 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 471-478 Serum hyaluronan and collagen IV as non-invasive markers of liver fibrosis in patients from an endemic area for schistosomiasis mansoni: a field-based study in Brazil Carolina Coimbra MarinhoI, +; Thales BretasIII; Izabela VoietaI; Leonardo Campos de QueirozI, IV; Raiza Ruiz-GuevaraII; Antônio Lúcio TeixeiraIII; Carlos Maurício AntunesI; Aluízio PrataII; José Roberto LambertucciI IPrograma
de Pós-Graduação em Ciências da Saúde, Infectologia
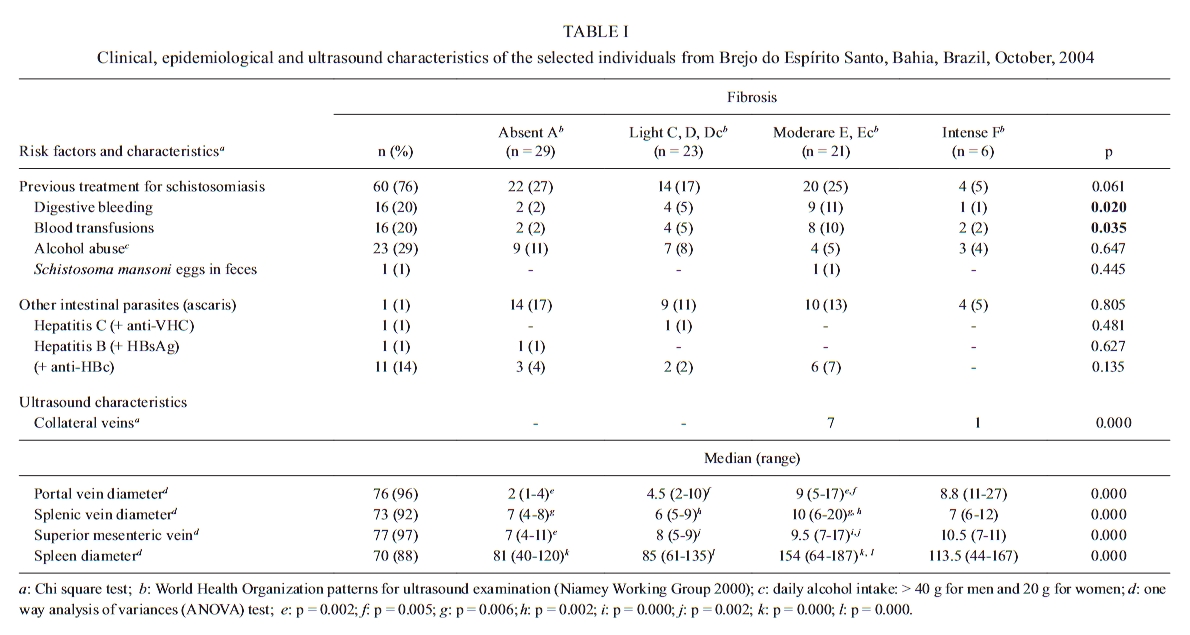
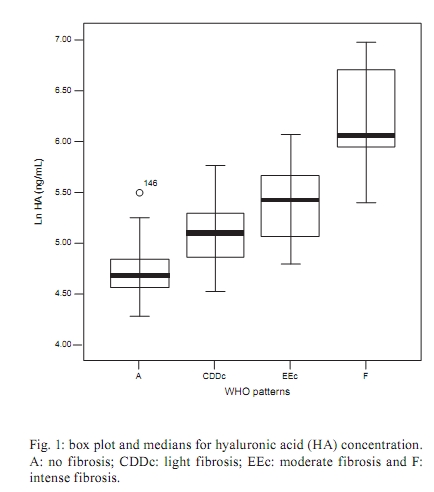
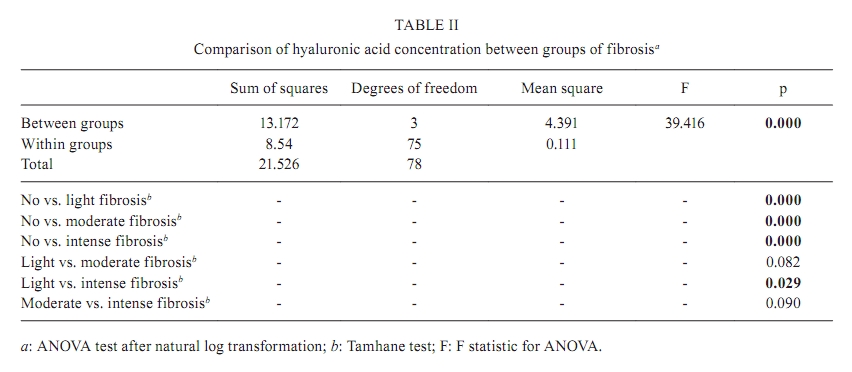
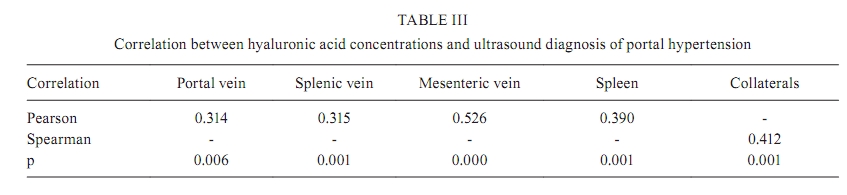
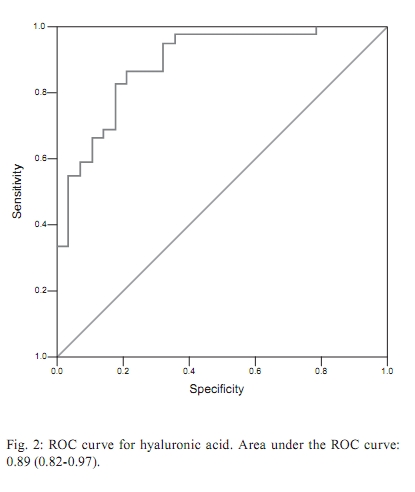
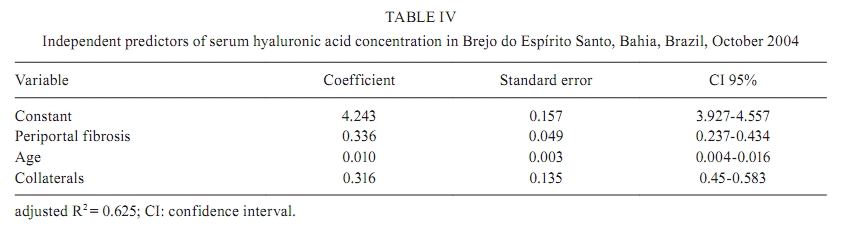
e Medicina Tropical + Corresponding author: carolinacmarinho@gmail.com Received 6 January 2009 Financial support: FAPEMIG, CNPq, FMTM Code Number: oc10081ABSTRACT Non-invasive markers of fibrosis have been used to diagnose liver fibrosis in a variety of diseases. Hyaluronic acid (HA) and collagen IV (C-IV) levels were measured in the sera of patients from an endemic area for schistosomiasis in Brazil to diagnose and to rank the intensity of liver fibrosis. Seventy-nine adult patients with schistosomiasis, in the age range of 21-82 years (49 ± 13.4) were submitted to clinical and ultrasonographic examinations. Ultrasound was employed to diagnose and categorise liver fibrosis according to World Health Organization patterns. Serum HA and C-IV levels were measured using commercial ELISA kits. Ultrasound revealed six patients with intense liver fibrosis, 21 with moderate, 23 with light and 29 without. Serum HA was able to separate individuals with fibrosis from those without (p < 0.001) and light from intense fibrosis (p = 0.029), but C-IV was not (p = 0.692). The HA diagnostic accuracy for fibrosis was 0.89. The 115.4 ng/mL cut-off level diagnosed patients with fibrosis (sensitivity 0.98, specificity 0.64). HA correlated positively with portal hypertension. Periportal fibrosis (subjective evaluation), age and collateral circulation predicted HA increase. In conclusion, we propose that serum HA can be used to identify patients with liver fibrosis in an endemic area for schistosomiasis mansoni in Brazil. Key words: schistosomiasis - ultrasound - liver fibrosis - hepatosplenic schistosomiasis - fibrosis markers Schistosoma mansoni eggs are continuously trapped in the liver. They are surrounded by granulomatous inflammatory reactions that eventually lead up to portal branch obstruction. The consequence is chronic deposition of collagen in periportal spaces, seen as fibrous plaques, while liver architecture is considerably preserved (Bogliolo 1957, Lambertucci 1993, Andrade et al. 1997, Lambertucci et al. 2001, Andrade 2004, Gryseels et al. 2006). The correspondent clinical manifestation, hepatosplenic schistosomiasis, includes portal hypertension and its complications - splenomegaly, collateral circulation, oesophageal varices and ultimately, death from variceal bleeding. Abdominal ultrasound has been compared to liver biopsy and proved useful in the diagnosis of liver injury in schistosomiasis (Homeida et al. 1988, Abdel-Wahab et al. 1989). Considered a simple, safe and low-cost method, after the advent of portable equipment, it has been of invaluable help in the screening of populations living in endemic areas and in field-based studies of the disease. Taken as a nearly ideal tool in the diagnosis and classification of schistosomiasis, it is now