 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 460-466 Correlation of biological serum markers with the degree of hepatic fibrosis and necroinflammatory activity in hepatitis C and schistosomiasis patients Clarice Neuenschwander Lins de MoraisI, +; Bruno de Melo CarvalhoI; Wlademir Gomes de MeloI; Fábio Lopes de MeloI; Edmundo Pessoa de Almeida LopesII; Ana Lúcia Coutinho DominguesII; Norma JucáII; João Roberto Maciel MartinsIII; George Tadeu Nunes DinizI; Silvia Maria Lucena MontenegroI IDepartamento
de Imunologia, Centro de Pesquisas Aggeu Magalhães-Fiocruz, Av. Moraes
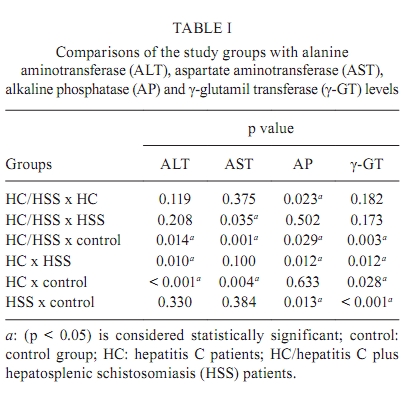
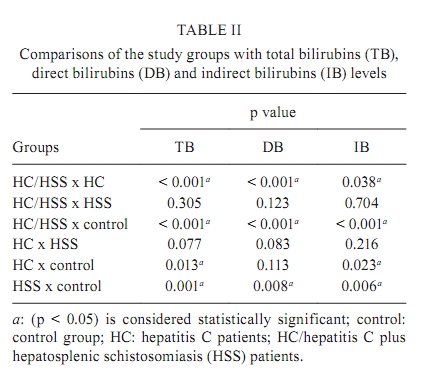
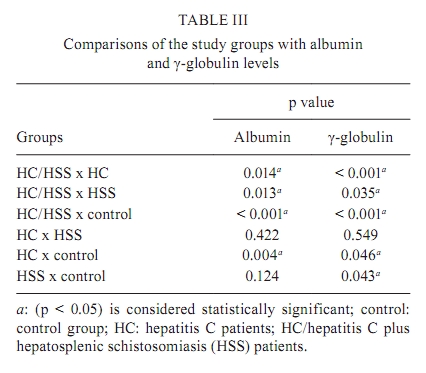
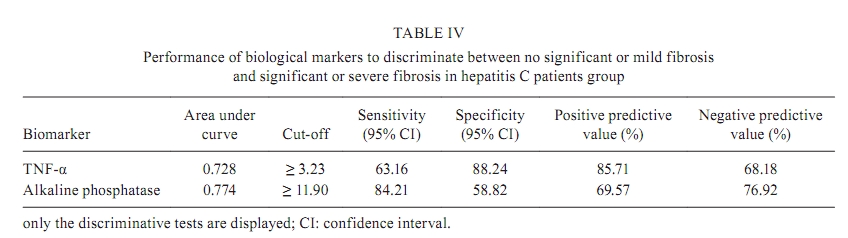
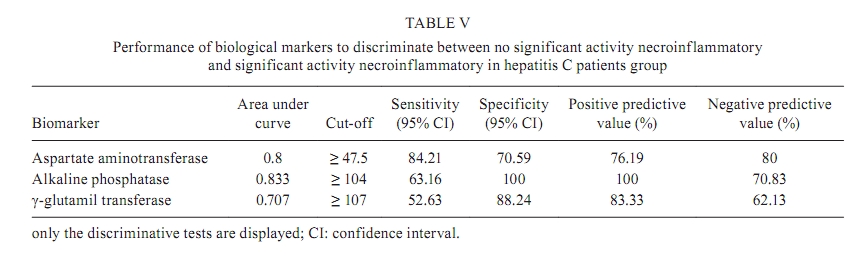
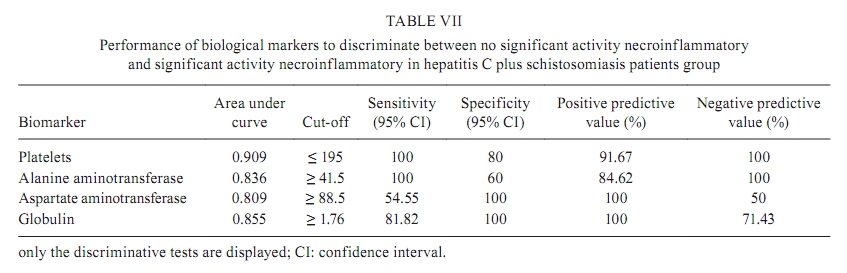
Rego s/n°, 50670-420 Recife, PE, Brasil + Corresponding author: clarice@cpqam.fiocruz.br Received 30 April 2009 Financial support: PAPES V/FIOCRUZ, CNPq (to SMLM) Code Number: oc10079ABSTRACT Liver biopsy is the gold-standard method to stage fibrosis; however, it is an invasive procedure and is potentially dangerous. The main objective of this study was to evaluate biological markers, such as cytokines IL-13, IFN- γ , TNF- α and TGF- β , platelets, bilirubins (Bil), alanine aminotransferase (ALT) and aspartate aminotransferase (AST), total proteins, γ -glutamil transferase ( γ -GT) and alkaline phosphatase (AP), that could be used to predict the severity of hepatic fibrosis in schistosomiasis and hepatitis C (HC) as isolated diseases or co-infections. The following patient groups were selected: HC (n = 39), HC/hepatosplenic schistosomiasis (HSS) (n = 19), HSS (n = 22) and a control group (n = 13). ANOVA and ROC curves were used for statistical analysis. P < 0.05 was considered significant. With HC patients we showed that TNF- α (p = 0.020) and AP (p = 0.005) could differentiate mild and severe fibrosis. With regard to necroinflammatory activity, AST (p = 0.002), γ -GT (p = 0.034) and AP (p = 0.001) were the best markers to differentiate mild and severe activity. In HC + HSS patients, total Bil (p = 0.008) was capable of differentiating between mild and severe fibrosis. In conclusion, our study was able to suggest biological markers that are non-invasive candidates to evaluate fibrosis and necroinflammatory activity in HC and HC + HSS. Key words: biological markers - hepatic fibrosis - HC - schistosomiasis Hepatitis C (HC) disease is an important public health problem, with a high potential for chronicity (85%), cirrhosis and hepatocellular carcinoma (Imbert-Bismut et al. 2001). Hepatocellular damage occurs when the infected cell is recognized by the immune system and destroyed. This process is extremely variable and dynamic, resulting in different intensities of hepatic necrosis and inflammation. Thus, this continuous inflammatory process is responsible for fibrogenesis (Missale et al. 1996, Strauss 2001, Poynard et al. 2003). During HC virus (HCV) infection, male sex, age, alcohol consumption, presence of other viruses (HIV, hepatitis B virus), schistosomiasis and immunological status have been linked to histological severity (Pessione et al. 1998, Kamal et al. 2006). Schistosoma mansoni infection is a chronic helminthic disease that develops primarily because of chronic granulomatous inflammation against parasite eggs in the liver, which results in hepatic periportal fibrosis, portal hypertension and sometimes death by digestive bleeding of esophageal varices, present in the severe hepatosplenic clinical form. Granulomas in schistosomiasis depend predominantly on CD4+ T cells and represent a form of delayed-type hypersensitivity (Abath et al. 2006). Andrade (1962) and Dusek et al. (1965) emphasized that the association between chronic hepatitis and schistosomiasis aggravated liver disease. Blood transfusions secondary to digestive haemorrhage due to schistosomiasis portal hypertension is one of the major causes of HC transmission to schistosomiasis patients in Brazil (Cid et al. 1985). HC