 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 5, 2010, pp. 712-716 SHORT COMMUNICATIONS Molecular characterization of adenoviruses from children presenting with acute respiratory disease in Uberlândia, Minas Gerais, Brazil, and detection of an isolate genetically related to feline adenovirus Lysa Nepomuceno LuizI; José Paulo Gagliardi LeiteII; Jonny YokosawaIII, +; Bruno M CarneiroI; Edson Pereira FilhoII; Thelma Fátima de Mattos OliveiraI; Guilherme Ramos Oliveira e FreitasI; Lourenço Faria CostaI; Nayhanne Tizzo de PaulaI; Hélio Lopes da SilveiraIV; Júlio César NepomucenoV; Divina Aparecida Oliveira QueirózI ILaboratório
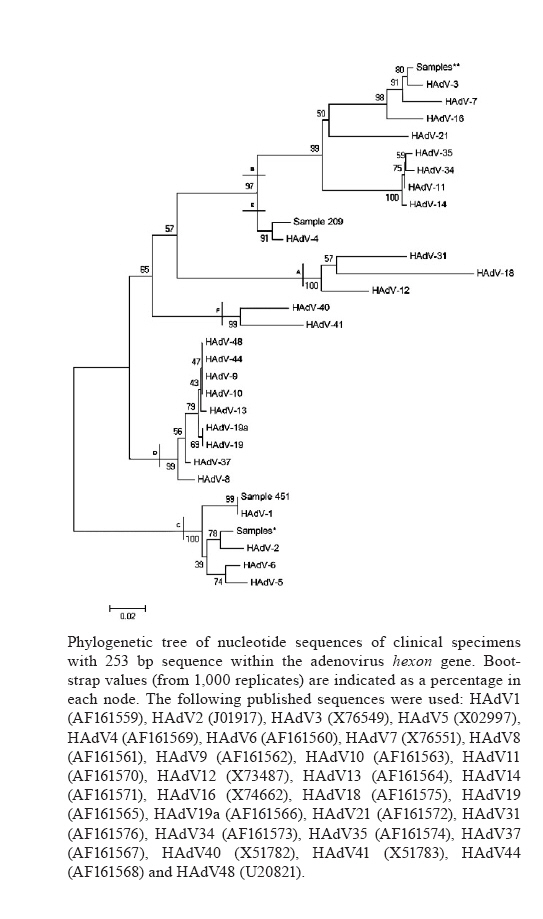
de Virologia, Instituto de Ciências Biomédicas + Corresponding author: j.yokosawa@uol.com.br Received 25 October 2009 Code Number: oc10120 ABSTRACT Human adenoviruses (HAdV) are a major cause of acute respiratory diseases (ARD), gastroenteritis, conjunctivitis and urinary infections. Between November 2000-April 2007, a total of 468 nasopharyngeal aspirate samples were collected from children with ARD at the Clinics Hospital of Uberlândia. These samples were tested by immunofluorescence assay (IFA) and 3% (14/468) tested positive for the presence of HAdV. By performing polymerase chain reaction (PCR) to detect HAdV DNA in samples that tested negative or inconclusive for all viruses identifiable by IFA (respiratory syncytial virus, parainfluenza viruses 1, 2 and 3, influenza viruses A and B and HAdV), as well as negative for rhinoviruses by reverse transcription-PCR, additional 19 cases were detected, for a total of 33 (7.1%) HAdV-positive samples. Nucleotide sequences of 13 HAdV samples were analyzed, revealing that they belonged to species B, C and E. Further analyses showed that species C (HAdV-2) was the most prevalent among the sequenced samples. To our knowledge, this is the first report describing the presence of HAdV-4 in Brazil. We also detected an isolate that was 100% identical to a part of the feline adenovirus hexon gene sequence. Key words: adenovirus - acute respiratory disease - children Acute respiratory disease (ARD) is one of the major causes of morbidity and mortality among children under the age of five, especially in developing countries (Williams et al. 2002). Approximately 5% of these cases are associated with adenoviruses (HAdV) (Brandt et al. 1969). Furthermore, HAdV infections could account for severe lower respiratory infections in children (Murtagh et al. 2009). HAdVs are non-enveloped, double-stranded DNA viruses with a viral particle size ranging from 70-90 nm in diameter with icosahedral symmetry. These viruses belong to the Adenoviridae family, which consists of 54 serotypes (HAdV-1-54) and are classified into seven species (A-G) based on their physicochemical, biological and genetic characteristics (Horwitz 2001, Jones et al. 2007, Ishiko & Aoki 2009, Walsh et al. 2009). In addition to the determination of the etiological agent, the characterization of AdV in an infection is of important clinical interest because specific serotypes are frequently associated with the manifestation and severity of the disease (Hong et al. 2001). Indeed, HAdV-14 has recently emerged and has rapidly become a highly prevalent strain in regions of the United States, causing substantially more severe illnesses (Gray & Chorazy 2009, Lewis et al. 2009, Tate et al. 2009). In general, neutralisation or heamagglutination inhibition assays are used for HAdV serotyping (Swenson et al. 2003). However, serotyping can be done using immunofluorescence assay (IF) with serotype-specific monoclonal antibodies (Wood et al. 1997), genus-specific polymerase chain reaction (PCR) combined with restriction endonuclease digestion (PCR-restriction