used as a surrogate for the gold-standard in the diagnosis of schistosomiasis-related liver fibrosis (Doehring-Schwerdtfeger et al. 1989, Abdel-Wahab et al. 1992, Richter et al. 1992, Abdel-Wahab & Strickland 1993, Pinto-Silva et al. 1994, Richter 2000, Kariuki et al. 2001, Cota et al. 2006, Marinho et al. 2006, Ruiz-Guevara et al. 2007). Fibrogenesis in the liver arises from the activation of hepatic stellate cells. The activated cell proliferates and undergoes phenotypical transformation to acquire the myofibroblast phenotype, which provides it with the migration and secretory properties of a myofibroblast. In addition to collagenous and non-collagenous matrix components, myofibroblasts produce and secrete matrix degradation enzymes and pro-fibrotic cytokines, thus promoting environment modification, amplification and perpetuation of fibrogenesis (Gressner & Bachem 1990, Friedman 1993, Gressner 1998, Friedman 1999, 2000, Kisseleva & Brenner 2007). Stellate cell activation is a common response to various mechanisms of injury, like necrosis, inflammation or peroxidation. It is started and mediated by cytokines and growth factors produced by most cell types present in the liver: inflammatory cells, endothelial cells, platelets, injured liver parenchymal cells and previously activated stellate cells (Nakatsukasa et al. 1990, Friedman 1993, Blazejewski et al. 1995, Friedman 1999). Evolving knowledge of liver fibrosis pathophysiology (Grimaud 1987, Friedman 1993), allied to advances in laboratory methods for quantification in body fluids, led to the identification of useful markers of liver fibrosis activity. Examples exist of different chemical specialties, such as hyaluronan (HA), a glycosaminoglycan, the glycoproteins laminin and YKL-40, collagenous molecules, such as collagen (C) types I, III, IV and V, the metalloproteinase enzymes and their tissue inhibitors, the cytokine TGF-ß. Many of them have been tried and have proved useful in the diagnosis and grading of liver fibrosis secondary to several conditions, including chronic viral hepatitis, alcoholic cirrhosis, non-alcoholic steatohepatitis and schistosomiasis (Stone 2000, Afdhal & Nunes 2004, Grigorescu 2006). However, their ability to identify liver fibrosis in schistosomiasis, when applied to population-based studies in endemic areas, deserves further investigation. In this paper, we compare the serum levels of two non-invasive markers of fibrosis, HA and C-IV, to ultrasound diagnosis of liver fibrosis, in a highly endemic area for schistosomiasis in the state of Bahia (BA) in Brazil. The main objective was to determine the importance of those markers as a screening procedure to identify patients with liver fibrosis in endemic areas for schistosomiasis mansoni. PATIENTS, MATERIALS AND METHODS Patients - A total of 3,766 subjects from Brejo do Espírito Santo, a rural community of Santa Maria da Vitória, BA, Brazil, were examined every four years since 1976 by one of the authors of this paper (AP). The prevalence of schistosomiasis, determined by parasitological stool examinations (Katz et al. 1972), was 75% in 1976. After the implementation of disease control measures, a significant improvement occurred and the prevalence of schistosomiasis dropped down to 1.8% by 2004 (Ruiz-Guevara 2005). In October 2004, 79 individuals were selected and invited to participate in this cross-sectional study. Subjects were submitted to clinical and ultrasound examination. Serum samples were obtained from all participants and stored at -20ºC