and schistosomiasis co-infection is common in many developing countries, including Brazil, and according to Kamal et al. (2004, 2006) shows a specific clinical, virological and histological pattern characterized by virus persistence with high HCV RNA titres and higher necroinflammatory and fibrosis scores in liver biopsies. In addition, these patients exhibit a poor interferon therapy response and accelerated hepatic fibrosis (Kamal et al. 2006). Fibrosis is the major cause of mortality and morbidity related to both schistosomiasis and HC, although the pattern of fibrosis and underlying immunological mechanisms are different (Abath et al. 2006). Liver biopsy is the gold-standard method for the assessment of fibrosis; however, it is an invasive procedure and is potentially dangerous (Imbert-Bismut et al. 2001, Myers et al. 2002, Wai et al. 2003, Poynard et al. 2005). In addition, it is a costly procedure and requires a physician, support staff and an experienced pathologist. Furthermore, a percutaneous liver biopsy can generate sampling errors from the small size of the biopsy and variability in fibrosis interpretation, giving a static view of the necroinflammatory and fibrotic process since a liver biopsy represents only a small part of the whole organ (Lichtinghagen & Bahr 2004). As a result of these limitations, several studies have emerged in an attempt to develop accurate and reliable non-invasive means to assess the severity of hepatic fibrosis in HC patients, since knowledge of the stage of liver fibrosis is essential for prognosis and decisions on antiviral therapy (Imbert-Bismut et al. 2001, Myers et al. 2002, Poynard et al. 2002, 2005, Freeman et al. 2003, Morais et al. 2006, Gressner et al. 2007, Correia et al. 2009). Although there is no indicator of human schistosomiasis in liver biopsy, use of non-invasive biological markers to predict fibrosis severity is important for monitoring the transition to the severe forms of the disease and prognosis of these patients. In the areas where access to health care services is limited, these markers are also essential to evaluate fibrosis regression after treatment (Burchard et al. 1998, Ricard-Blum et al. 1999, Köpke-Aguiar et al. 2002). Most of the studies regarding biological serum markers of fibrosis have focused on HC or schistosomiasis as an isolated disease. The main objective of this study was to correlate levels of biological serum markers with the prediction of clinically significant fibrosis and necroinflammatory activity in HC and schistosomiasis, not only as isolated diseases, but also as co-infections. PATIENTS, MATERIALS AND METHODS Subject selection - This study included 80 patients aged 18-65 years old, selected at the outpatient facilities of the Hospital das Clínicas da Universidade Federal de Pernambuco (UFPE), Recife, Pernambuco (PE), Brazil. The following groups were studied: HC (n = 39); HC plus hepatosplenic schistosomiasis (HSS) (n = 19) and HSS (n = 22). Liver biopsies, ultrasonography, parasitological stool exams and blood tests for biological markers of fibrosis were performed. All patients were tested for hepatitis B (HBsAg and anti-HBc), HIV (anti-HIV) and HCV (anti-HCV) (Gretch 1997). Diagnosis of HC in patients was confirmed by detection of viral RNA (Zeuzem et al. 1994) and genotyping (Stuyver et al. 1996). For schistosomiasis patients, the diagnosis was confirmed by ultrasonography and three parasitological stool examinations. These patients were selected after treatment; however, HC patients were selected before treatment. Patients with the following conditions were excluded from the study: other causes of liver disease, liver transplantation, prior interferon therapy, immunosuppressive therapy, hepatitis B, HIV, insufficient liver tissue samples for staging of fibrosis and alcohol consumption (> 30 g/day). The control group (n = 13), ranging from 21-57 years old, was from non-endemic areas of PE and was selected at Centro de Pesquisas Aggeu Magalhães. These individuals had three negative parasitological stool examinations