 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 5, 2010, pp. 621-626 ARTICLES Chagas disease: serological and electrocardiographic studies in Wichi and Creole communities of Misión Nueva Pompeya, Chaco, Argentina Edgardo MorettiI, +; Irma CastroI; Claudio FranceschiII; Beatriz BassoI IFacultad
de Ciencias Médicas, Universidad Nacional de Córdoba and Coordinación
Nacional de Control de Vectores, Tránsito Cáceres de Allende 421,
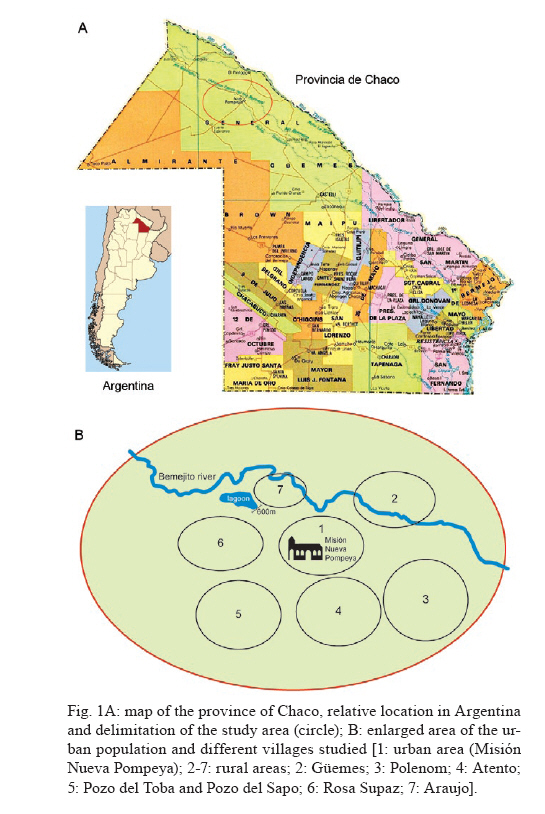
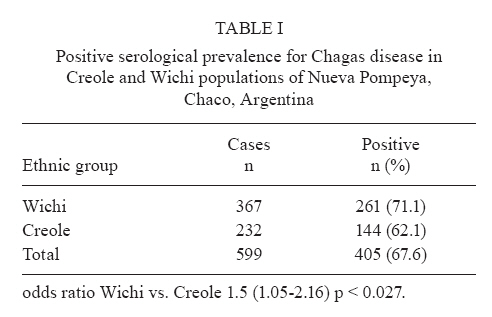
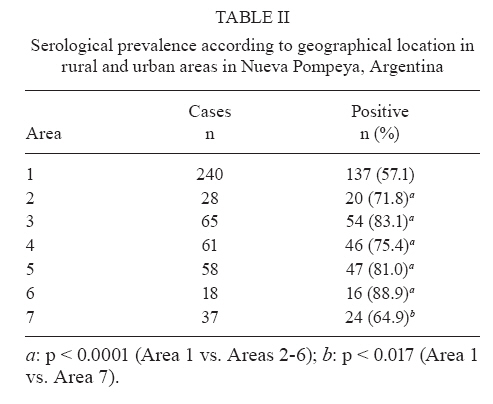
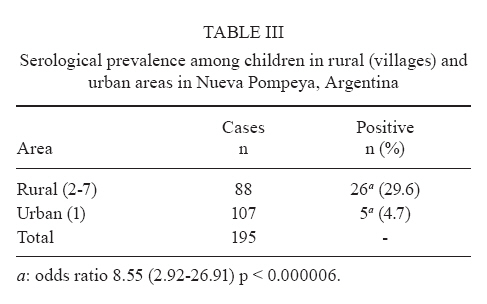
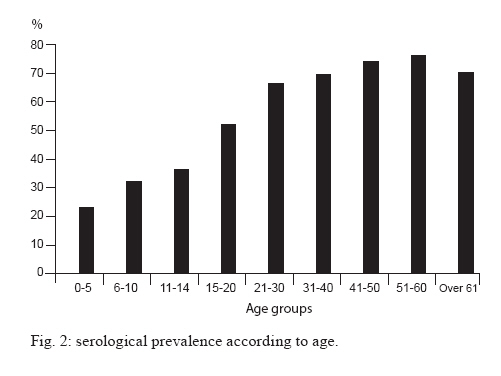
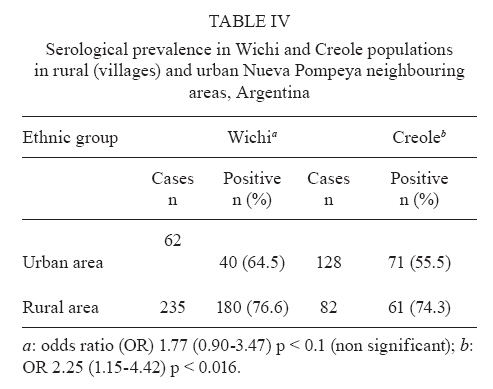
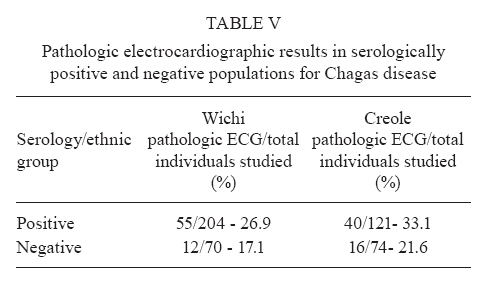
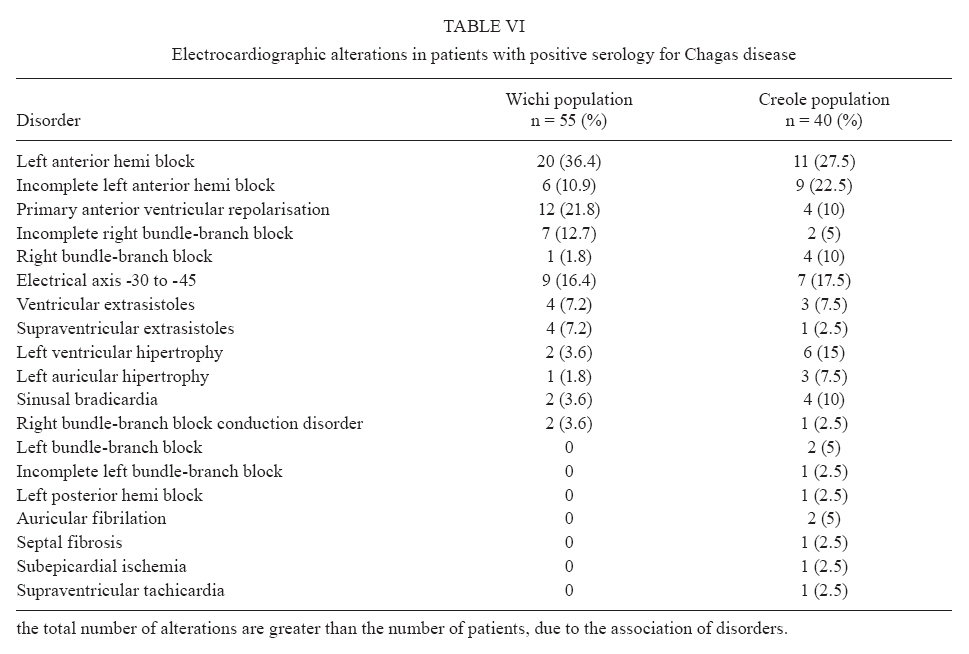
5000 Córdoba, Argentina + Corresponding author: ebi@fcm.unc.edu.ar Received 3 December 2009 Code Number: oc10105 ABSTRACT Chagas disease, which is caused by Trypanosoma cruzi, affects nearly 16 million people in Latin America and causes 75-90 million people to be at risk of infection. The disease is urbanizing and globalizing due to frequent migrations. There are regions of high prevalence of infection, including the north-eastern provinces of Argentina and the entire phytogeographic region known as the Gran Chaco. In the province of Chaco, Argentina, there are places inhabited by native populations such as the Wichi and Toba communities, among others. Many Creole populations resulting from miscegenation with European colonists and immigrants coexist within these communities. It has been widely accepted that in the chronic phase of the disease, between 25-30% of individuals develop some form of cardiac disease, with the right bundle-branch block being the most typical condition described so far. The aim of this work was to study the prevalence of Chagas infection and its electrocardiographic profile in the Wichi and Creole populations of Misión Nueva Pompeya, in the area known as Monte Impenetrable in Chaco, to determine the prevalence and the pattern of heart diseases produced by Chagas disease in this region. Key words: Chagas disease - Wichi - serological studies - electrocardiographic pattern - Chaco Chagas disease is an anthropozoonosis caused by Trypanosoma cruzi that affects nearly 16 million people in Latin America and that causes 75-90 million people to be at risk of infection (Coura 2007). The etiological agent is the protozoan parasite T. cruzi, which is transmitted by vectors such as Triatoma infestans, Pastrongilus megistus and Rhodnius prolixus, among others, and also via the digestive tract and human-to-human transmission: congenital, blood transfusion and organ transplant. Due to migration, the latter forms of transmission made it possible to spread human infection to areas traditionally free of the disease, like the US and some European countries (Kirchhoff 1993, Moretti et al. 2007, Paricio-Talayero et al. 2008). There are areas of high prevalence of infection in some regions of Latin America, including the north-eastern provinces of Argentina, such as Chaco and Formosa, which are inhabited by Creole and American native populations, such as the Wichi and Toba, among others. Due to some still unknown reasons, there are a high number of infected individuals in whom the parasite does not cause any disease. In contrast, many years after the original