fragment length polymorphism) analysis (Allard et al. 2001) and sequence analysis (Sarantis et al. 2004). Studies conducted in Brazil reinforce the importance of HAdVs in ARD cases and they have been found as the second most frequent virus detected in nasopharyngeal aspirates (NPA) from children with ARDs in the cities of São Paulo (Moura et al. 2007) and Rio de Janeiro (Nascimento et al. 1991), located in South-eastern Brazil and Porto Alegre (Straliotto et al. 2002), located in Southern Brazil. The main objectives of the present paper were to detect HAdV in NPA specimens from children under the age of five suffering from an ARD and to determine the HAdV serotypes that are circulating in Uberlândia, state of Minas Gerais, in South-eastern Brazil. Between November 2000-April 2007, 468 NPA specimens were collected at the Clinics Hospital, Federal University of Uberlândia (UFU), and processed according to Oliveira et al. (2008) at the Laboratory of Virology at UFU. This project was approved by the UFU Ethical and Research Council. Due to the limited amount of specimen that could be collected from each child, the initial screening was carried out by IF using the Respiratory Panel I Viral Screening and Identification kit® (Chemicon International, Millipore, Temecula, CA) according to the manufacturer's instructions. This kit was used for the detection of respiratory syncytial virus (RSV), parainfluenza viruses 1, 2 and 3 (PIV 1, 2 and 3), influenza viruses A and B (Flu A and B) and HAdV. We followed the classification of results (positive, negative or inconclusive) established by Queiróz et al. (2002). RNA was extracted from IF-negative/inconclusive samples with Trizol® (Invitrogen Corp, Carlsbad, CA), following the manufacturer's instructions. Reverse transcription-PCR (RT-PCR) was used to detect rhinovirus RNA as previously reported (Costa et al. 2006). The remainder of each specimen was used for the detection of HAdV. Two rounds of detection PCR (Araújo et al. 2001) were used to amplify a 107 bp segment of the HAdV hexon gene from samples that tested negative/inconclusive by IF and also tested negative for rhinovirus by RT-PCR. The only modification made in the protocol was the addition of one deoxyribonucleotide residue in the forward primer (5'- TGA CTT TTG AGG TGG ATc CCA TGG -3'). Standard precautions were followed in all procedures to avoid cross-contamination. In order to determine the serotypes of HAdV-positive specimens (detected by IF or PCR), we used a characterization PCR assay (Allard et al. 2001) to amplify a 301 bp portion of the hexon gene and the amplicons were subsequently sequenced. The specimens that did not produce amplicons were inoculated into A-549 cells to increase the number of virus particles (Rosete et al. 2008). DNA was extracted from cell scrapes and retested using the characterization PCR assay. PCR amplicons of the expected size (301 bp) were purified using the QIAquick PCR purification kit® (QIAGEN). Both strands were sequenced using the ABI Prism Big Dye Terminator Cycle Sequencing Ready Reaction Kit® (PE Applied Biosystems, Foster City, CA, USA). Sequence editing and analysis were performed using BioEdit (Hall 1999) and MEGA 3.1 by the neighbour-joining method (Kumar et al. 2004), respectively. Out of 468 samples tested by IF, 3% (14/468) were positive for HAdV. In addition, among the 126 specimens that tested negative for respiratory viruses in the IF assay (RSV, PIV 1, 2 and 3, Flu A and B) and for rhinoviruses using RT-PCR (Costa et al. 2006), 19 positive samples were obtained using the PCR detection assay. This increased the total rate of HAdV-positive specimens to 7.1% (33/468). This rate (7.1%) is similar to the rate (6%) in Southern Brazil described by Straliotto et