 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 479-484 Ultrasound in schistosomiasis mansoni Rogério Augusto Pinto-SilvaI, +; Leonardo Campos de QueirozI, II; Letícia Martins AzeredoI; Luciana Cristina dos Santos SilvaII; José Roberto LambertucciI, II IServiço
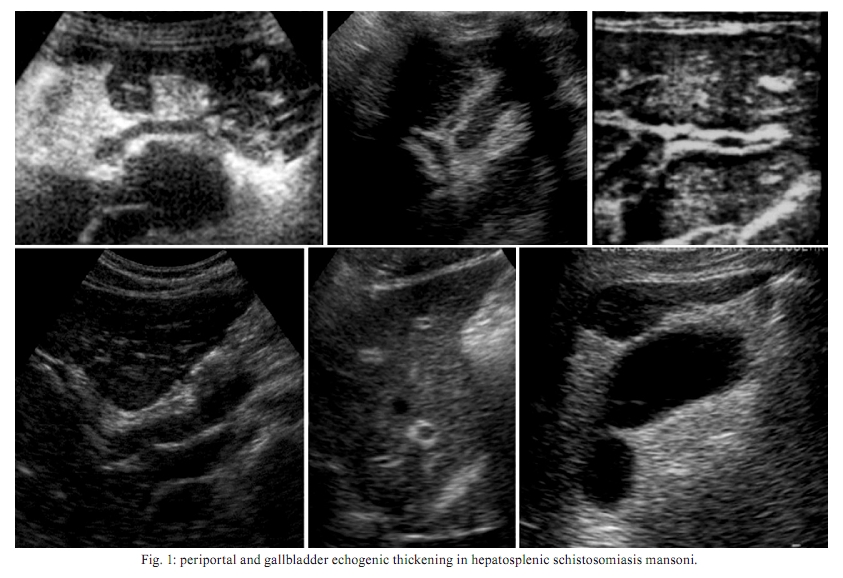
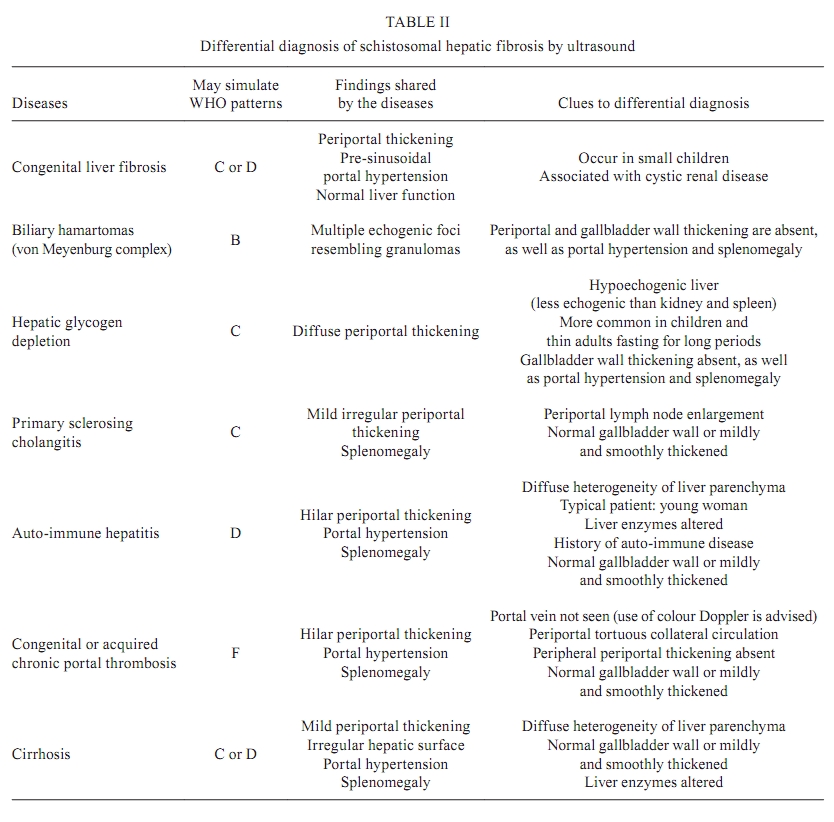
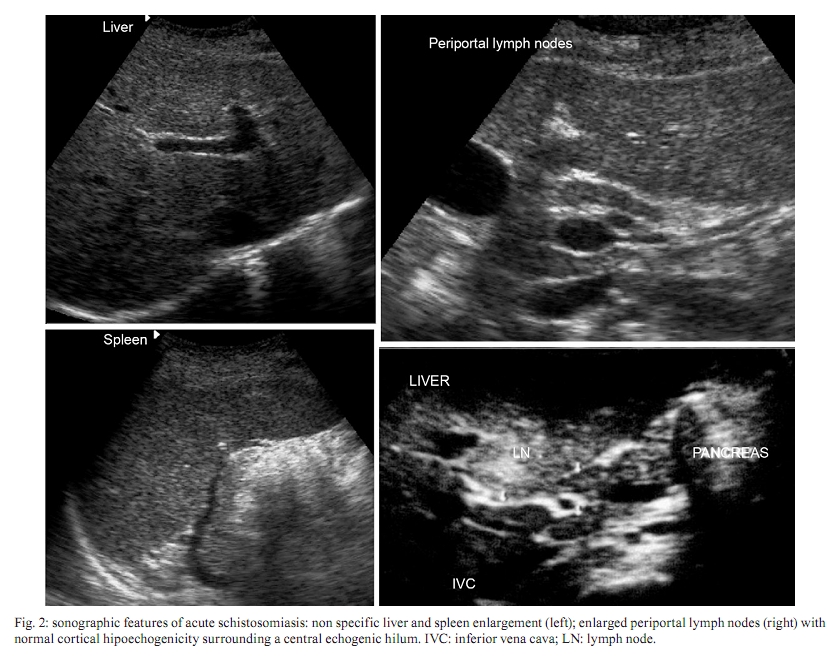
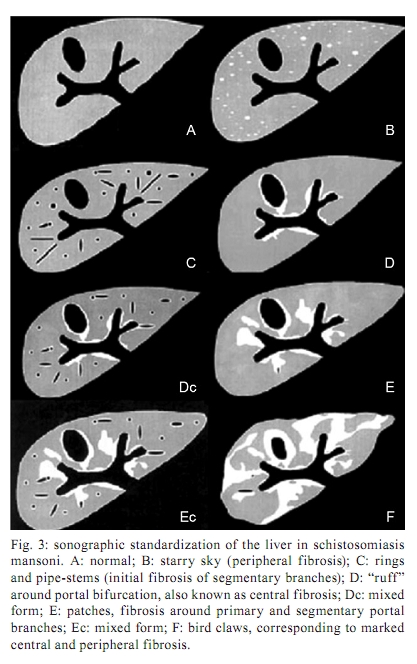
de Radiologia, Hospital das Clínicas + Corresponding author: rapsilva@gmail.com Received 19 May 2009 ABSTRACT We reviewed ultrasound features in patients with schistosomiasis mansoni. The alterations that we observed in acute and hepatosplenic schistosomiasis are described. The advantages and disadvantages of using ultrasound patterns in the evaluation of liver fibrosis are discussed. Other diseases that are important in the differential diagnosis of schistosomal liver fibrosis are presented. Ultrasound is an effective and flexible diagnostic tool in the evaluation of a variety of diseases. It presents no harmful effects to patients, allowing non-invasive studies in hospitalized patients and in other facilities. Key words: ultrasonography - ultrasound - schistosomiasis - diagnostic imaging - hepatosplenic schistosomiasis Abdel Wahab et al. (1979) were the first to report the ultrasound features of hepatosplenic schistosomiasis mansoni. Their findings were confirmed by several investigators in Africa (Fataar et al. 1984, Hussain et al. 1984) and in Brazil (Cerri et al. 1984, Domingues et al. 1993, Pinto-Silva et al. 1994, Lambertucci et al. 2001, 2008). Table I summarises the main findings reported by the above investigators. The first studies were carried out in hospitalized patients with severe hepatosplenic schistosomiasis; in most cases, there was also a history of upper digestive bleeding. In this scenario, ultrasound proved to be efficient in the diagnosis of liver fibrosis and in the differential diagnosis with other chronic liver diseases such as cirrhosis, steatosis and liver abscesses. In addition, ultrasound facilitated the exclusion of other diseases that evolved with splenomegaly, such as kalazar, lymphoma and portal vein thrombosis (Homeida et al. 1988). Liver fibrosis findings in ultrasound are similar to those described by pathologists in the autopsy theatre (Bogliolo 1957, Andrade & Bina 1983, Lambertucci et al. 2000). The schistosomal periportal fibrosis appears like an echogenic band surrounding the portal vessels from the hilum to the periphery of the liver; in advanced cases, the liver surface may develop pseudonodules as a result of fibrous tissue scaring and retraction. The gallbladder wall is thickened by echogenic tissue as shown in Fig. 1. Liver parenchymal echogenicity is usually preserved. The portal vein and its tributaries are generally dilated. Collateral veins with hepatofugal flow are frequently reported, especially in the following veins: left gastric, short gastric, splenorenal and parumbilical. In the parumbilical vein, the blood flows toward the umbilical scar, where it joins the superficial epigastric veins and may originate the "caput medusae". With the intense use of ultrasound in everyday life, the authors noticed that other diseases