infection, 25-30% of patients develop a disease primarily affecting the heart or the digestive system (Andrade & Andrade 1979). Chronic Chagas heart disease presents a greatly variable evolution, morbidity and mortality. In this regard, some authors found that the associated risk factors such as hypertension, atherosclerosis, diabetes mellitus, obesity and smoking, among others, influence the severity of Chagas heart disease (Diez et al. 2006). Most studies on the cardiac profile have been conducted in rural, predominantly Creole populations. The aim of this work was to investigate the prevalence of Chagas infection in an area of the province of Chaco, Argentina, known as the Impenetrable and to analyze the electrocardiographic profile of the native Wichi population, comparing it with that of the Creole population in the same region. PATIENTS, MATERIALS AND METHODS Study population - Individuals from the communities of Wichi and Creole, of urban and rural area of Misión Nueva Pompeya, a village in Chaco forest known as El Impenetrable, which is located in the northwest of the province of Chaco, Argentina (Fig. 1A). As it is shown in Fig. 1B, the urban population is located in Zone # 1 and the surrounding rural villages in Zones # 2-7. Samples - They were taken from venous blood in adults and capillary blood in children. In the first case, the serum was separated and stored at -20ºC until use. Capillary blood was stored in buffered glycerine at room temperature (Serokit). Serological methods - Sera were analyzed by ELISA and indirect hemagglutination tests using conventional commercial kits (Wienerlab), following the manufacturer's instructions. The indirect immunofluorescence reaction was performed with antigen prepared in our laboratory as previously described (Basso et al. 1987). Briefly, T. cruzi epimastigotes were harvested in the exponential phase of growth, washed in PBS and fixed with 0.1% glutaraldehyde. Spots were prepared and the reaction was performed using a conventional technique with fluorescein isothiocyanate-conjugated anti-total human immunoglobulins (bioMérieux). In capillary blood, an ELISA test was performed and positive samples were confirmed with venous blood using the three methods described. Electrocardiographics studies - Fukuda electrocardiographs powered by a local power unit or a power generator were used for the recording of electrocardiograms (ECG). Conventional 12-lead ECG was performed (6 frontal plane and 6 horizontal plane sections) with extended D2 derivation for rhythm control. Whenever alterations were found, the record was extended to determine their permanence or transience. Electrocardiographic abnormalities (ECGA) were reported according to criteria established by Lazzari et al. (1998). Routine medical histories and thorough clinical examinations were performed, with special emphasis on the cardiovascular system. Participants were questioned about the history of concurrent conditions known for the individuals and for their family groups. Ethics - The procedures followed were in accordance with the ethical standards of the responsible committees on human experimentation of the University of Bologna and the University Hospital of Maternity and Neonatology, Universidad Nacional de Córdoba, Argentina and with the Helsinki Declaration of 1975, as revised in 1983. Authorisation to