until transportation to Belo Horizonte, Minas Gerais (MG) where processing took place. Besides HA and C-IV levels in serum, serological tests for viral hepatitis - HBsAg, anti-HBc (HBS and anti-HBc EIA, Medical Biological Service, Milano, Italy) and anti-HCV (Detect-HCV 3.0, Adaltis, Montreal, Canada) - were performed. Liver cirrhosis was excluded by ultrasound examination. Liver fibrosis was diagnosed and graded according to ultrasound classification following the World Health Organization (WHO) patterns for liver fibrosis in schistosomiasis mansoni (Niamey Working Group 2000). The information was stored in a databank especially elaborated for this study, using the appropriate software (Epi Data, http//www.epidata.dk). Physical examination - Physical examination was conducted by two of the authors of this paper (AP, JRL). Discordant patients were re-examined and a consensus was reached in all cases. Abdominal palpation was performed with patients in the dorsal decubitus, during deep breath. The liver and spleen were sought below the costal margins and when palpable, their lengths were measured. Ultrasound - Sonographic examination was conducted by a radiologist trained in the application of the Niamey protocol (Niamey Working Group 2000). One portable GE Logic Book (GE Healthcare, Chalfont St. Giles, UK) was used with a 2.5-5 MHz multifrequency convex transducer, which allows storage of raw data in Dicom format for future re-evaluation. Subjects were allocated in four groups according to ultrasound classification: (i) no fibrosis, including those classified as WHO pattern A, (ii) light fibrosis, composed of those classified as C, D or Dc, (iii) moderate fibrosis, with those classified as E or Ec and (iv) intense fibrosis, with patients classified as F. HA and C-IV - The serum fibrosis markers were both tested using commercially available ELISA kits, in accordance with the manufacturer's recommendations (HA-ELISA® and Collagen IV ELISA®, Echelon Biosciences Inc, Salt Lake City, EUA). Statistical analysis - Data analysis was performed using SPSS 12.0 for Windows (SPSS Inc, Chicago, EUA, 2005). The significance level of 0.05 was considered throughout the analysis. Continuous variables were described as mean (± standard deviation) or median (25-75%) and compared using Student's t or Kruskal-Wallis tests, as appropriate. Chi-square was used for comparison of categorical variables. Comparison between groups was accomplished using the ANOVA test after natural logarithm transformation of variables with non-normal distributions. Differences between groups were sought with the Tamhane test for non-parametric data. A global test accuracy and cut-off value was determined through the analysis of the area under the ROC curve (AUC). Pearson and Spearman coefficients were employed for correlations, as appropriate. Linear regression modelling was employed for multivariate analyses. Clinical and ultrasound variables with significance levels up to 0.20 were included. The clinical variables included were as follows: liver to right costal margin, liver to xiphoid process and spleen to left costal margin distances. The ultrasound variables included were as follows: left and right liver lobe length, spleen length, portal, splenic and superior mesenteric vein diameters, periportal fibrosis (subjective evaluation), WHO patterns of fibrosis, gallbladder wall thickness, periportal thickness in the hilum and on first and second order branches. Data was also adjusted by age and body mass index (BMI), based on