for S. mansoni, no history of contact with contaminated water and negative anti-HCV. All patients and control group individuals signed an informed consent form and the study was reviewed and approved by the Ethical Committee of the Centro de Pesquisas Aggeu Magalhães-Fiocruz, Recife, PE, Brazil. Fibrosis stage and necroinflammatory activity grade - HC and HC + HSS patients underwent percutaneous liver biopsy at Hospital das Clínicas da UFPE. Histological features of liver biopsy were analysed according to the Metavir scoring system (Bedossa & Poynard 1996). Fibrosis was staged on a scale as follows: F0 (no fibrosis), F1 (portal fibrosis without septa), F2 (few septa), F3 (numerous septa without cirrhosis) and F4 (cirrhosis). The intensity of necroinflammation was graded on a scale as follows: A0 (no activity), A1 (mild activity), A2 (moderate activity) and A3 (severe activity). In addition, HSS and HC + HSS patients had their degree of fibrosis analysed by ultrasonography according to the Cairo scoring system (WHO 1990) as follows: degree I (mild periportal fibrosis), degree II (moderate periportal fibrosis) and degree III (severe periportal fibrosis). Determination of serum levels of biological markers - Blood samples (15 mL) were collected using a vacuum system and disposable needles from all patients and control group individuals for assessing the serum levels of biological markers. In this study, the biological markers were divided into biochemical markers, platelets and cytokines involved with inflammation and fibrogenesis. Determination of serum levels of biochemical markers - The following markers were assessed for the study: alanine aminotransferase (ALT), aspartate aminotransferase (AST), total proteins, bilirubins, γ -glutamil transferase ( γ -GT) and alkaline phosphatase (AP). The serum levels of ALT, AST, total proteins, bilirubins, γ -GT and AP were determined by the ARCHITECT c8000 (Abbott) using Abbott reagent kits at the laboratory of the Hospital das Clínicas da UFPE. Platelet count - Platelet counts were determined using the Cell-Dyn 3500 (Abbott) at the laboratory of the HC-UFPE. Determination of cytokine serum levels - The serum levels of cytokines IL-13, IFN- γ , TNF- α and TGF- β were measured using the enzyme linked immunosorbent assay Quantikine kit (R&D system) following the manufacturer's instructions. Statistical methods - HC and HC + HSS patients were divided into two groups according to the severity of their histological lesions: no significant or mild fibrosis (F0-F1) and significant or severe fibrosis (F2-F4). The primary outcome was the identification of patients with clinically significant fibrosis. This dichotomization was performed because F2 fibrosis is generally considered the threshold for the initiation of antiviral treatment of chronic HC. These patients were also analysed according to the presence of necroinflammatory activity and divided into two groups: no significant activity (A0-A1) and significant activity (A2-A3). HSS and HC + HSS patients were statistically analysed into two groups according to the degree of fibrosis as evaluated by ultrasonography as follows: mild fibrosis (degree I) and severe fibrosis (degrees II and III). The statistical analyses were performed using the software SPSS for Windows version 12.0, 2004 (Chicago, USA). P values of 0.05 or less were considered significant. The ANOVA was used for comparison of serum levels of biological markers between the four study groups. For every biological marker, receiving operating characteristics (ROC) curves were built to establish the best cut-off value that would correlate with severe fibrosis and severe necroinflammatory activity for each group of patients studied. RESULTS Biological serum marker levels - For the HC + HSS group (Table I), serum levels of AST, ALT, AP and γ -GT were higher in comparison to the control group (p = 0.001, p = 0.014, p = 0.029 and p = 0.003, respectively). In addition, the serum levels of AST were higher in comparison to the HSS group (p = 0.035). Also, the AP levels