carry out the study was also granted by the Ministry of Health of the province of Chaco. People who voluntarily participated in the study were informed of its objectives through translators from their own community. Subsequently, prior to signing the consent form, they were read the informed consent written in Spanish and Wichi languages. RESULTS Table I shows the prevalence of positive serology for Chagas disease in both studied groups. As it can be observed, prevalence in the Wichi population was 71.1%, whereas in the Creole population it was 62.1%, p < 0.027. By analyzing the distribution of seroprevalence according to the habitat of the studied subjects (Table II, Fig. 1B) it was observed that the prevalence in individuals living in the urban area of Misión Nueva Pompeya (Area 1) was 57.1%, whereas in rural areas it ranged between 64.9-88.9%, with an average of 77.5%. The difference was statistically significant when the prevalence in urban areas was compared to each of the surrounding villages and to the total rural population (p < 0.0001 when comparing Zone 1 vs. Zones 2-6 and p < 0.017 vs. Zone 7). Remarkably, in Area 2, the only place almost exclusively inhabited by Creoles, the prevalence was very high, similar to that seen in other places mostly inhabited by Wichi populations. In school children, the difference was dramatic, depending on whether they lived in rural areas, where a 29.6% infection rate was found or in urban areas, where only a 4.7% infection rate was recorded, as shown in Table III (p < 0.000006). The analysis by age group in both populations as a whole (Fig. 2) showed a high rate of infection since early infancy; thus, in children aged 0-5 years, the prevalence rate reached 21% and was higher than 50% at age 20. From age 30, there was a plateau close to or above 70%. When each community was investigated according to their place of residence, it was observed that the seropositive rate in the Wichi community (Table IV) was 64.5% in urban areas and 76.6% in the rural villages. This difference was not statistically significant: odds ratio (OR) 1.77 (0.90-3.47) p < 0.11. On the other hand, a greater and statistically significant difference was observed in the Creole population: 55.5% in the urban area and 74.3% in the rural area [OR 2.25 (1.15-4.42) p < 0.016]. With regard to the electrocardiographic studies, the prevalence of ECGA was 26.9% among Wichi and 33.1% among Creoles (Table V), with an average age of 46 and 52 years, respectively (data not shown). In the population with negative serology for Chagas disease, the frequency of altered ECG was 17.1 and 21.6, respectively. As seen in Table VI, the most common ECGA in the Wichi population was the left anterior hemiblock (LAHB), which was observed in 36.4% of patients with pathological ECG, either as an isolated or associated abnormality. A group of six patients (10.9%) had incomplete AHB (ILAH). Also frequent were primary ventricular depolarization abnormalities (PVRA), which accounted for 21.8% of heart disease detected by ECG. The right bundle-branch block (RBBB) was observed in only one patient in the study group (1.8%). No atrioventricular block or bradycardia, which suggests sick sinus syndrome, was observed. Mild ventricular arrhythmia was observed. In 16.4% of patients, there was a QRS-axis shift greater than -30°, with no other