 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 4, 2010, pp. 578-586 The role of population movement in the epidemiology and control of schistosomiasis in Brazil: a preliminary typology of population movement Helmut KloosI; Rodrigo Correa-OliveiraII, IV; Dener Carlos dos ReisIII, IV; Ed Wilson RodriguesIII; Luciana Alves Silveira MonteiroIII; Andrea GazzinelliIII, IV, + IDepartment
of Epidemiology and Biostatistics, University of California Medical Center,
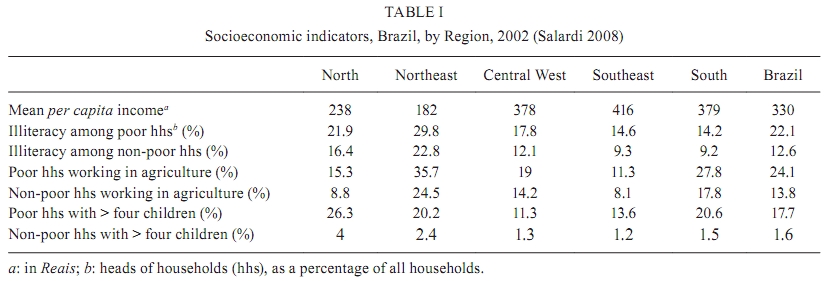
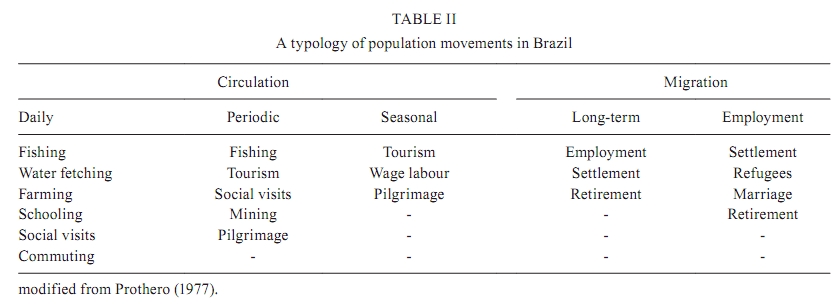
San Francisco, California, USA + Corresponding author: andreag@enf.ufmg.br Received 4 May 2009 Financial support: UNICEF/UNDP/World Bank/WHO/TDR, FIC (1D43TW006580), FAPEMIG, CNPq Code Number: oc10099ABSTRACT This paper examines recent developments in migration studies. It reviews literature related to the potential role of internal population movement in the occurrence of schistosomiasis in Brazil and modifies Prothero's typology of population movement for use in Brazil. This modified classification system may contribute to a better understanding of schistosome transmission as well as improved research and control programs. The results of this study indicate that population movement in Brazil primarily involves economically-motivated rural-urban and interregional movement. However, several movement patterns have become increasingly important in recent years as a result of changing socioeconomic and urbanisation dynamics. These patterns include urban-urban, intracity and urban-rural movement as well as the movement of environmental refugees and tourists. Little is known about the epidemiological significance of these patterns. This paper also highlights the role of social networks in the decision to migrate and to settle. Prothero's classic population movement typology categorises movement as either one-way migrations or circulations and examines them along spatial and temporal scales. However, the typology must be modified as epidemiological information about new patterns becomes available. This paper identifies areas that require further research and offers recommendations that can improve the measurement and spatial analysis of the relationship between population movement and schistosomiasis. Key words: schistosomiasis - typology of population movements - spatial analysis - schistosomiasis control - Brazil Population movement often increases exposure to infectious disease and can affect disease prevention and control efforts (Galvani & May 2005). Many epidemiological studies have shown that human migration affects the transmission, spread and control of schistosomiasis in Brazil (Ximenes et al. 2000) and around the world (Chitsulo et al. 2000, Bruun & Aagaard-Hansen 2008). However, the determinants, patterns and impacts of this migration are poorly understood. Suitable methodologies and reliable data are limited and, as a result, there have been few rigorous examinations of the epidemiological role of human movement in schistosomiasis and other parasitic diseases (Stoddard et al. 2009). Junghanss (1998) examined the relationship between tuberculosis and population movement, but found that the absence of information about underlying circumstances and mechanisms made such a project difficult. This problem is common in epidemiological studies of migration, including studies of migration and schistosomiasis; it is usually referred to as "black box epidemiology" (Junghanss 1998). The lack of reliable information on peoples' movements is often caused by limited detailed public records on migration; in addition, migrants may be unable to reliably recall their exposure at multiple heterogeneous water contact sites that may range from non-infective to highly infective (Kloos et al. 2006). Many migrants are also concerned about privacy and are therefore reluctant to fully disclose exposure history; this adds to the difficulty of establishing population movement histories and exposure risk (Junghanss 1998). Population movements in the global South are considerably more complicated than those in the industrialised North because of complex social, economic, demographic and political factors. Ravenstein's influential theory of migration, therefore, may be inadequate in nations where schistosomiasis is endemic. Ravenstein's theory has been modified by Lee (1966) and is based on Newton's Law of Gravitation. According to the gravity model of migration, geographical movements result from decisions made by economically rational individuals who weigh the push and pull factors at two locations (the origin and the destination) and evaluate the obstacles, particularly distance, between those two locations. This model describes only one type of movement (from the