al. (2002). However, other studies carried out in Brazil reported prevalence rates that varied from a slightly higher rate (9.9%) for cases in the Northeast (de Arruda et al. 1991), to a slightly lower rate (4.6%) in the Southeast (Vieira et al. 2001) and a much lower rate (0.8%) in the South (Tsuchiya et al. 2005). Although IF is a more affordable and rapid diagnostic method, PCR-based assays are also of great importance due to their higher sensitivity in the detection of HAdV (Larrañaga et al. 2007). In this study, PCR allowed us to increase the detection rate from 3%, based only on the IF assay, to 7.1% by combining IF and PCR results. The seasonal distribution pattern obtained in this study revealed that HAdV cases occurred in all seasons, similar to the results reported by Cabello et al. (2006). However, in our study approximately half of the cases were detected in the autumn. The high number of cases observed during this season may be due to a higher number of patients with ARD attending the hospital. The median age of the patients was 13 months old (range: 3-60 months) and upper respiratory tract infection was verified in approximately 66.7% (8/12) of the cases. Of the total 33 HAdV positive specimens, 31 NPAs were tested using the characterization PCR assay (2 of the samples lacked enough material to be tested). Ten of these samples tested positive and were subsequently sequenced. The remaining 21 samples were inoculated into cell culture (A-549) and their DNA was extracted from cell scrapes. From these, six additional PCR-positive samples were obtained. However, due to the insufficient amount of PCR products, only three of them were sequenced, providing a total of 13 sequenced samples. Some factors may have contributed to the limited number of specimens that tested positive using the PCR method described by Allard et al. (2001). NPAs were collected within five days after the onset of symptoms and it is possible that some of the specimens collected on the 5th day contained a low number of infected cells and/or had a low virus titre. In addition, we used freshly collected cells in the IF assay and stored specimens for PCR and inoculation of cell culture. Moreover, detection PCR was performed in two rounds (nested PCR), while characterization PCR was carried out in one round. Lastly, the use of fresh samples would probably help to increase the number of positive specimens for characterization, but performing the test daily would be impractical and cumbersome. Identification of the nucleotide sequences from a highly conserved region among various serotypes that allow for characterization for the development of a two-round PCR assay would increase the sensitivity of detection and allow for the characterization of more specimens. However, this task is very difficult and is a subject for another study. Through a BLAST (http://blast.ncbi.nlm.nih.gov) search with sequences obtained in this study, we determined different HAdV genotypes: eight sequences were highly identical to HAdV of species C (7 HAdV-2 and 1 HAdV-1), four sequences were identical to species B (HAdV-3) and one sequence to species E (HAdV-4). Furthermore, a phylogenetic tree was constructed (Figure) using the sequences obtained in this study and 27 different HAdV reference sequences (Allard et al. 2001) obtained from GenBank (http://www.ncbi.nlm.nih.gov/Genbank), which corroborated the results obtained using BLAST. A different circulation pattern was observed in São Paulo by Moura et al. (2007) in samples collected between March 1995-March 1996 and between April 2000-April 2001. The most prevalent serotype from this study was HAdV-7 (56.7%), followed by HAdV-1 (26.7%), HAdV-3 (6.7%), HAdV-2, HAdV-5 and HAdV-6 (3.3% each). However, in