influencing factors. In the Creole population, the findings were 27.5% of LAHB, 22.5% of ILAHB, 10% of PVRA and 5% of IRBB. Again, RBBB was low (10%), but it was higher than that observed in the Wichi population (OR 6.0). In 17.5% of these patients, the QRS complex axis presented a left shift greater that -30°. In both populations, all patients were asymptomatic, with no cardiovascular history. Only three patients with previously undetected hypertension in the community of Wichi and seven in the Creole population had risk factors for heart disease. All of these patients were older than 60 years. DISCUSSION In the studied area of El Impenetrable, in the province of Chaco, Argentina, the prevalence of Chagas disease was very high. In fact, the results indicate that the serological prevalence was more than 10 times higher in both Wichi and Creole populations than the average for the country that was reported by Moncayo and Silveira (2009). The differences found between the two populations were related to habitat rather than ethnicity. Indeed, the highest prevalence was observed in individuals who live in rural areas and there was a far greater impact on children, which clearly demonstrates the increased risk associated with rural habitat. In fact, houses are quite different in rural and urban areas and the presence of vectors is much higher in villages. In villages, houses are precariously made with adobe and straw roofs, facilitating the colonization by vectors. Urban houses are made of brick instead of adobe. Remarkably, the major difference between rural and urban people in the adult population is seen in Creoles. This finding is expected considering that, most likely, the Wichi adults were born in rural houses and moved, already infected, to the urban area following the establishment of a Wichi neighborhood in Misión Nueva Pompeya in the 80's. It is noteworthy that even before the age of 20, the infection rate reaches 50% and that there is a marked difference in children who live in rural places (29.5%) and urban areas (4.6%). These results clearly show the importance of implementing health policies to tighten control, epidemiological surveillance and maintenance of sustainable health measures over time. Chronic Chagas heart disease occurs in Argentina with a frequency ranging from 25-30% of chagasic people, depending on the authors and the studied area (Rosenbaum & Alvarez 1955). Similar results have been obtained in Brazil (Laranja et al. 1956). These reports agree with the results found in the present paper, in which the incidence of ECGA was 26.9% in Wichis and 33.1% in Creoles, with an apparently slightly higher incidence in men, but statistically not significant (Wichi: 32% in men vs. 23% in women, Creole: 34.8% vs. 29.4). Regarding the characteristics of ECGA, the predominating ones are intraventricular conduction disturbances (IVCD), ventricular arrhythmias and PVRA (Santamarina 1981), which are nonspecific abnormalities that occur on an isolated or associated basis. In most studies performed with seropositive patients in endemic areas, RBBB is the most frequent abnormality. Thus, Rosenbaum and Alvarez (1955) reported RBBB in 55.7% of patients with chagasic heart disease in Argentina, whereas according to Santamarina (1981), RBBB accounts for 72.3% of IVCD, alone or associated with LAHB or, less frequently, with