place of origin to the final destination) and assumes that individuals have complete freedom in their migratory decisions; it therefore neglects the role of social processes in population movement. The gravity model and the related human capital model have been employed in regional migration studies in Brazil (Golgher et al. 2005, Justo & Silveira Neto 2006). It is increasingly recognised, however, that social processes, including social capital or networks, also play a large role in the decision to migrate and in the timing, spatiality and success of movements such as circulation, chain migration and seasonal movements (Aragon 1985, Watts 2008). Epidemiological studies of the relationship between population movement and schistosomiasis have been conducted for at least four decades (Bradley 1968, Ruyssenaars et al. 1973, Kloos et al. 1980, Machado 1982, Ximenes et al. 2000). However, many aspects of this relationship remain poorly understood. The only detailed study of migration and schistosomiasis in Brazil focused on rural-urban migration that was largely the result of socioeconomic forces (Ximenes et al. 2000). Most studies focus on rural-urban and rural-rural migrations and examine only the migrants' place of origin and duration of stay. Researchers and public health officials in Brazil are increasingly focused on understanding other patterns, including additional motivations for migration (such as travel for social, educational, medical and recreational reasons), changing urbanisation patterns (Carmo & Barreto 1994, Enk et al. 2004), urban-urban migration and return migration (Ribeiro & Carvalho 1999, Ximenes et al. 2000, Golgher et al. 2005). Migrants contribute to the transmission and spread of schistosomiasis in at least three ways: (i) by introducing the parasite into non-endemic areas, (ii) by creating habitats for snail intermediate hosts and water contact points in the areas where they settle and (iii) by direct moves in which infected people migrate to areas where schistosomiasis has been controlled or eradicated (WHO 2000). A lack of detailed and reliable information impedes our understanding of migration and schistosomiasis at different spatial and temporal scales in Brazil; this literature review may identify important relationships and areas that require further research. The Brazilian national schistosomiasis control program has had a significant effect. The prevalence of Schistosoma mansoni infections nation-wide was reduced by 38.5% between 2000-2003 by treating carriers. In addition, the prevalence of infection was reduced by more than 50% in hyperendemic municipalities in the state of Paraíba after the first year of treatment (Amaral et al. 2006). Nation-wide, the number of hospitalised cases fell by 65% between 1988-1999; schistosomiasis-specific mortality fell by 54% between 1979-1997 (WHO 2000) and mean schistosomiasis prevalence rates declined from 11.5% in 1980-1989 to 9.2% in 1990-2002 (Coura & Amaral 2004). Over the same period, however, prevalence rates increased in five states [Alagoas (AL), Sergipe, Rio Grande do Norte (RN), Ceará and Santa Catarina (SC)] and in the Federal District (FD); the rates did not change in Paraná (PR) (Coura & Amaral 2004). Reductions in prevalence and the intensity of infection also varied in different localities. Control has been particularly difficult in places that depend on farming, fishing and other activities that increase occupational exposure (Kloetzel 1989, WHO 2000). Groups with low socioeconomic status generally have a higher risk of contracting schistosomiasis and of being affected by the disease for an extended period of time. This risk is related to a variety of factors that include a lack of access to safe water and to health services (Ximenes et al. 2003, Kloos et al. 2008, Watts 2008). Population movements affect all areas and communities that are vulnerable to schistosomiasis in Brazil. Attention has recently been directed toward both rural and urban areas despite the schistosomiasis control program's treatment of infected migrants in some areas of Brazil (Coura & Amaral 2004). The objectives of this paper are to examine population movement patterns and determinants as well as the impact of these movements on the occurrence and spread of schistosomiasis in Brazil. The paper presents a preliminary typology based on the typology developed by Prothero (1977) to identify some understudied areas and to provide guidelines for further research. Prothero's typology considers causal, spatial and temporal dimensions of individual and group movement and has been employed in the study of various vector-borne diseases in different endemic regions (Stoddard et al. 2009). MATERIALS AND METHODS Source material for this