shared some characteristics of the schistosomal hepatopathy. For example, other diseases presented some degree of periportal thickening in the hilum, like chronic portal thrombosis (cavernomatous transformation of the portal vein). Another difficulty comes from the coexistence of chronic hepatic viral infection or liver cirrhosis, which turn out to be difficult to differentiate from the hepatosplenic form of schistosomiasis. Table II lists the differential diagnoses of Symmers fibrosis and depicts some clues for differentiating them. Documented ultrasonographic regression of liver fibrosis was reported by Homeida et al. (1991) in 28 patients three years after treatment with praziquantel. Cota et al. (2006) studied 84 patients from a rural endemic area of Brazil four years after treatment with oxamniquine and confirmed the regression of fibrosis in 32% of the patients and the disappearance of splenomegaly in 48% of the patients. Ultrasound showed moderate inter-observer reproducibility (kappa = 0.46) for patterns C through F of the Niamey-Belo Horizonte Protocol and a perfect intra-observer reproducibility (1.00) for static images. In addition, an agreement of 0.43-0.57 was observed for the dynamic study of the same patient in different moments; this was considered satisfactory compared to mammography readings using the Breast Imaging Reporting and Data System criteria of the American College of Radiology. For mammography, the agreement ranges from 0.25-0.75 (Santos et al. 2007). Ultrasound and doppler imaging in schistosomal portal hypertension - Portal hypertension can be suspected by B-mode sonography when dilation of one or more of the portal, mesenteric and splenic veins is observed (typical diameters for adults are: portal vein, < 12 mm; superior mesenteric and splenic veins, < 9 mm) and when the collateral veins are present. The most commonly described collateral veins are the left and right gastric, the short gastric, the parumbilical and the splenorenal. Other vessels are less frequently observed, especially splenointercostal veins and direct shunting between portal branches and hepatic veins (Pinto-Silva et al. 1994). Colour Doppler increases the sensitivity of ultrasound because it detects the presence and direction of blood flow and the presence of hepatofugal circulation. Moreover, it is possible to measure flow velocity and to estimate the flow volume-per-minute, which indirectly assesses any physiopathological changes in portal circulation. Vezozzo et al. (2006) did not find significant differences in the Doppler findings between patients with hepatosplenic and hepatointestinal schistosomiasis. A dilated parumbilical vein can increase portal flow velocity and volume-per-minute (Widman et al. 2001). The absence of blood flow indicates acute thrombosis or a very slow flow (Vezozzo et al. 2006). Portal thrombosis is more frequently observed after portal hypertension surgery (de Cleva et al. 2005). The hepatic veins in schistosomiasis remain patent with normal phasic flow as the disease evolves, which is different from liver cirrhosis. In advanced cirrhosis, hepatic venous outflow becomes monophasic. The right hepatic vein is closer to the diaphragm as a result of atrophy of the posterolateral