-endemic areas are fundamental factors for the outbreak of new foci of the disease. Clinical findings make possible the division of the disease in two phases. First is the acute phase, which includes cercarian dermatitis caused by the penetration of cercarias inside the skin and Katayama fever that may appear 3-7 weeks after an exposure, and is characterised by fever, anorexia, abdominal pain and headaches. The second phase is the chronic phase. Its clinical manifestations vary depending on the parasite localization and the viral load. The chronic phase may present intestinal, hepatointestinal, compensated hepatosplenic and decompensated hepatosplenic forms, with the latter being a main indicator of schistosomiasis severity, particularly in areas where the disease and low socio-economic conditions are prevalent (Kloetzel 1963). The diagnosis is guided by the patient history in an endemic area. This evidence is confirmed by the presence of the Schistosoma mansoni ova in stool samples, serological tests (very useful where the disease transmission is low), rectal and hepatic biopsy, studies of circulating antigen by the ELISA capture method and abdominal ultrasound (Beck et al. 2004). A total of 60% of the Alagoas (AL) territory is considered endemic for schistosomiasis. In this area, there are locations of moderate to high prevalence and more than two million people are exposed to infections here. The present classification level of the parasitosis clinical forms is not known. According to the Schistosomiasis Control Program by the National Health Foundation (Funasa), a recrudescence of the disease is taking place in AL. In the last seven years, there has been a decreasing trend, although in a systematic way, the prevalence is around 9%. In order to reduce regional research and technology inequalities that exist in the country, the Unified Health System's Research Program has supported studies (such as this one) whose purpose is to determine the prevalence of clinical forms of schistosomiasis through laboratory diagnoses in an endemic AL community. Thus, such studies contribute to the implementation of a continued and consistent control program of this parasite that affects the health of the poorest populations. PATIENTS, MATERIALS AND METHODS A transverse and descriptive study was undertaken in the city of Rio Largo, AL, Brazil. Study area - The city of Rio Largo has 309 Km² of area and a population of about 65,432 inhabitants. It is situated on the northeast coast of Brazil and is located 20 km away from Maceió, capital of AL. The study sample includes residents of three Rio Largo locations (Ilha Angelita, Lourenço de Albuquerque and Fazenda Riachão), with moderate prevalence for schistosomiasis. Coprological inquiry - A total of 3,609 stool examinations were made in the Rio Largo Municipal Laboratory from November 2007-August 2008 by the Kato-Katz technique (2 slides of a single sample) (Katz et al. 1972). The result was considered positive if S. mansoni ova were present in at least one of the slides. Inquiry - The positive cases of schistosomiasis were sent to the Rio Largo's Basic Health Unit where they were submitted to an inquiry of the date of birth, sex, educational level, address and other information about sanitary and socioeconomic living conditions. Physical examination - The physical exam was conducted by a physician when unarmed semiological techniques were applied. During abdominal examination, ascites and collateral circulation were searched. Abdominal palpation was performed with patients in the dorsal decubitus during deep breath. A liver was considered to be palpable when it was felt below the costal margins and/or xiphoid appendix by examiner. In addition to the size, the surface (regular and irregular) of the right lobe and the thin or rounded brim of the left lobe were described. A spleen was considered to be palpable when the splenic border was felt below the left costal margin by both examiners. Every patient was weighed and treated with prazi-quantel in the recommended dose of 60 mg/kg for children under 15 years old and 50 mg/kg for adults, both with a single dose. The medication was distributed in 600 mg tablets, dividable in two equal parts. Clinical forms - The clinical forms included the following: intestinal (presence of ova and no hepatomegaly), hepatointestinal (presence of ova and hepatomegaly), compensated hepatosplenic (presence of ova, hepatomegaly and splenomegaly) and decompensated hepatosplenic (presence of ova, hepatomegaly, spleno-megaly and oesophageal varices haemorrhage or ascitis or evidence of jaundice). Laboratory tests - Laboratory screening consisted of a