study was obtained from online literature searches and from the literature collection of the first author (which includes four decades of literature). Several online search terms were used: "migration, schistosomiasis, Brazil", "population movements, schistosomiasis", "schistosomiasis, migrants, Brazil", "tourism, travel, schistosomiasis, Brazil", "schistosomiasis, parasite spread, Brazil" and "schistosomiasis, snail spread, Brazil". These searches identified 62 articles in the PubMed database on the relationship between population movement and schistosomiasis. The search terms "migration, Brazil", "population movements, Brazil" and "population movement typology, Brazil" were also entered into the Google search function. These searches identified 239 papers on population movement and other disease and health issues and 1,597 publications on population movement and migration; most of these results were socioeconomic and demographic studies. Most of the studies returned by the Google search did not meet the spatial, temporal and motivational criteria set for this study. Additional manual searches of individual articles were carried out because epidemiological studies of schistosomiasis that include population movement as an explanatory variable normally do not include keywords such as "migration" or "population movements"; this is especially true if no statistically significant relationship with infection was found. Survey and national population data was obtained, in part, from the 2000 National Census and the 2002-2003 household survey (Pesquisa Nacional por Amostra de Domicílios and Pesquisa de Orçamentos Familiares), Golgher et al. 2005, World Bank 2007, Salardi 2008]. In addition, data from community-based studies were used to describe spatial and temporal variations in population movement and socioeconomic determinants at the regional and local levels. Prothero's (1977) typology of population movement was developed for the study of malaria epidemiology in Africa; we modified this typology to examine the role of population movement in the spread of schistosomiasis in Brazil. The individual types of population movement that are included are based on a review of Brazilian demographic literature and any available epidemiological studies of schistosomiasis. Population movements Interregional movements - Southern Brazil has the highest rate of economic development in the nation and this development has been largely attributed to the southward migration of farm labourers from the sugar cane plantations in the Northeast (Machado 1982). In 2002, the Southeastern Region produced 56% of real Brazilian gross domestic product (GDP); the two most economically depressed regions, the Northeast and North, together produced only 16% of Brazilian GDP (IBGE 2002). According to the 2002 household survey conducted by the Instituto Brasileiro de Geografia e Estatística, the highest levels of poverty in terms of per capita income exist in the nine Northeastern states. The second-highest levels of poverty are in the 10 Northern and Central-Western states. The lowest poverty rates exist in the four Southeastern and three Southern states. Similarly, illiteracy rates among poor household heads were 14.6% in the Southeast and 14.2% in the South but 29.8% in the Northeast. Even higher differentials between the Northeast and Southeast Regions existed in the percentage of poor households working in agriculture. In the Southeast, 11% of poor and 8% of non-poor household heads worked in agriculture; in the Northeast, however, 35.7% of the poor and 24.5% of the non-poor household heads worked in agriculture. Larger family sizes and larger proportions of Afro-Brazilians in the Northeast and North further skew the socioeconomic profile in favour of the wealthier regions (Table I). Push factors (poverty, unemployment and a lack of social services in areas of outmigration) and pull factors (economic opportunities at destinations) are major determinants of interregional population movement, including both rural-urban and rural-rural movement (Golgher et al. 2005, Salardi 2008). An additional factor leading to poverty and outmigration in the Northeast is environmental degradation, which is expected to worsen in the future as the climate changes (Sietz et al. 2006). Epidemiologists have paid little attention to the issue of where migrants from various places of origin ultimately settle. Data from the 2000 Brazilian Census show that migrants from Minas Gerais (MG), Bahia (BA), Piauí and other states tend to cluster in different neighbourhoods in the São Paulo (SP) metropolitan area as a result of social networks (Skop et al. 2006). In view of the heterogeneity of schistosomiasis distribution among and within states (Coura & Amaral 2004) and the variety of snail intermediate hosts in urban areas (Barreto 1991), such migrant clusters may play an important role the epidemiology of schistosomiasis and control efforts. Movements within regions - Within each region, poverty levels continue to be significantly higher in rural areas than in metropolitan areas; smaller urban areas are generally at intermediate levels. Two common measures of poverty, the extreme poverty index and the minimum livelihood index, identify individuals who cannot afford to meet basic food needs and determine basic food and non-food needs, respectively. These measures were at least five times higher in rural than metropolitan areas and about twice as high in rural than urban areas overall (Salardi 2008). The spatial distribution of the Human Development Index (HDI), which is based on life expectancy, literacy, highest grade of school completed and per capita GDP, was used by Golgher et al. (2005) to classify the 5,507 municipalities included in the 2000 National Census. Differential rates of poverty and economic development, combined with spatial variations in labour surplus or high population density and relatively strong urban-based labour demands, are the major push and pull factors in both regional and rural-urban migration (Justo & Silveira Neto 2006). These factors have contributed to the high urbanisation rate and the decrease in the rural population over the last five decades (Camarano & Abramovay 1999). The modernisation and commercialisation of agriculture exacerbated the overpopulation and high unemployment problems and thus increased emigration from the Northeast (Goza 1992, Brumer 2008). Heavy rural-urban migration resulted in extremely high urbanisation rates. While 30% of the Brazilian population lived in urban areas in 1940, 55% lived in these areas in 1970 and 81.2% lived in these areas in 2000 (PAHO 2002). Although the unique rural/urban classification system used by Brazil's census bureau has caused some debate over the figure for 2000 (Veiga 2004), it is important for this study that urban/rural differences in schistosomiasis occurrence have tended to decrease. The establishment of rural agrarian reform settlements between 1985-1997 resulted in the movement of 30,226 families into government-assisted farm projects throughout the country. Although many settlers moved within the same municipalities, considerable numbers of individuals in SC moved there from other parts of the state; in the FD and in Pará, a large percentage of settlers were born in other states (Heredia et al. 2005). Brazilian Indians (Ribeiro & Curtis 1993) and Catholics have also made pilgrimages for hundreds of years. Although catholic pilgrimages to cities, towns and villages occur daily and can involve millions of people (Kiddy 2005), no specific information is available on their possible relationship to schistosomiasis risk. Recently emerging types of migration - Recently, a greater variety of internal migrations have become common in Brazil and other South American countries; these new migration patterns have resulted from greater population mobility and socioeconomic developments like rising urban unemployment and the rapid growth of slums that lack adequate infrastructure and social services (Tannen 1992, Matos 1995, PAHO 2002). As a result of these developments, new migration dynamics gradually emerged in the 1990s; these dynamics are characterised by a decrease in migration to the main urban centres, an increase in migration to medium-sized towns, greater population retention in some areas of traditional outmigration and heavier rates of return migration (Golgher et al. 2005). Additional changes include increases in urban-rural, urban-urban, seasonal and short-term movements for economic, educational, social, recreational and retirement purposes (PAHO 2002, Cerrutti & Bartoncello 2003, Enk et al. 2004). Regional and municipality maps at the national level show some of these changes through census data. Although six of the seven regions with high outmigration between 1995-2000 (each with net losses of 50,000-500,000 people) were in the Northeast, RN had a net migration gain between 1995-2000. In addition, two regions in the South (PR and Rio Grande do Sul) and one state each in the Central-West (Goiás) and North (Acre) had net outflows. Similarly, although rural municipalities in all regions experienced population declines during that five-year period, large areas of new land settlement were developed in the North and Central-West regions; in addition, some municipalities surrounding large metropolises, especially in the South and Southeast, gained population through migration (Golgher et al. 2005). Spatial distribution of schistosomiasis