 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 467-470 Schistosoma mansoni: magnetic resonance analysis of liver fibrosis according to WHO patterns for ultrasound assessment of schistosomiasis-related morbidity Luciana CS SilvaI, +; Luciene M AndradeI, II; Leonardo C de QueirozIII; Izabela VoietaI; Letícia M AzeredoIII; Carlos MF AntunesI; José R LambertucciI IPrograma
de Pós-Graduação em Ciências da Saúde: Infectologia
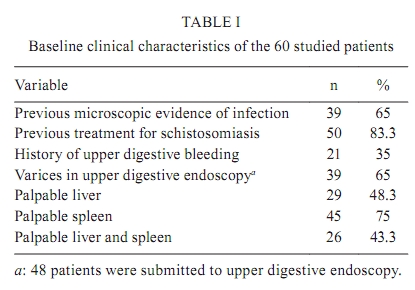
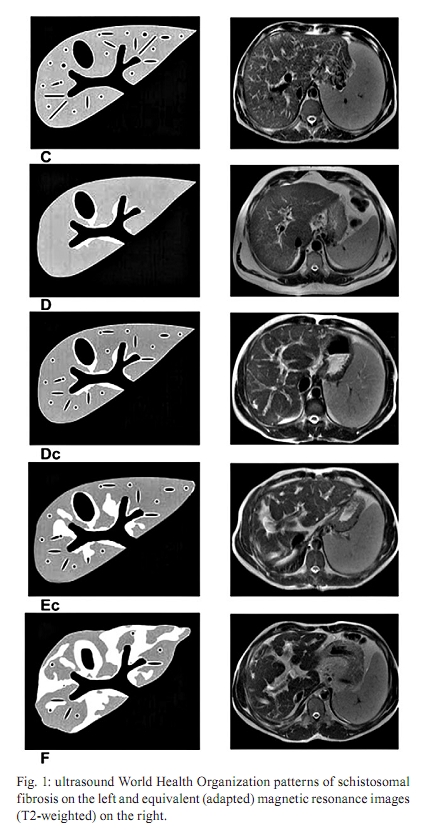
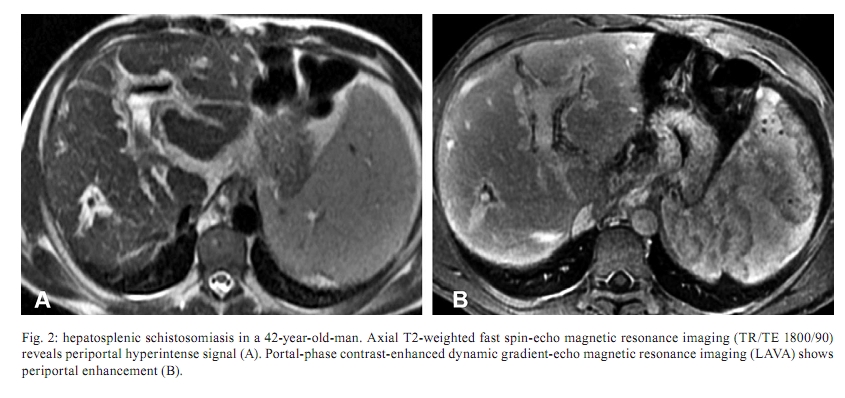
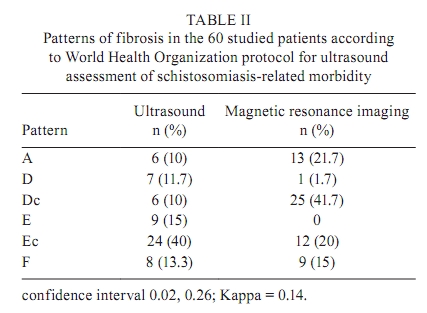
e Medicina Tropical, Faculdade de Medicina + Corresponding author: silva.luciana@ig.com.br Received 10 January 2009 Financial support: CNPq, CAPES Code Number: oc10080ABSTRACT For the last two decades, ultrasound (US) has been considered a surrogate for the gold standard in the evaluation of liver fibrosis in schistosomiasis. The use of magnetic resonance imaging (MRI) is not yet standardised for diagnosing and grading liver schistosomal fibrosis. The aim of this paper was to analyse MRI using an adaptation of World Health Organization (WHO) patterns for US assessment of schistosomiasis-related morbidity. US and MRI were independently performed in 60 patients (42.1 ± 13.4 years old), including 37 men and 23 women with schistosomiasis. Liver involvement appraised by US and MRI was classified according to the WHO protocol from patterns A-F. Agreement between image methods was evaluated by kappa index (k). The correlation between US and MRI was poor using WHO patterns [k = 0.14; confidence interval (CI) 0.02; 0.26]. Even after grouping image patterns as "A-D", "Dc-E" and "Ec-F", the correlation between US and MRI remained weak (k = 0.39; CI 0.21; 0.58). The magnetic resonance adaptation used in our study did not confirm US classification of WHO patterns for liver fibrosis. Key words: schistosomiasis - ultrasound - magnetic resonance - WHO patterns - hepatic fibrosis The gold standard method in evaluating schistosomal hepatic fibrosis was wedge liver biopsy, a safe procedure performed during abdominal surgery, but not justified in non-surgical patients. An alternative procedure, percutaneous liver biopsy, has low sensitivity because it retrieves small and fragmented samples with few portal tracts (Bogliolo 1957, Cheever 1968, Maharaj et al. 1986). For the last 20 years, abdominal ultrasound (US) has become the best tool for the evaluation of liver fibrosis in schistosomiasis mansoni (Lambertucci et al. 1996, Richter et al. 2001). It is an indirect method of diagnosis and classification of the disease (Abdel-Latif et al. 1981, Cerri et al. 1984, Fataar et al. 1984, Homeida et al. 1988, Pinto-Silva et al. 1994, Gerspacher-Lara et al. 1998, Lambertucci et al. 2001). US in hepatosplenic schistosomiasis shows characteristic alterations, such as echogenic thickening of the walls of the portal vein and its branches, corresponding to periportal fibrosis and echogenic enlargement of the gallbladder wall. However, US has disadvantages. Training is necessary for the examiner to apply the World Health Organization (WHO) protocol for US assessment of schistosomiasis (Niamey Working Group 2000) and it is a subjective procedure and, therefore, examiner-dependent. Magnetic resonance imaging (MRI) is a very sensitive imaging technique and, unlike US, is less dependent on the examiner. MRI has been described in hepatosplenic schistosomiasis mansoni (Patel et al. 1993, Willemsen et al. 1995, Lambertucci et al. 2002, 2004, Bezerra et al. 2004, 2007, 2008, Silva et al. 2006), but there is no standardisation