were higher than in the HC group (p = 0.023). Total and direct bilirubins were higher when compared with the HC group and control group (p < 0.001 for both) (Table II). Levels of γ -globulin (Table III) were also higher in the HC + HSS group in comparison to the HC (p < 0.001) and HSS (p = 0.035) groups, as well as the control group (p < 0.001). Albumin levels (Table III) were lower in the HC + HSS group than in the HC group (p = 0.014), HSS group (p = 0.013) and control group (p < 0.001). For the HC group (Table I), ALT levels were higher than in the HSS (p = 0.010) and control groups (p < 0.001). AP and γ -GT were lower than in the HSS group (p = 0.012 for both). In addition, AST levels were higher than in the control group (p = 0.004). Also, γ -GT levels were higher than in the control group (p = 0.028). Total bilirubins (Table II) in the HC group were higher when compared with the control group (p < 0.013) mainly due to indirect bilirubin (p = 0.023). The HSS group compared with control group showed higher levels of AP, γ -GT (Table I), TB (Table II) and γ -globulins (Table I) (p = 0.013, p < 0.001, p = 0.001 and p = 0.043, respectively). Serum levels of the cytokines IL-13, TGF- β , IFN- γ and TNF- α were not significantly different among the study groups (p > 0.05). Correlation of biological serum marker levels to predict severe fibrosis and necroinflammatory activity in HC patient groups - Fibrosis stages and necroinflammatory activity grades obtained through histologies of liver biopsy using the Metavir scoring system were studied as described in the Patients, Materials and Methods section. Our results showed that 47.2% of HC patients had mild fibrosis and necroinflammatory activity and 52.8% had severe fibrosis and necroinflammatory activity. When we compared the area under the curve (AUC) for the ROC of the serum levels of the biological markers in order to predict mild or severe fibrosis, it was found that TNF- α and AP showed statistically significant AUC (p = 0.020 and p = 0.005, respectively). The best diagnostic values of these markers (cut-offs) were reported using sensitivity, specificity, positive predictive value and negative predictive value and are shown in Table IV. For the prediction of severe necroinflammatory activity, AST, AP and γ -GT showed statistically significant AUC. The best cut-off levels and diagnostic values of these markers can be seen in Table V. Correlation of biological marker serum levels to predict severe fibrosis and severe necroinflammatory activity in the HC plus schistosomiasis group - In this group of patients, the gold-standard classification of fibrosis stage was the histology of liver biopsies using the Metavir scoring system, since only a small number of patients had ultrasonography data (5 patients missing data). Our results showed that 31.2% of HC + HSS patients had mild fibrosis and necroinflammatory activity and 68.8% had severe fibrosis and necroinflammatory activity. When analysing the results, we found that total bilirubin showed a statistically significant AUC ROC curves for predicting severe fibrosis (Table VI). In addition, platelets, ALT, AST, total bilirubin and γ -globulin showed statistically significant AUC ROC curves for predicting severe necroinflammatory activity in these patients (Table VII). Correlation of biological marker serum levels to predict severe fibrosis in the schistosomiasis patient group - The degree of fibrosis analysed through ultrasonography using the Cairo scoring system, as described in the Patients, Materials and Methods section, was compared with biological marker serum levels. Of schistosomiasis patients, 90.9% presented with severe fibrosis according to ultrasonography analysis. Platelet counts were used to build ROC curves to predict severe fibrosis in schistosomiasis patients. The results showed no statistically significant AUC ROC curves. The other biological markers could not be analysed due to the small number of patients. Comparative analysis between HC and HC + HSS groups and HSS and HC + HSS groups relative