Coura and Amaral (2004) mapped and summarised the spatial distribution of schistosomiasis in Brazil. Regional studies have examined several municipalities, in BA (Carmo & Barreto 1994), Pernambuco (de Farias et al. 2007, Favre et al. 2008), MG (Guimarães & Tavares Neto 2008, Martins et al. 2008), Rio de Janeiro (RJ) (Moza et al. 2005) and AL (Moza et al. 2005, de Farias et al. 2007). In addition to showing the clustering of schistosomiasis in the well-known hyperendemic areas in the rainforests in the Northeast and in northern MG, these studies also reveal considerable heterogeneity among municipalities. An increasing number of spatial epidemiological studies of schistosomiasis have been conducted at the community level (Gazzinelli & Kloos 2007) and were presented at the 11th International Symposium of Schistosomiasis in Salvador, BA. These studies also show a considerable degree of heterogeneity which is discussed in more detail below. Little information is available on the impact of migrants on spatial clustering and the maintenance of schistosomiasis. A typology of population movements People moving to and from (or through) schistosomiasis-endemic areas may be categorised as either active transmitters or passive acquirers of infection. Passive acquirers may have low levels of immunity or no immunity and are at particularly high risk of developing the disease when moving from non-endemic to endemic areas. The typology presented here draws on the above-mentioned definitions and considers temporal scales to identify the five major categories of population movement in Brazil. In Table II, various activities are grouped under these categories and, when assessed within the context of local environmental and epidemiological parameters, can be associated with different risks of S. mansoni transmission and spread. This typology can accommodate all types of population movement from the community to the national levels. It is important to remember, however, that some movements can be placed in more than one category because they may be multi-purpose and may overlap geographically and temporally. Migration - Prothero's (1977) broadly-based definition of population movement includes "migration" (the permanent change of residence) and "circulation" (daily, periodic, seasonal and long-term movements); circulation has been described by some investigators as "circular migration". Migration from rural to urban areas was found to be highly predictive of schistosomiasis infection (Carmo & Barreto 1994, Carvalho et al. 1997, Lima e Costa et al. 1998). The well-known influx of large numbers of rural migrants from the Northeast to the industrial Southeast, together with the congregation of large numbers of people living under precarious conditions as a result of the urbanisation process, has made schistosomiasis a public health problem in the municipality of São Paulo, Campinas and other cities (da Silva 1985, de Lima 1995). In the metropolitan area of Belo Horizonte, MG, where most migrants come from the hyperendemic northern part of MG (Matos 1995), schistosomiasis prevalence has been between 7-10%. This prevalence is similar to the overall rate in MG over most of the last seven decades (Schall & Diniz 2001). Although most studies report higher infection rates in migrants than in native urban residents, several studies found that the risk of infection increased with the length of stay in urban areas (Ximenes et al. 2000, Massara et al. 2004). Ximenes distinguished between migrants from endemic and non-endemic areas and found that infection rates among the former were similar to those of native urban dwellers while infection rates among the latter were significantly higher. Long distance rural-rural migrations, such as movement from the Northeast to the Amazon Basin, pose similar public health threats as rural-urban migrations. Settlement by farmers, gold miners, extractors of forest products and labourers at dam construction projects in the Amazon Basin warrant particular attention in light of the rapid development of that area. The presence of two snail intermediate hosts of S. mansoni (Biomphalaria straminae and Biomphalaria amazonica) and of infected migrants from areas in the Northeast makes it likely that schistosomiasis will become endemic as the Amazon Basin develops and the population increases (Corrêa & Paraense 1971, Coimbra Júnior et al. 1984, Barrow 1987, Bichara et al. 1997, Paraense 2001, Fernandez & Thiengo 2002). Many of the settlers from the Northeast are environmental refugees, a newly defined category of migrants who leave their home areas due to climate change and environmental deterioration (Kayley 2008, Barbieri et al. 2009). The spread of schistosomiasis and several