of the method in the evaluation of liver periportal fibrosis. The aim of this paper was to analyse MRI using an adaptation of the WHO patterns for US assessment of schistosomiasis-related morbidity. PATIENTS, MATERIALS AND METHODS Patients - The study was approved by the Ethical Review Board of the Universidade Federal de Minas Gerais (UFMG), Brazil, and all study subjects signed the informed consent for participation. Sixty adult patients (37 men and 23 women) with a diagnosis of schistosomiasis from the Infectious Diseases Outpatient Clinic, UFMG, were studied from 2004-2006. Schistosomiasis was defined by microscopic evidence of the infection (positive parasitological stool examination or rectal biopsy) and/or characteristic US signs of periportal fibrosis in a patient exposed to stream waters of an endemic area. Patients included in the study did not have a history of previous surgery for portal hypertension or evidence or vestiges of other causes of chronic liver disease, such as cirrhosis, congestive heart failure and toxic or viral hepatitis. Ages ranged from 19-77 years old (mean 42.1 ± 13.4). Baseline characteristics of the patients are shown in Table I. Methods - Routine outpatient evaluation included clinical examination, abdominal US, blood cell count, assessment of serum albumin, prothrombin, aspartate aminotransferase and alanine aminotransferase levels and serology for hepatitis B and C. US was performed using a real-time device (ALOKA SSD 1700, ALOKA CO, Japan) with an electronic convex 3.5 MHz transducer, according to the WHO protocol for assessment of schistosomiasis-related morbidity (Niamey Working Group 2000). Hepatic fibrosis was classified from patterns A-F, defined as follows: A: normal liver structure; B: "starry sky" (diffuse echogenic foci); C: highly echogenic "ring echoes", which correspond to the "pipe stems" seen in a scan perpendicular to the one where rings are seen; D: highly echogenic "ruff" around portal bifurcation and main stem; Dc: combined D and C patterns; E: highly echogenic "patches" extending from the main portal vein and branches into the parenchyma; Ec: combined E and C patterns; F: highly echogenic "bands" and "streaks", extending from the main portal vein and its bifurcation to the liver surface, causing retraction of the organ surface. MRI was obtained using a 1.5-T unit (GE Sigma unit, General Electric, USA). Axial and coronal 7 mm slice thickness images were acquired in T1 and T2-weighted sequences before and after gadopentetate dimeglumine administration (0.1 mmol/kg) (Magnevist, Bayer Pharmaceuticals, Germany). MRI analysis was adapted from the WHO protocol proposed for US assessment of schistosomiasis-related morbidity (Fig. 1). Two radiologists (one for US and another for MRI) independently examined the images. They were blinded regarding patients' clinical states. Statistical analysis - Agreement between image methods was evaluated by kappa index (k). The degree of agreement was classified as follows: 0.81-1, almost perfect; 0.61-0.8, strong; 0.41-0.6, moderate; 0.21-0.4, fair; 0-0.2, poor. RESULTS Of the 60 patients in the study, US and MRI identified periportal thickening in 54 (90%) and 47 (78.3%) cases, respectively. MRI fibrosis was characterised by hypointense periportal bands on T1-weighted images, which were hyperintense on T2-weighted images (Fig. 2). Periportal enhancement after injection of paramagnetic contrast material was observed in 41 out of 47 (87.2%) patients. US image patterns were classified according to WHO orientations as follows (Table II): A, n = 6 (10%); D, n = 7 (11.7%); Dc, n = 6 (10%); E, n = 9 (15%); Ec, n = 24 (40%) and F, n = 8 (13.3%). MRI patterns were classified as follows: A, n = 13 (21.7%); D, n = 1 (1.7%); Dc, n = 25 (41.7%); Ec, n = 12 (20%) and F, n = 9 (15%). The correlation between US and MRI was poor using WHO patterns in schistosomiasis [k = 0.14; confidence interval (CI) 0.02; 0.26]. Even after grouping image patterns as "A-D", "Dc and E" and "Ec and F", the correlation between US and MRI remained fair (k = 0.39; CI 0.21; 0.58). DISCUSSION In the present study, US and MRI presented a poor correlation in classifying liver fibrosis according to the WHO patterns for US assessment of schistosomiasis-related morbidity. After grouping image patterns, the correlation barely improved to fair. Therefore, the magnetic resonance adaptation used in our study did not confirm US classification of WHO patterns for liver fibrosis. MRI identified schistosomal fibrosis as hyperintense periportal bands on T2-weighted images and hypointense on T1-weighted images with enhancement after contrast, in accordance with previous reports and studies (Patel et al. 1993, Willemsen et al. 1995, Lambertucci et al. 2002, 2004, Bezerra et al. 2004, 2007, 2008). Efforts to establish procedures for US evaluation of schistosomiasis have been published since the early 1990s (Cairo Working Group 1992, Niamey Working Group 2000). In 2000, the WHO published a protocol for US performance and analysis in the evaluation of schistosomiasis-related morbidity (Niamey Working Group 2000), based on previous studies. In the protocol, recommendations to assess periportal fibrosis, portal hypertension and liver and spleen enlargement were established. However, the quantitative assessment of periportal thickness of portal vein walls, particularly of the secondary branches, proved to be difficult in everyday use. In addition, it is considered time-demanding and complex, leading to low reproducibility (Thomas et al. 1997, Yazdanpanah et al. 1997, Hoffmann et al. 2001, Richter et al. 2001, Ruiz et al. 2002, King et al. 2003). Besides the quantitative evaluation, an additional qualitative method for assessing periportal fibrosis was proposed, comparing the observed liver texture with a series of standard reference patterns. The qualitative proposal was expected to define morbidity promptly. Even though the method is simple to use, small nonspecific alterations were mistakenly interpreted as abnormal (for example, patients with depleted liver glycogen due to prolonged fasting were diagnosed as having periportal thickening). Major observer-related discordances have also been reported. In a patient without portal hypertension and with intense periportal thickening diagnosed by US, MRI described a normal liver (Silva et al. 2006). In fact, MRI identified fat tissue around the main portal vein that was seen as fibrosis by US. Therefore, in patients with periportal thickening without portal hypertension, US must be confirmed by MRI. MRI has been used in a variety of liver diseases and its value has been proven. In schistosomiasis, there were only reports of cases or series of cases describing characteristic alterations, but without classification of liver fibrosis. This study is the first to classify schistosomal periportal fibrosis intensity using MRI. The use of WHO US patterns as a guide did not result in sufficient agreement to be recommended. Our results indicate that new patterns should be constructed to better reflect MRI findings. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10080f2.jpg] [oc10080t1.jpg] [oc10080t2.jpg] [oc10080f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}