left posterior hemiblock. In Brazil, Laranja et al. (1956) reported a prevalence of 48.3% for RBBB. In contrast to these results, in a study of a community of Toba migrating from the province of Chaco to the city of Rosario, 28% of chagasic patients were diagnosed with ECGA and RBBB was detected only in 13.5% of them (Dávila et al. 1987). Interestingly, these authors noted that the prevalence of LAHB is significantly higher in individuals who had spent more than 20 years in highly endemic areas. These findings are consistent with the results of the present work, which reports that LAHB was the most common disorder, found in 36.4% of chagasic Wichi individuals and in 37.8% of the Creole population, all of them being permanent residents in highly endemic areas. It is interesting to note that this disturbance was predominantly present in asymptomatic individuals younger than 50 years (before age 40 in Wichi) who had normal clinical examinations and no clinical evidence of other pathologies that may be causing the disturbance. Asymptomatic and unrecognized arterial hypertension was detected only in three Wichi and four Creole individuals. In this study, RBBB was very rare and had a clear tendency for lower prevalence in the Wichi population: 1.8% in Wichi vs. 10% in Creoles or 6.0. These results were similar to those reported by Basso et al. (1978) in a 30-year follow-up study of the Creole and Huarpe populations in the province of Mendoza. The frequency of RBBB was also close to the one reported by Dávila et al. (1987) in the community of Toba of Rosario. In contrast, RBBB frequencies were significantly lower than those reported by other authors (Rosenbaum & Alvarez 1955, Santamarina 1981). The results of this work do not allow for a possible explanation of these differences; however, a very interesting perspective opens up for the study of the dynamics of infection and disease in this hyperendemic area, with a population that has been cohabiting with the vectors and the parasite since ancient times. In this sense, the low prevalence of RBBB is worth noting, particularly in the Wichi population. Additionally, the presence of this disturbance in 1/13 non-chagasic Wichi individuals and 3/18 of serologically negative Creoles, suggests that Chagas disease would not have a particular impact on the rate of occurrence of RBBB on these populations, at least in the group studied here. The same tendency was observed in relation to PVRA and LAHB, which show similar frequencies of ECGA in chagasic and non chagasic populations (data not shown). Further studies will be needed to confirm this trend and to try to find its causes. The influence of the triad host-parasite-environment still remains unknown. Although there are numerous studies on the influence of the parasite strain or lineage, this does not seem to be the only factor involved and there is a considerable degree of controversy in this regard. Thus, Sanchez-Guillen et al. (2006) state that, "the relationship between genotypes and biological characteristics in T. cruzi strains is still debated and not clearly understood". Also, Añez et al. (2004) reported that, "the predominance of T. cruzi I human isolates in Venezuela allied to the higher prevalence of severe symptoms of Chagas disease in patients infected by this lineage do not corroborate an innocuousness of T. cruzi I