species of Biomphalaria as a result of changes in the natural environment caused by settlement and agricultural development has also been described in the South and Southeast (Paraense 2001). Migrations often take place in stages and include one or more stopovers along the way (Goza 1994, Ribeiro et al. 2004). Most existing maps of regional migration, however, show non-stop flows of migrants rather than multistage migration (Coura & Amaral 2004). Although multistage migrations are not often studied by epidemiologists, they may result in additional exposure risk and influence the reliability of migrant exposure histories. Unsuccessful settlers in agricultural settlement areas in the Amazon basin and migrants in the industrial Southeast often return to their home areas or move on to other destinations (Tannen 1992, Goza 1994, Ribeiro et al. 2004). Circulation - Most epidemiologically-relevant movements of people do not involve a permanent change of residence but represent different types of circulation that result in the return of migrants to their home areas. This was true in Africa (Prothero 1977) and is also apparent in Brazil. Circulation involves movements that last from one day to more than a year; they are classified here according to time scale. Daily circulation involves leaving a place of residence for a period up to 24 h. A number of epidemiological studies of schistosomiasis in Brazil and Africa have reported daily circulation movements by housewives, farmers, people visiting relatives and students attending school, among others (Ruyssenaars et al. 1973, Lima e Costa et al. 1987, 1998, Gazzinelli & Kloos 2007, Kloos et al. 2008). Perhaps the most common daily movements in rural areas are trips to household water sites at streams and other potential transmission sites; the patterns and epidemiological risks of these movements have been identified and spatially analysed in a number of studies (Kloos et al. 1998, Friedman et al. 2001, Gazzinelli et al. 2001). Daily movements of farmers to the fields may be similarly important epidemiologically because many farmers wash or bathe in streams near their homes on their return trips (Kloos et al. 2006). The risk associated with daily commuting to work in urban areas is probably low because of the use of motorised transport; this topic, however, has not been studied. Periodic circulation may extend from one day to one year. In seasonal circulation (a type of periodic circulation), the timing of movements is defined by distinct seasonality in the economic cycle or the physical environment; persons or groups are absent from their permanent homes for one or more seasons of the year (Goza 1992). Tourism, which typically involves the periodic and seasonal movement of urban residents to larger tourist centres and smaller rural resorts, is increasingly associated with schistosomiasis infection. These movements are mostly by persons in the higher socioeconomic brackets who tend to have little acquired immunity to schistosomiasis. Common exposure risk activities include recreational fishing, bathing and swimming (Barbosa et al. 2004, Enk et al. 2004). Carvalho et al. (2008) studied tourism as a risk factor in RJ, SP and MG; they examined 178 towns included in the Estrada Real Tourism Project. Seasonal wage labour by rural people in towns may also carry considerable risk of introducing S. mansoni into ecologically vulnerable urban neighbourhoods. Long-term circulation, defined as absence from home for more than one year, often occurs among returning settlers in new agricultural settlement areas in the Amazon Basin (Goza 1994). Return movements of retired persons to their places of birth may also entail increased exposure. The pattern and schistosomiasis risk of long-term circulations are relatively difficult to determine retrospectively. Recall loss is a particular problem, especially if the circulation included multistage movements and therefore exposure activities at potential transmission sites in different communities. Long-term circulations or migration within municipalities or between nearby communities often result in short-distance movement; however, they may also result in significant changes in exposure to schistosomiasis. In a rural area in northern of MG (Melquiades), an estimated 10% of the households moved within a four-year period to houses in the same or other hamlets that had significantly different S. mansoni prevalence levels (Gazzinelli et al. 2006). Significant spatial heterogeneity of schistosomiasis prevalence was reported from other small rural areas (Brooker et al. 2006) and in urban communities. From a control perspective, daily activities tend to reduce the effectiveness of interventions. For example, in one municipality