 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 5, 2010, pp. 722-728 TECHNICAL NOTES Evaluation of Lionex TB kits and mycobacterial antigens for IgG and IgA detection in cerebrospinal fluid from tuberculosis meningitis patients Isabela Gama SardellaI; Mahavir SinghII; Susanne KumpferII; Rafael Ribeiro HeringerIII; Maria Helena Féres SaadI, +; Marzia Puccioni SohlerIII ILaboratório
de Microbiologia Celular, Instituto Oswaldo Cruz-Fiocruz, Av. Brasil 4365, 21045-900
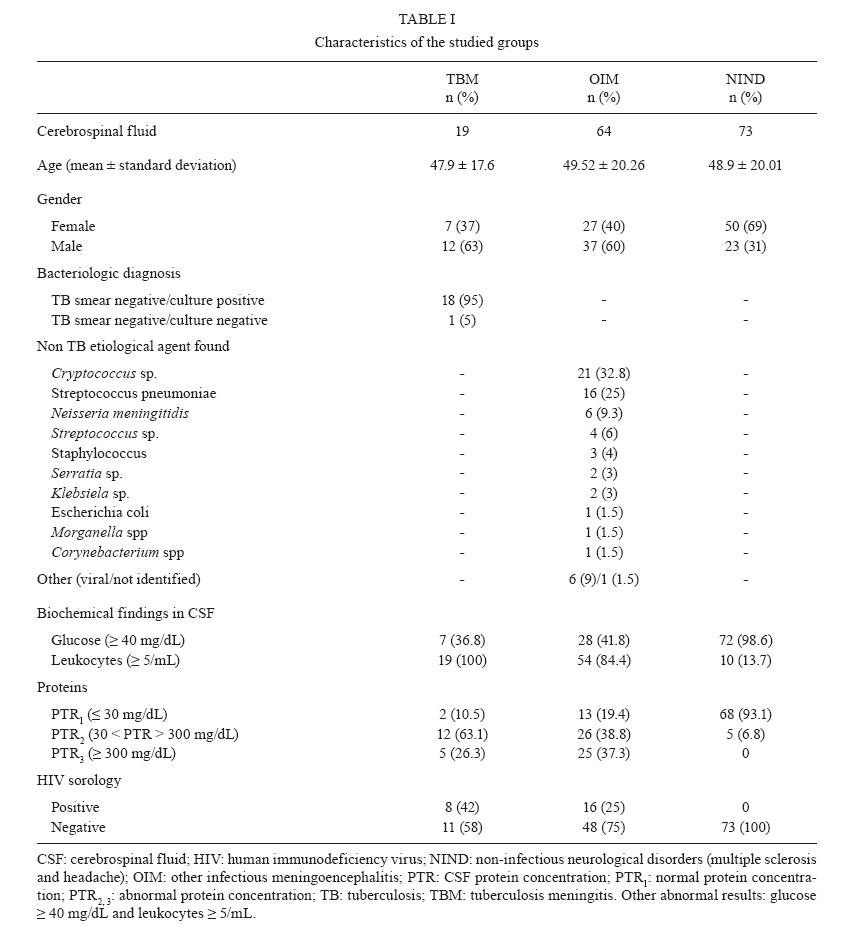
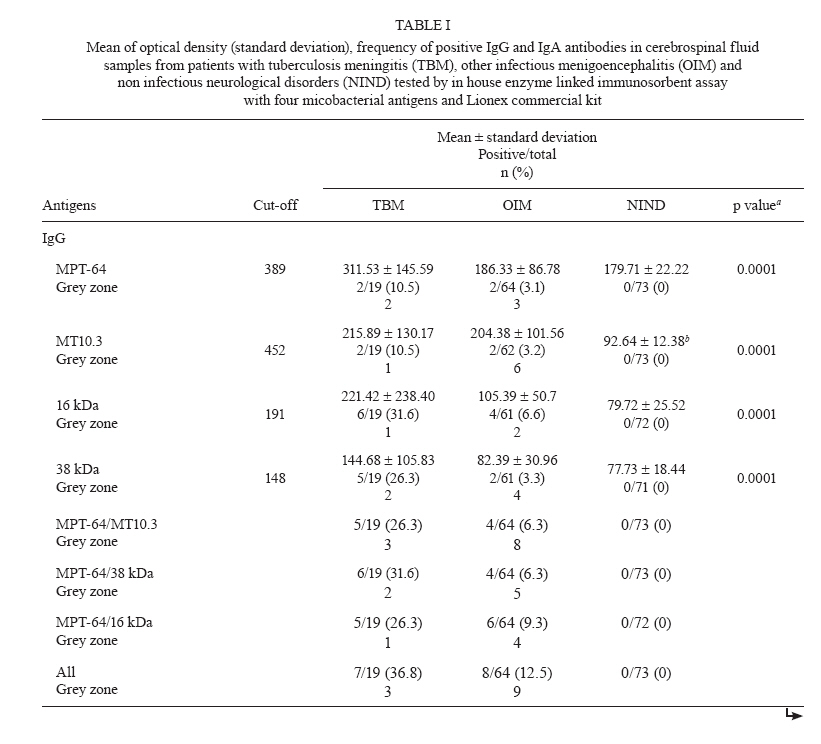
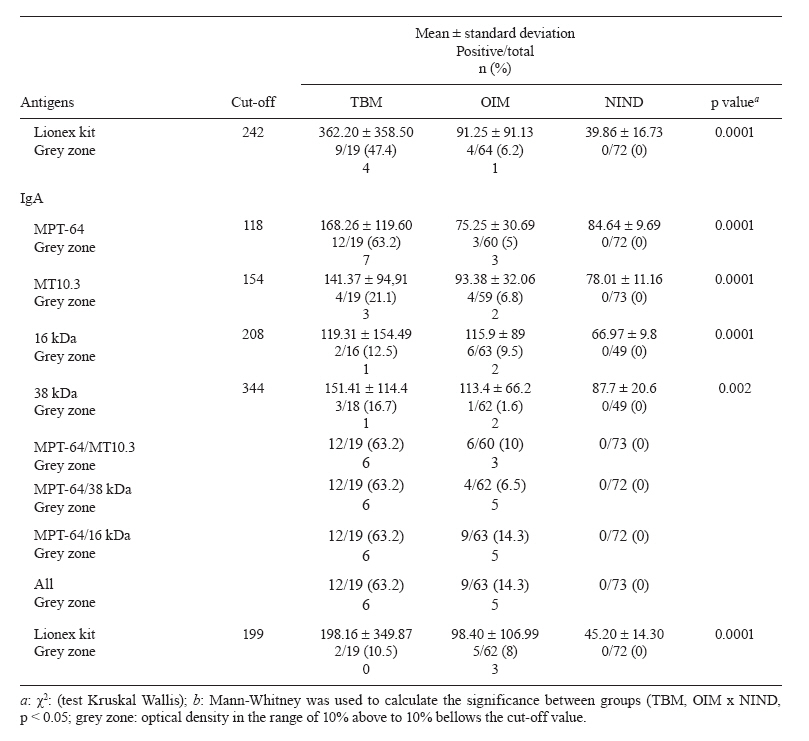
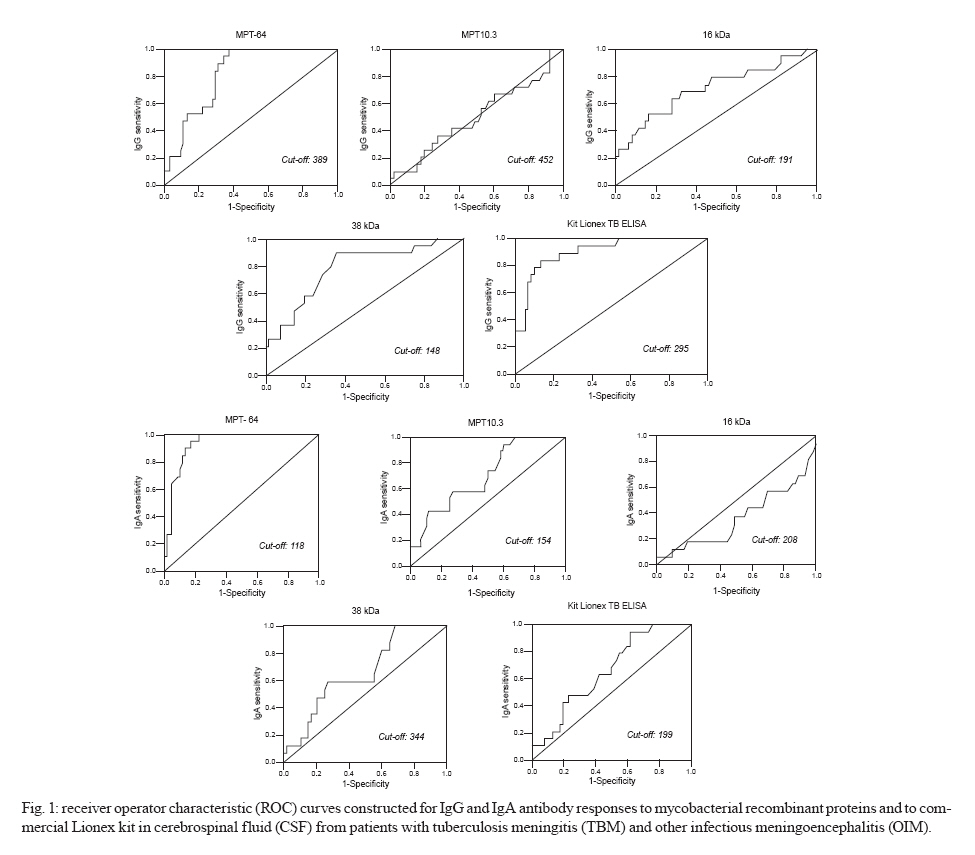
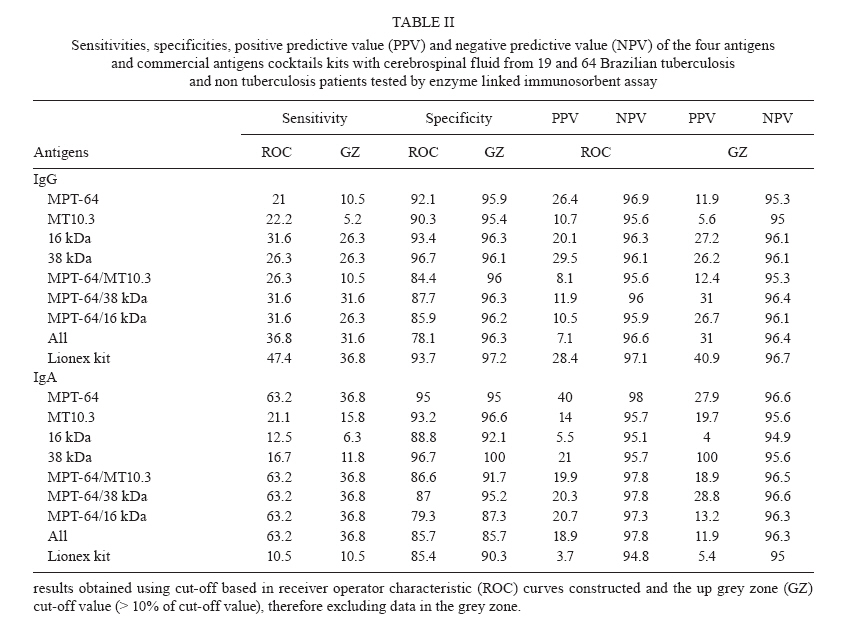
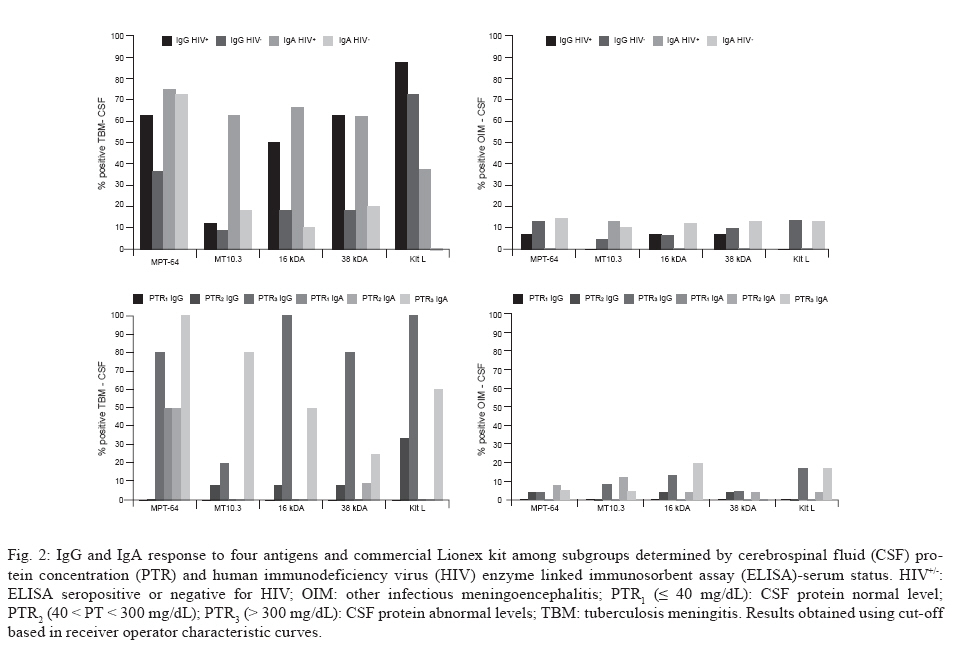
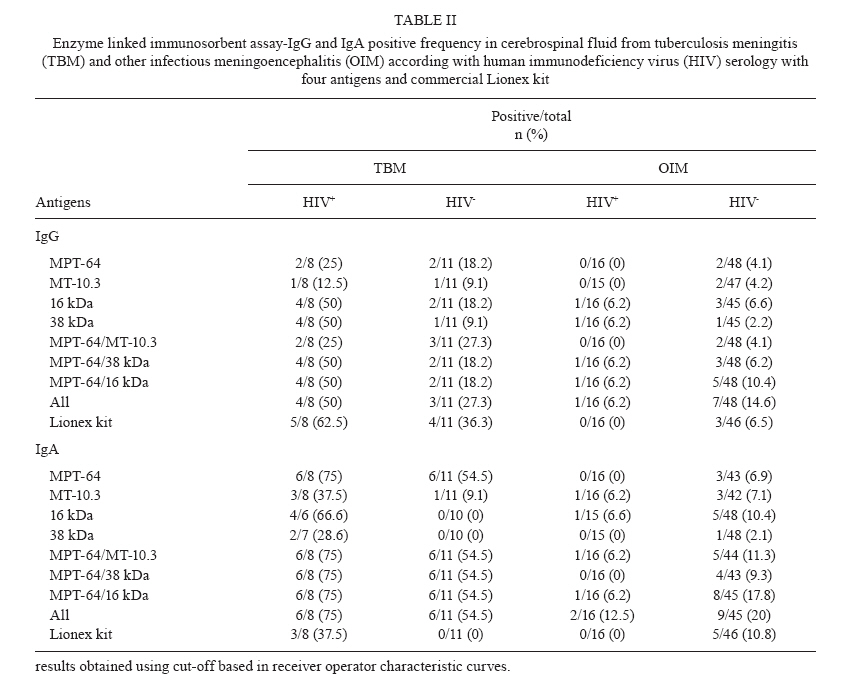
Rio de Janeiro, RJ, Brasil + Corresponding author: saad@ioc.fiocruz.br Received 28 October 2009 Code Number: oc10123 ABSTRACT To evaluate commercial Lionex TB together with four antigens of Mycobacterium tuberculosis (MPT-64, MT10.3, 16 kDa and 38 kDa) for IgG and IgA cerebrospinal fluid (CSF) detection in the diagnosis of tuberculosis meningitis (TBM) with CSF negative acid-fast bacilli staining, 19 cases of TBM, 64 cases of other infectious meningoencephalitis and 73 cases of other neurological disorders were tested by enzyme linked immunosorbent assay. IgA-MPT-64 and IgG Lionex showed the highest sensitivities, specificities, positive predictive value and negative predictive value (63.2%, 47.4%; 95%, 93.7%; 40%, 98% and 28.4%, 97.1%, respectively). However, while grey zone was 12.7% and 6%, respectively, lowering sensitivity but maintains high specificity (> 95%). High protein concentration in CSF was associated with antibody positivity CSF/HIV+ which did not influence the sensitivity of both tests. To our knowledge, this is the first description of IgA-MPT-64 and IgG Lionex antibodies in CSF-TBM and, although there is good specificity, adjustments are needed based on antigen composition to enhance sensitivity. Key words: tuberculosis - cerebrospinal fluid - ELISA - meningoencephalitis tuberculosis - Mycobacterium tuberculosis - immune response Tuberculosis (TB) remains a major cause of morbidity and mortality, principally in developing countries where the disease is endemic and exposure to the bacilli is more frequent. Diagnosis of TB is difficult, mainly in extrapulmonary cases, because clinical symptoms are unspecific and specimens for diagnosis are difficult to obtain. TB meningitis (TBM) is a common clinical manifestation involving infection of the central nervous system with Mycobacterium tuberculosis. Delay in diagnosis and treatment leads to neurologic handicap and mortality (Quan et al. 2006). Usually, TBM diagnosis is made by clinical suspicion associated with cerebrospinal fluid (CSF) biochemical findings and protein concentration measurement is an important tool for early recognition of neurological disease; however, abnormalities may suggest TBM but do not differ significantly from those observed in other types of infectious meningitis (Thompson 1995). Brazil is the second major TB endemic country in Latin America and TBM comprises 4% of all extrapulmonary