segment of the right liver lobe. There is no consensus about the presence of alterations in the hepatic artery flow in hepatosplenic schistosomiasis. Most authors have found no variations (Bogliolo 1957, Coutinho 1964), whereas some observed a compensatory increase in arterial blood flow (Andrade & Cheever 1971). The splenic artery is dilated with increased blood flow in patients with massive splenomegaly. Ultrasound in acute schistosomiasis mansoni - Lambertucci et al. (1994) and Rabello et al. (1994) described the sonographic features of acute schistosomiasis in both adults and children. The findings included hepatic and splenic enlargement without focal parenchymal lesions and increased periportal and mesenteric lymph nodes. The echogenic hilum of lymph nodes was enlarged and was surrounded by a thin symmetric hypoechoic cortex. This finding is not specific for acute schistosomiasis, being observed in other hepatobiliary inflammatory diseases. The sonographic features of acute schistosomiasis are shown in Fig. 2. Acute schistosomal granulomas are not usually detected by ultrasound. Other imaging methods such as computed tomography (Cesmeli et al. 1997) and magnetic resonance imaging (MRI) may show them after contrast injection as non-enhancing nodules. Ultrasound Doppler shows hepatic artery hyperaemia, probably because of acute inflammatory changes (Barata et al. 1999). Field studies - mass treatment response evaluation - World Health Organization (WHO) protocol - Many field-based studies have been performed in African and South American countries to establish ultrasound characteristics and reproducibility (Lambertucci et al. 1987). Homeida et al. (1988) conducted the first study in Sudan, with periportal fibrosis being reported in 19.8% of the 297 patients examined. Comparing three different populations, the investigators found that the prevalence of fibrosis was higher among those not treated for schistosomiasis. Periportal thickening suggestive of fibrosis was found more frequently than hepatosplenomegaly by clinical examination. Doehring-Schwerdtfeger et al. (1989) evaluated 536 Sudanese children with Schistosoma mansoni infection and reported predominant central periportal fibrosis on ultrasound. On the other hand, Homeida et al. (1988) described periportal thickening that started in the peripheral branches and progressed towards the hilum as the disease evolved. Our findings (Gerspacher-Lara et al. 1997) are similar to those of Homeida et al. 1988: patients with isolated central fibrosis did not present evidence of portal hypertension (splenomegaly and collateral vessels). Other authors have emphasized the finding of periportal thickening in patients without eggs in stool, as well as the lower sensitivity of clinical examination in the evaluation of hepatomegaly and splenomegaly. Martins et al. (1998) reported that only 25% of patients with palpable spleens had periportal fibrosis. Marinho et al. (2006) observed that 23% of palpable spleens and 54% of palpable right liver lobes are shown by ultrasound to be of normal size. The liver consistency also had a weak correlation with periportal fibrosis. Portal hypertension may be seen without splenomegaly in cases with abundant hepatofugal