literature evidence of HA variations with aging and non-alcoholic steatohepatitis (Fraser et al. 1997, Sakugawa et al. 2005, Suzuki et al. 2005). Ethics - This study was approved by the Ethical Board of the Universidade Federal de Minas Gerais. All participants had given written authorisation at the time of inclusion in the study, following the recommendations contained in the Helsinki protocol (WMA 1964). RESULTS Of those included, 38 of the 79 individuals were male (47.5%). The ages ranged from 21-82 years (49 ± 13.4) and the mean BMI was 22.1 (± 3.0). Twelve (15%) were white (skin colour), as per observer. Digestive bleeding and blood transfusions were more frequently reported in patients with more intense fibrosis (Table I). Ultrasound - A comparison between groups of fibrosis showed statistically significant differences for the presence of collateral circulation, spleen, portal, splenic and mesenteric vein diameters. In sum, six patients (2 with light and 4 with moderate fibrosis) had previously undergone a splenectomy, two patients (1 with moderate and 1 with intense fibrosis) had portal vein thrombosis, three individuals without fibrosis had steatosis and five (1 light and 4 moderate fibrosis) had a heterogeneous liver. In addition, one patient with moderate fibrosis had abdominal lymph node swelling. Clinical, epidemiological and ultrasound data are summarised in Table I. HA - Serum HA levels ranged from 72.3-1.074.9 ng/mL [152.6 (117.0-230.1) ng/mL]. A comparison of medians revealed statistically significant differences between individuals without fibrosis and all groups of fibrosis (p < 0.001) as well as between light and intense fibrosis (p = 0.029) (Fig. 1, Table II). HA had a positive and significant correlation with an ultrasonographic diagnosis of portal hypertension (Table III). AUC (CI 95%) for HA was 0.89 (0.82-0.97) for diagnosing fibrosis (Fig. 2). A concentration of 115.4 ng/mL identified patients with fibrosis, with a sensitivity of 98% and a specificity of 64%. Independent predictors of an increase in the HA level were periportal fibrosis (subjective radiologist evaluation), age and collateral circulation. The constant, variables, regression coefficients and significance levels are depicted in Table IV. C-IV - Serum levels of C-IV ranged from 234.8-1.549.4 ng/mL (798.5 ± 300.9 ng/mL). A comparison of means between groups did not show a statistically significant difference (p = 0.692). DISCUSSION In this study, patients with liver fibrosis presented high serum levels of HA. No correlation was found between C-IV levels and the presence or grade of fibrosis in our patients. Serum levels of HA might not express fibrosis activity and extracellular matrix production in the liver. This point has been addressed by Torre et al. (2008). They have tested serum samples collected simultaneously from the peripheral and hepatic veins during portal venous system hemodynamic investigation in 15 patients. The results showed an excellent correlation between hepatic and peripheral levels for HA (r = 0.971; p < 0.00001) and other markers. This information, together with the consistently good correlation of HA levels and fibrosis in imaging and histological studies, lead us to accept serum levels as a marker of liver fibrosis in pertinent contexts. The serum HA level has been compared to ultrasound diagnosis of liver fibrosis in schistosomiasis mansoni with inconsistent and even contradictory results. Ricard-Blum et al. (1999) found a good correlation between HA and ultrasound