complete blood count and determination of aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, γ -glutamyl transpeptidase ( γ -GT) and bilirubin levels. The prothrombin time and serology for human immunodeficiency virus (enzyme immunoassay) and hepatitis B and C were also determined in every patient at the Laboratory of Clinical Analysis at the Professor Alberto Antunes Hospital of the Federal University of Alagoas (UFAL). Ethics - The study was approved by the Ethical Committee of the UFAL and performed according to the Declaration of Helsinki. All subjects signed a written informed consent form prior to starting the study. Statistical analysis - The data were digitalized in Microsoft Excel. Later, they were analysed by a Chi-square test in the SPSS 16.0 software. A risk α of 0.05 or 5% was fixed and results were considered statistically significant at p < 0.05. RESULTS From 3,069 samples, 249 (8.11%) were positive for S. mansoni with no significant difference observed in relation to the prevalence set up for AL. From these 249 patients, 130 (52.2%) were male (23 ± 13 years, range 5-69) and 119 (47.8%) female (26 ± 17 years, range 1-73). No statistically significant differences were observed between the genera (p = 0.689). Of the schistosomiasis patients, 74 (29.7%) live in Ilha Angelita, 53 (21.3%) in Fazenda Riachão and 122 (49%) in Lourenço de Albuquerque. All these places are located in the city of Rio Largo. Parasite load - The medium parasite load on slide one was 80 ± 193.4 eggs (range 24-2.592) and on slide two was 78.2 ± 156.2 (range 24-1.488). Clinical forms - In relation to the clinical forms, there was a predominance of the intestinal form in 227 cases (91.53%). There was no occurrence of hepato and/or splenomegaly and 21 patients (9.47%) presented palpable hepatomegaly without splenomegaly, characteristic of the hepatointestinal form (Figure). There were no patients with the compensated and/or decompensated hepatosplenic clinical forms. Laboratory analysis - Table I shows the blood count results in patients with schistosomiasis. The mean values of the haemoglobin, platelets and leucocytes counts were lower than the normal values. Anaemia was present in 25 patients (11.9%), low platelets count in four (1.9%) and high eosinophils levels in 154 patients (73.3%). Serum markers for hepatitis B or C were negative in all cases. The laboratory results are presented in Table II. The γ -GT levels were raised in 29 patients (13.8%) and the other exams yielded normal results. DISCUSSION This study was carried out in three Rio Largo locations due to their proximity to the Mundau River, where there is an intense proliferation of the Biomphalaria glabrata mollusc, according to an inquiry made by Funasa in 2003. Therefore, caution is recommended in the interpretation of the data because they come from the records of those locations. The analysed data, however, may contribute to updating the schistosomiasis mansoni information in Rio Largo. The prevalence of schistosomiasis observed in this study was very close to the 9% that is advocated for AL, without any statistical significance (p > 0.05). However, the level was lower than the latest data provided by Funasa in 2003, which established a prevalence of 15.7% in the three localities studied, establishing these regions as having a moderate prevalence according to a scale in the last Technical Communication of the Schistosomiasis Surveillance and Control of AL. There was no statistical difference between the number of men and women among the schistosomiasis patients, suggesting that the sample was homogeneous (p = 0.689). The parasite load presented a mean between the two slides of 79 eggs per gram of faeces, corresponding to a slight infection level in accordance with the classification of the World Health Organization, which establishes the following infection levels: slight from 1-99, moderate from 100-399 and high greater than 400 eggs/g of faeces. According to Coura et al. (1992), the policy of mass treatment of the population during the 1980s in areas considered to have high prevalence and the repeated treatments of re-infections may have contributed to a better control of the morbidity caused by schistosomiasis due to a weaker infection intensity as measured by the low parasite load. Concerning the clinical forms, the intestinal one was present nine times more frequently than the hepatointestinal form, a statistically significant difference (p < 0.001). No patients showed the hepatosplenic clinical form, compensated and/or decompensated. Even today, there is still a discussion about the importance of the parasite load in the determinism of the