to fibrosis degree - Our results showed no statistically significant differences when we compared the degree of fibrosis among the study groups (p > 0.05). DISCUSSION Hepatic fibrosis in HC and schistosomiasis co-infections can progress to cirrhosis and its complications, such as hepatocellular carcinoma (Köpke-Aguiar et al. 2002, Myers et al. 2002, Shiha & Zalata 2002, Kamal et al. 2006). The assessment of the presence and severity of liver fibrosis is essential in determining treatment strategies, response to treatment, prognosis and the potential risk for complications in patients with chronic liver disease. Liver biopsy, the gold-standard method for diagnosing the severity of necroinflammatory activity and fibrosis, is an invasive tool and it is associated with rare but serious complications, such as bleeding, pneumothorax and perforation of the colon and gallbladder (Thuluvath & Krok 2006). Furthermore, because of its risks, cost and inconvenience, liver biopsy is certainly not the ideal procedure for repeated assessment of disease progression, especially during chronic HC (Castera et al. 2008, Fontana et al. 2008). In light of this, developing non-invasive tests that can accurately predict fibrosis stage and progression over time is a high priority and a growing medical necessity. Among these non-invasive tests are biological markers in serum, used either individually or in combination and alternative imaging techniques, such as ultrasound, magnetic resonance imaging and transient elastography (Sandrin et al. 2003, Ziol et al. 2005, Gressner et al. 2007, Castera et al. 2008). Conventional liver function tests reflect hepatocyte damage as ALT and AST, whereas biliary obstructions can be studied by bilirubin and AP and biosynthetic function by albumin and prothrombin time. Although these tests provide important information on some aspects of liver function, they do not assess the activity of the fibrogenic process, but can indicate the stage of fibrosis (Gressner et al. 2007, Rossi et al. 2007). However, biomarkers that have a direct relation to extracellular matrix protein synthesis or turnover, such as the amino-terminal peptide of III procollagen, are believed to primarily reflect fibrogenesis activity (Gressner et al. 2007). Recent studies suggest that some of these biological serum markers of fibrosis, used in combination to form fibrosis scores, such as Fibrotest and Actitest (Poynard et al. 2002, 2004, 2005), Forns index (Forns et al. 2002) and AST/platelets ratio (Wai et al. 2003), may provide important disease staging information like the presence or absence of advanced fibrosis or cirrhosis. Although widely available, these scores have been found to be poor at predicting intermediate levels of fibrosis and there is a risk of false-positive and false-negative results (Poynard et al. 2005). Most scores were developed and tested in HCV patients and, thus, their extrapolation to non-HCV aetiologies of fibrosis must be considered with caution (Gressner et al. 2007). In this context, this study aimed to evaluate biological serum markers that could be used to predict the severity of liver fibrosis in HC and schistosomiasis as isolated diseases or co-infections. According to Kamal et al. (2004, 2006), patients with HC and schistosomiasis co-infections exhibit higher necroinflammatory and hepatic fibrosis in liver biopsies with a significant hepatic fibrosis progression rate compared with HCV infection alone. They also found that levels of fibrosis markers and cytokines evaluated in this study showed a strong correlation with disease progression. Our results showed no statistically significant differences in fibrosis degree on histology evaluation when fibrosis of HC + HSS patients were compared to HC patients alone. In addition, no statistically significant differences were found comparing fibrosis degree by ultrasonography in HC + HSS and HSS groups. However, higher levels of fibrosis serum markers, such as AST, AP, bilirubin and γ -globulin, were found in HC + HSS patients in comparison with HC and