scores of fibrosis in an endemic area for schistosomiasis in Madagascar. Burchard et al. (1998) found no correlation and suggested that the increase of serum HA levels was actually related to inflammatory activity or liver function alterations that are absent in schistosomiasis, rather than to fibrosis itself. Yet, WHO patterns for ultrasound in schistosomiasis (Niamey Working Group 2000) have not been employed in the investigation of non-invasive markers of fibrosis. An increase in HA levels during liver parenchyma inflammation has been investigated in viral hepatitis patients with or without schistosomiasis. The results have demonstrated that serum HA concentrations preferably correlate with fibrosis, even when concurrent inflammatory activity exists (Pascal et al. 2000, Tao et al. 2003, Eboumbou et al. 2005, Zheng et al. 2005). Köpke-Aguiar et al. (2002) evaluated serum HA in the diagnosis of hepatosplenic schistosomiasis using the ROC curve analysis. HA was considered a useful marker of portal hypertension caused by schistosomiasis, as it had a diagnostic efficacy of 0.78. Herein, we found that HA correlated positively with an ultrasound diagnosis of portal hypertension. The best HA diagnostic accuracy, however, was found for the identification of fibrosis. Fibrosis is a consequence of immune modulation and tissue repair of the egg-induced granulomatous reaction in vascular and perivascular tissue (Lenzi et al. 1998, 1999, Wynn et al. 2004). HA clearance has been reported to rely on endothelial function (Fraser et al. 1986). A high HA serum concentration in patients with fibrosis might actually signal declining endothelial function due to vascular obstruction by schistosoma eggs and chronic inflammation. Likewise, portal hypertension might represent a consequence of the same process, thus leading to a positive correlation with HA concentrations. The commercial competitive ELISA assay we used counts on industrial standards and has the advantage of not using radioactive reagents, as in the radiometric assays previously employed (Burchard et al. 1998, Ricard-Blum et al. 1999). Köpke-Aguiar et al. (2002) used an in house-developed sandwich ELISA test. The 20 μ g/L cut-off point they have reported differs from the one we found, 115.4 ng/mL. Discordances may be attributed to the assay methods. Notwithstanding, differences in diagnostic accuracy must be interpreted with caution. HA is a main component of extracellular matrix, which increases substantially during fibrosis of any aetiology (Friedman 2003). Hence, in the present paper, the ability of HA to diagnose fibrosis in the endemic area was tested by comparing it to ultrasound. The smaller accuracy of HA to identify portal hypertension suggests that the clinical features may not be directly determined by, although positively correlated to, the amount of liver fibrosis. To our knowledge, there is no study comparing serum HA to liver histology in human schistosomiasis mansoni. However, such a comparison has been carried out by others for different liver diseases. Their results were consistent and reliable for diagnosis of the presence and intensity of fibrosis in viral hepatitis (Guéchot et al. 1996, Zheng et al. 2002), alcoholic cirrhosis (Parés et al. 1996, Stickel et al. 2003) and non-alcoholic steatohepatitis (Sakugawa et al. 2005, Suzuki et al. 2005). Nevertheless, in the present paper, serum HA was not able to detect fibrosis progression. Studies comparing histology and ultrasound, albeit presenting reliability for the ultrasonographic