that study samples were only collected from hospitalized children. Our study included samples collected from children who presented ARD at the Paediatric Emergency Service, the Paediatric Ward, the Paediatric Intensive Care Unit and the Neonatal Intensive Care Unit. In this study, a characterization into serotypes was also performed in silico. This was accomplished by determining the presence of restriction sites listed in the flowchart proposed by Allard et al. (2001). Four specimens of HAdV-3 belonged to the type 3p genome. This serotype was previously observed in patients with either respiratory disease or conjunctivitis in the cities of Belém (North Brazil) and Rio de Janeiro (Southeast) (Kajon et al. 1999). Through nucleotide sequence analysis, we determined that eight specimens were from species C. Due to the limitations of the protocol proposed by Allard et al. (2001), caused by the lack of other restriction sites in the amplicons, the serotypes of seven specimens could not be determined and might be HAdV-2, HAdV-5 or HAdV-6. However, a BLAST search showed the highest identity to HAdV-2. Nevertheless, the presence and absence of certain restriction sites in their nucleotide sequences confirmed the results obtained in the phylogenetic analysis and BLAST search. Although serotype HAdV-4 is frequently associated with ARD in military recruits (Kolavic-Gray et al. 2002), one specimen of this serotype was identified in a two-year-old child. The nucleotide sequence was 100% identical to the HAdV-4 isolated from basic training recruits in United States of America during the end of the 1990s (Blasiole et al. 2004). This serotype was also found in Japan, where it was associated with cases of conjunctivitis (Miura-Ochiai et al. 2007). To our knowledge, this is the first description of serotype HAdV-4 in Brazil. In addition, we found the nucleotide sequence of specimen AdV-UDI-451 to be 100% identical to two feline AdV sequences (Lakatos et al. 1999, and data reported in GeneBank accession AY512566). One of these sequences was detected in a cat that suffered from a transient hepatic failure (Lakatos et al. 1999). A similar result was found by Phan et al. (2006), who reported that the amino acid sequence of the AdV hexon gene, obtained from the stool specimen of a one-year-old child with gastroenteritis in Japan, grouped together with the feline adenovirus sequence AY512566 in a phylogenetic analysis, suggesting that HAdV-1 may be transmitted from felines to humans and/or vice versa. However, a cat was not kept at the family's house and it was not clear whether there was contact with the animals that lived in the surrounding area. In our study, we did not determine whether the family of the HAdV-1-infected child had a cat. In conclusion, using a combination of IF and PCR methodologies allowed us to determine a 7.1% prevalence rate of HAdV infection in clinical samples from children presenting with ARDs in Uberlândia. Furthermore, HAdV-2 was the most prevalent serotype found among the HAdV specimens. HAdV-4, which had not been previously described to circulate in Brazil and an isolate with strong similarity to the feline AdV were also found. ACKNOWLEDGEMENTS To Dr. Dean D Erdman, Centers for Disease Control and Prevention, and to Dr. Marilda Siqueira, Laboratório de Vírus Respiratórios e Sarampo, IOC-Fiocruz, for providing the Respiratory Panel I Viral Screening and Identification kit, and to the laboratories of Immunology, Parasitology, Molecular Biology, Physiology and Genetics, UFU, to permit us to use their facilities and the health care professionals of the Clinics Hospital of Uberlândia for the screening of patients. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10120f1.jpg] |
| |||||||||

{kind=link}