HSS alone, suggesting that these markers could differentiate co-infected from the mono-infected patients (Kamal et al. 2006). In addition, HC patients produced higher levels of ALT in comparison to HSS patients, indicating that necroinflammatory activity and viral replication is present in this infection (Pal et al. 2006). Levels of γ -GT and AP were higher in HSS patients in comparison to HC patients. Increased γ -GT serum levels in HSS patients may be due the presence of granulomas in the hepatic parenchyma. The AP levels in HSS patients are also related to the presence of granulomas in the hepatic parenchyma and distortion of the vasculature (Barreto 1971, Vianna et al. 1989). These granulomas could eventually produce a biliary duct compression by raising the levels of γ -GT and this enzyme could be an early marker of portal hypertension (Martins & Borges 1993, Souza et al. 2000, Köpke-Aguiar et al. 2002). According to our results, γ -GT serum levels were also capable of differentiating between mild and severe necroinflammatory activity in HC patients with a predictive positive value of 83%. An explanation for this association was not found because levels of this enzyme are normally related to severe fibrosis and early cholestasis (Martins & Borges 1993, Imbert-Bismut et al. 2001). Serum levels of the cytokines IL-13, INF- γ , TNF- α and TGF- β were not significantly different among the study groups (p > 0.05). Analysing fibrosis stage and necroinflammatory activity in each group of patients separately, keeping in mind that patients with F2 fibrosis/A2 activity or greater are candidates for antiviral therapy, we found in the HC group that TNF- α and AP could differentiate between mild and severe hepatic fibrosis and that AST, AP and γ -GT could differentiate between mild and severe necroinflammatory activity. TNF- α levels in HC patients have been correlated with hepatic inflammation (Neuman et al. 2002, Kamal et al. 2006) and our study showed the association of this cytokine with severe hepatic fibrosis. AP serum levels could be used as a biological marker for both severe fibrosis and necroinflammatory activity in HC patients. In other studies, AP has also been associated with HC cirrhosis, where fibrosis and inflammation may be more severe (Fontana & Lok 2002). We demonstrated an association between platelet counts and severe activity in HC + HSS patients, with a cut-off level of < 195.000/mm3. A moderate decrease in platelet count is a marker of portal hypertension present in the HSS group and is also a good predictive marker of cirrhosis in HCV infection (Renou et al. 2000, Souza et al. 2000). In conclusion, our results suggest the inclusion of some biological serum marker levels determination in clinical practice, prognosis and management of HC and schistosomiasis patients and this may be helpful for the diagnosis of fibrosis degree and necroinflammatory activity. These may not yet be used as a substitute, but as a tool to avoid repeated liver biopsy. However, currently available biological serum markers should be used with caution since neither single nor sets of markers fulfil the requirements of an ideal non-invasive biomarker of fibrosis that is liver-specific, easy to perform, reliable, reproducible with low inter-laboratory variability and cost-effective. Even the best and most evaluated markers do not meet the criteria of an ideal marker. The future goals of our group are to increase the number of subjects in the HC, HC + HSS and HSS groups and to build a fibrosis index with the markers analysed in this present study to improve diagnostic values and accurately measure the degree of liver fibrosis and necroinflammatory activity in these diseases. Furthermore, we aim to correlate these biological markers with other chronic liver diseases and measure the clinical evolution after treatment. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10079t3.jpg] [oc10079t6.jpg] [oc10079t2.jpg] [oc10079t4.jpg] [oc10079t7.jpg] [oc10079t1.jpg] [oc10079t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}