diagnosis of the presence of fibrosis, have also pointed to the inaccuracy of the method in grading the intensity of fibrosis (Homeida et al. 1988, Abdel-Wahab et al. 1992, Voieta 2008). There is no consensus on the use of ultrasound as a gold-standard for the diagnosis of liver fibrosis in schistosomiasis (Lambertucci et al. 2000, 2001, 2008). A recent investigation comparing ultrasound to magnetic resonance and liver histology further revealed drawbacks of ultrasound diagnosis and grading of Symmers fibrosis (Lambertucci et al. 2002, 2004, Silva et al. 2006, Voieta 2008). Magnetic resonance, however, demands resources unavailable in most endemic countries and large scale liver biopsy in field-based studies contradicts elementary ethical principles. In addition, percutaneous liver biopsy itself carries its own technical shortcomings, which are related to the variability and reproducibility of results (Afdhal 2004, Cheung et al. 2008). Serum C-IV has been used to diagnose liver fibrosis in diseases that evolved with sinusoid capilarisation (Hiramatsu et al. 1995, Murawaki et al. 2001, Pereira et al. 2004, Santos et al. 2005, Halfon et al. 2006, Yoneda et al. 2007). Comparing serum C-IV levels between groups, according to the clinical classification of patients with mansonic and hematobic schistosomiasis, Shahin et al. (1992) found high serum levels in patients with hepatosplenic schistosomiasis. In Tanzania, a correlation between serum C-IV and clinical and sonographic signs of hepatosplenic schistosomiasis was observed, but it did not have enough sensitivity to be useful as a screening tool for fibrosis (Kardorff et al. 1999). Two independent groups in China found C-IV to be higher in subjects infected with Schistosoma japonicum (Guangjin et al. 2002) and to correlate with re-infection after treatment of schistosomiasis japonica with praziquantel (Li et al. 2000). Wyszomirska et al. (2005, 2006) investigated C-IV for the detection of schistosomiasis-related liver fibrosis in a tertiary care hospital in Brazil. Patients had higher levels than controls. Nevertheless, significant differences were found only in patients with hepatosplenomegaly and complications of portal hypertension. In further investigation of those patients who underwent a splenectomy, the authors reported a reduction of pre-surgical levels, suggesting that C-IV expression and deposition in the liver may be influenced by the spleen. However, as in the present paper, no correlation was found between serum C-IV levels and ultrasound diagnosis of fibrosis. We speculate that the high frequency of previous splenectomy in patients with moderate and intense fibrosis in the present paper may have hindered the identification of an increase in serum C-IV levels in parallel with the intensity of liver fibrosis. We conclude that HA has a place in the diagnosis of schistosomiasis-related liver fibrosis in field-based studies. C-IV did not identify liver fibrosis in the study subjects. A comparison of serum markers of fibrosis to histology and to magnetic resonance in selected cases will shed light on their role in the diagnosis of liver fibrosis. HA may be used as a screening test to select patients with fibrosis and, hence, direct diagnostic resources to individuals with the highest chances of having hepatosplenic schistosomiasis. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10081t2.jpg] [oc10081f1.jpg] [oc10081t4.jpg] [oc10081t3.jpg] [oc10081t1.jpg] [oc10081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}