in MG (Sabará), a 2.5% S. mansoni infection rate persists after 27 years of domestic water treatment for the entire population and chemotherapy for infected individuals. The continued infection rate has been partly attributed to the daily movements of farmers to the fields and the frequent contact people have with rivers and streams (Vasconcelos et al. 2009). Short-distance movements appear to be similarly important in urban areas. Two recently-described types of urban migration, urban-urban movements between towns and intracity movements from the inner city to the suburbs of the same urban area, may be conducive to schistosomiasis transmission and spread. Urban-urban migration, which has become more common due to the diversification of the Brazilian economy and rapid urbanisation, accounted for 61% of all intermunicipal movement between 1981-1991 (Cerrutti & Bartoncello 2003). Significant differences in S. mansoni infection rates were reported from various neighbourhoods in towns in BA and AL (Kloetzel 1989, Barreto 1991). In addition, the presence of S. mansoni infections among poor settlers at the urban fringe of RJ (Grault et al. 1998) suggests that the epidemiological consequences of moves within urban areas may be considerable. The movement of inner-city populations to the sprawling suburbs has accelerated since the 1980s in response to increasing congestion, crime and pollution (Matos 1995, Cerrutti & Bartoncello 2003). In many favelas, rapid urban growth overtakes infrastructure development and is characterised by a lack of safe water supplies and sewage systems; such growth is also associated with an increased risk of schistosomiasis exposure (Soares et al. 1995, Schall & Diniz 2001, Massara et al. 2004, Guimarães et al. 2008). The tendency of Biomphalaria tenagophila and possibly other snail species to cluster in urban neighbourhoods that have high levels of organic pollution in surface water (Teles 2005) increases the risk of transmission in these neighbourhoods. In addition to the spatial and temporal patterns of population movements, the presence of migrants, returnees and visitors in endemic areas can significantly influence surveillance and treatment outcomes. The movement of infected migrants in and out of project areas may affect control activities (Pieri et al. 1998) and failure to exclude migrants and other persons moving out of study areas may affect schistosomiasis risk assessment (Disch et al. 2002). As a result of the efficient passive case detection program in Brazil, migrants have assumed a relatively more significant role. For example, migrants represented 89% of all infected persons in SP in 1992 (Glasser 1995). In a rural community in MG, the only S. mansoni-infected Biomphalaria glabrata snails found four months after the administration of mass chemotherapy were located at a stream site used exclusively by infected vacationing visitors for bathing (Kloos et al. 2001). Selected methodological guidelines for the study of population movement and schistosomiasis Studies of population movement in schistosomiasis epidemiology and control in Brazil can benefit from more reliable survey data, appropriate data acquisition tools and improved analytic methods. Spatial scale - The spatial scale of a study, which may range from the local to the interregional and international levels, will determine the framework of the data gathering and analytical processes. While detailed information on local movements and exposure risk may be obtained at the individual level, larger geographical units and secondary survey or census data may be the only affordable or available options for obtaining data at the regional and interregional levels. The research question, particularly whether local transmission or the spread of schistosomiasis is the focus of the study and available resources will also determine the spatial scale of a study. Measurement - The measurement of population movements and their epidemiological significance continues to be a major problem in studies of schistosomiasis. Questionnaires have traditionally been used at the community level to elicit, at relatively low cost, information on spatial, temporal and motivational aspects of the migration process and schistosomiasis exposure. Although these questionnaires can capture both quantitative and qualitative information, they are subject to recall error and social desirability bias and fail to identify transmission sites at the local level (Friedman et al. 2001). The efficiency of questionnaires identifying exposure risk may be increased by preparing questionnaires for each study community (Lima e Costa et al. 1998). Kloos et al. (2006) used a combined methodology involving questionnaires and direct observation