schistosomiasis hepatosplenic form. The first papers by Pessoa and Barros (1953), Pessoa and Coutinho (1953), Cheever et al. (1965), Kloetzel (1967) and Cheever (1969) called attention to the likely relationship between the infection intensity and the sprouting of the hepatosplenic form of schistosomiasis. Since the 1980s, a relationship between the intensity of the parasite load and the populations' quality of life, as an aggravating factor important in the development of the serious forms of the disease, has been observed (Barreto 1991). According to Barreto and Loureiro (1984), the intensity of the infection is a better indicator of morbidity than the prevalence. Normal blood counts were maintained except for the eosinophil levels, which were elevated in more than two-thirds of the samples, probably due to the stimulus of the proteolytic enzymes produced by the eggs of S. mansoni, in agreement with the literature (Gryseels et al. 2006). The percentage of patients with anaemia and low platelet counts was slightly altered. This may have been caused by the existence of a hepatosplenic form that was not detected in the physical examination by means of liver and spleen exams, which confirms the importance of abdominal ultrasound as a complementary examination to evaluate the presence of hepato-splenomegaly (Marinho et al. 2006). Despite the fact that hepatic schistosomiasis is not characterized by the presence of cholestase strict sensu, there have already been descriptions of serum elevations of hepatosplenic or hepatointestinal forms of cholestatic enzymes of in carrying patients (Barreto 1971). In the present study, the γ -GT was raised in 29 (13.8%) of the patients. Amaral et al. (2002) observed increases of γ -GT values in patients with the hepatosplenic form of schistosomiasis and suggested that γ -GT increases can precede the establishment of the hepatosplenic disease form. According to Ganc (1974), livers of people affected by schistosomiasis presents a disharmonic bile tree with distorted ducts and irregularities in their contours, frequently showing short focal stenoses and micro-nodule impressions that would justify the increase of such enzymes. Paradoxically, Vianna et al. (1989) analysed hepatic biopsies of hepato-splenic schistosomiasis-carrying patients and found lesions of bile ducts (periductal fibrosis, hyperplasia of the ducts epithelium, bile duct degeneration and marginal duct proliferation) in 55.3% of the cases. The variables of the bile duct degeneration and ductal proliferation were related to the presence of the parasite and there was no correlation between the histological findings and the serum levels of enzymes. The present paper presents results that update information about schistosomiasis in Rio Largo. Although these data refer to only three locations of that city, they confirm the occurrence of the disease in the city population. Despite the moderate prevalence found, the parasitic load was low, possibly due to the absence of any policy of mass treatment for the population in the 1980s in areas of high prevalence and also due to the repeated treatments of the re-infections that may have contributed to a better control of the morbidity caused by schistosomiasis. This assumes that more concrete and long-term measures, such as educational health programs and environmental sanitation, which are recognised as having greater efficacy to change the permanent character of the conditions of schistosomiasis transmission, have not yet been implemented by the health politics of Rio Largo. These methods include collection and treatment of the residues, a potable water supply, hydraulic and sanitary facilities, landfills to eliminate hydrical collections where molluscs thrive, drainage, cleaning and rectification of streams and canals, small bridge construction etc. The clinical forms found in this study were the mildest, namely intestinal and hepato-intestinal, justified by the low infection intensity associated with the eosinophilia, which, in an unspecific way, may also be related to the presence of co-infections by geohelminthoses. Finally, the present paper confirms the Funasa data (SESAU 2007) that states a decrease in the positivity of mansonic schistosomiasis. The greatest importance of this paper, however, is to demonstrate in an objective and broad way the true dimension of the clinical forms of the disease where it was studied. This pilot study is feasible and easy to carry out and it must be applied on a wide scale in the city of Rio Largo. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10077t2.jpg] [oc10077t1.jpg] [oc10077f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}