collateral circulation or multiple splenic infarcts (haemolytic states). However, splenomegaly without periportal fibrosis may be seen in many clinical conditions, with or without liver disease. A series of controversies in the use of ultrasound forced the WHO to convene a group of experts to create an ultrasound protocol (Hatz et al. 1992). The WHO sponsored the Cairo meeting (Cairo Working Group 1992) to conduct the first attempt of ultrasound standardization in schistosomiasis related morbidity. The conclusions of the Cairo Working Group were revised in the Second International Workshop in Niamey-Nigeria in 1996 (WHO 2000) and in the Satellite Symposium on Ultrasonography in Schistosomiasis in Belo Horizonte, Brazil in 1997 (Richter et al. 2001). As a result of the meetings, standard schematic plates (patterns) were developed, as shown in Fig. 3. The WHO patterns facilitated teaching for field-based ultrasound examinations; however, the inter-observer agreement remained low (King et al. 2003). In our opinion, previous ultrasound experience is important to increase consistency. WHO patterns B, C, D and Dc, which represent patients with light liver fibrosis, are difficult to differentiate from normal liver and from other diseases (Ruiz-Guevara et al. 2007). In some cases, there is a tendency to overestimate the presence of schistosomal liver fibrosis. Correlation with other imaging modalities - Lambertucci et al. (2004) and Silva et al. (2006) reported disagreements between ultrasound and MRI features in the evaluation of schistosomal liver involvement. Silva et al. (2006) found a moderate agreement between ultrasound and MRI in 60 patients with schistosomiasis mansoni. MRI was superior to ultrasound in the assessment of liver and spleen sizes, vascular dilation, collateral vessels and periportal thickening. The apparent gallbladder wall thickening described on ultrasound actually corresponds to adipose tissue infiltration. MRI presented high inter-observer agreement. The field-of-view of the images includes the whole abdomen and the images can be saved for further review and analysis. Another study reported a poor agreement between ultrasound and MRI; the analysis of MRI showed perfect inter-observer agreement in 14 patients (Scortegagna et al. 2007). Ultrasound is an effective and flexible diagnostic tool in the evaluation of a variety of diseases. It presents no harmful effects to patients, allowing non-invasive studies in hospitalized patients and in other facilities. Despite its limitations, which include its high dependence on operator skills, ultrasound may be used to measure intra-abdominal organs and vessels as well as to diagnose moderate to severe schistosomiasis and other liver diseases. Physical examination is more subjective and is especially difficult in obese and non-cooperative patients such as children. Data may be stored using the Digital Imaging and Communications in Medicine protocol and sent to other examiners via the internet. Portability and connectivity have also improved in new ultrasound devices. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10082f1.jpg] [oc10082f3.jpg] [oc10082t2.jpg] [oc10082t1.jpg] [oc10082f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}