of water contact behaviour to overcome these limitations in a village in the northern part of MG, but no comparable methods exist for the study of local population movements. Our research group used electronic personal data assistants and global positioning system (GPS) units to facilitate the tracking of individuals and families who changed residences within rural study communities. The placement of smaller GPS units on individuals has been recommended by Stoddard et al. (2009) and Seto et al. (2007) as the best option for tracking daily, short-distance movements in rural communities; cellular phones may be used for large-scale studies or studies of regional movements and movements within large urban areas where GPS signals are intermittent. To the best of our knowledge, these and other electronic devices have not been used in research in Brazil. Their use may not be technically feasible for most endemic areas and would have to be complemented with survey methods to generate information on the determinants (facilitators and impediments) of movements (such as social networks) or on exposure risk. Spatial analysis - The rapid increase in Geographic Information System-based spatial studies of schistosomiasis in Brazil (Gazzinelli & Kloos 2007) was also revealed in the increasing number of papers presented at the 10th and 11th International Symposia on Schistosomiasis in Belo Horizonte, MG, in 2005, and Salvador, BA, in 2008. These studies can clarify the dynamics of spatial and temporal interactions and are important to the schistosomiasis control program. Climate, soil, vegetation and socioeconomic data may be integrated to model S. mansoni transmission risk in different communities and municipalities; these models can guide field work and may increase the allocation of resources in schistosomiasis control and contribute to the formulation of effective health strategies (Bavia et al. 2001, Guimarães et al. 2008, 2009). However, further progress will require the improvement of surveillance and reporting activities in the national, state and municipal schistosomiasis control programs (de Farias et al. 2007, Favre et al. 2008). This study reveals a variety of types of population movement, both permanent and temporary, that result in significant spatial and temporal shifts in the distribution of the population. These shifts affect the transmission, spread and control of schistosomiasis. Socioeconomic differentials at all social levels (from the family to the region) are the dominant and most widely-published determinants of population movement. Recent studies, however, have also shown that social networks and tourism can act as pull factors while growing inner-city problems act as push factors. This study identifies several neglected and emerging types of population movement, including chain migrations, multistage migration and return migration, as well as various forms of circulation. Many of these patterns have occurred in Brazil for a long time, although some, like tourism, urban-urban, intracity and urban-rural movements, are more recent. A major reason for this neglect appears to be the influence of traditional migration theories developed in the global North which are inadequate for studies of the more complex population movements in Brazil. The preliminary typology of population movements developed in this study, based on Prothero's (1977) model, is an effort to address these shortcomings and to provide a benchmark for further spatial epidemiological studies. The typology must be validated and modified further as epidemiological and demographic data on several types of population movement become available. In particular, further expansion of the schistosomiasis data base and interdisciplinary research may permit more detailed studies of causal relationships, the impact of various movements and their relevance for schistosomiasis control at the state, municipal and community levels. Poverty, rural living and incomplete urbanisation have interrelated effects on a number of water-related infectious diseases in Brazil and the development of appropriate methodologies may benefit surveillance, prevention and treatment programs for these other diseases. Overcoming the persistent economic inequities that underlie much of the vulnerability to schistosomiasis infection will also require further progress in broadly-based socioeconomic reform, including land reform, greater wealth equity and the provision of safe water, basic sanitation facilities and effective primary health care in poor communities. ACKNOWLEDGEMENTS To the anonymous reviewers, for valuable suggestions. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10099t1.jpg] [oc10099t2.jpg] |
| |||||||||

{kind=link}
{kind=link}