infection in humans". Moreover, regarding the genetic characteristics of the host, the Creole and Wichi populations in our study show no difference either in terms of susceptibility to infection or in terms of the incidence and profile of heart disease, except for the difference in the incidence of RBBB, which must be confirmed with further cases. This finding, however, does not rule out possible genetic influences, taking into account that the definition of "Creole" makes reference to a product of miscegenation between the Spanish and Indigenous populations. Finally, the environment, including customs, food and other factors that have not been clearly identified to date, could also influence the dynamics of infection, including the natural resistance of individuals who have lived with the parasite and the vector for more than 60 years, but do not become infected or who do not develop antibodies against the parasite. In short, according to the opinion of Devera et al. (2003), it is likely that "the interaction of the different infecting clones of the T. cruzi complex and the human host will determine the morbidity of the disease". In conclusion, from the healthcare aspect, this work clearly demonstrates the need for an active policy of continuous and sustainable prevention in this large area of our country. In this regard, Briceño (2007) clearly demonstrates the social and economic benefits of Chagas disease prevention. Similarly, Pinto and Borges-Dias (1979) address the social and cultural aspects that should be taken into account for the prevention and control of endemic Chagas disease. From the perspective of heart disease, the present paper shows a reality that differs from that which is classically accepted and raises some questions that cannot be answered with the current knowledge of the subject. ACKNOWLEDGEMENTS To Maria Cristina Dasso, Zelda Franceschi and Anna Ciannameo, who carried out anthropological studies prior to the execution of this work and the bilingual informed consent (with the colaboration of members of community of Wichi), to Patricia Gil, Andrea Tarditti and Olga Zorrilla, who took and prepared blood samples and carried out serological testings, to Diego Gauna, who colaborate in medical studies, to Dr Juan Beloscar, who kindly performed a blind analysis of ECG studies, to Maria Luisa Sánchez and Sabina del Valle Maguna, who performed ECGs, to Ianina Moretti Basso, who helped with the execution of promotional and secretarial tasks in the field, Julio Sosa, who helped us as truck driver and in the field tasks, to María Elena Polo and Fabián Matorras, members of the community of Wichi, who helped explain the study and the informed consent requirements, to the Director and medical and nursing staff of the Nueva Pompeya Hospital, to the Directors and staff of the local FM radio stations, to school teachers and community leaders in Nueva Pompeya, to Maria Fernanda Garstein, for editing and sharpening the translation to prepare the manuscript for publication, to Ministerio de Salud de la Provincia del Chaco and to the Dirección de Epidemiología y Servicio Provincial de Chagas. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10105t6.jpg] [oc10105t4.jpg] [oc10105f1.jpg] [oc10105t1.jpg] [oc10105f2.jpg] [oc10105t5.jpg] [oc10105t3.jpg] [oc10105t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}