cases. The incidence rate of all clinical forms of TB is 48/100,000 inhabitants. In large, crowded cities such as Rio de Janeiro, it is 75/100,000 and the TBM incidence rate is 0.34/100,000 (MS/SVS 2006, WHO 2009). Ziehl Neelsen acid-fast bacilli (AFB) staining is the most commonly used laboratory method to diagnose TB; however, in extra-pulmonary TB, the sensitivity is too low (10-40%) and culture is more sensitive (50-70%) but time-consuming (Garg 1999, Chandramuki et al. 2002, Thwaites et al. 2004). Newer diagnostic methods based on nucleic acid amplification tests have been developed, but meta-analysis studies have indicated that despite high specificity, the sensitivity is lower and variable (Pai et al. 2003, Dinnes et al. 2007). T cell based assays detecting INF-γ production have been reported to be promising; however expense, the requirement of fresh clinical specimens and inadequate laboratory infrastructure limit their use in low-income countries. There is an urgent need and a high demand for low cost, rapid TB diagnostic tests, principally for paucibacillary cases. Antibodies such as IgG and IgM produced against M. tuberculosis antigens in the CSF of patients with TBM have been reported but with a variable range of sensitivity (Kadival et al. 1994, Patil et al. 1996, Wang et al. 2005). Commercial serological antibody detection tests are sold in developing countries; however, most of them have not been submitted for an accurate evaluation in our set (Steingart et al. 2007). The aim of this paper is to evaluate the Lionex TB enzyme linked immunosorbent assay (ELISA) kits and a series of M. tuberculosis antigens such as MPT-64 (Rv1980c), MT10.3 (Rv3019c), 16 kDa (2031c) and 38 kDa (Rv0934), supplied by Lionex Diagnostics & Therapeutics, for IgG and IgA detection in smear-negative AFB CSF/TBM patients. The commercial kit and in-house ELISA with antigens are described in Appendixes. The study was done in CSF obtained from 2004-2006 and stored at University Hospital Clementino Fraga Filho of the Federal University of Rio de Janeiro (HUCFF/UFRJ) and Neurolife Laboratory Ltda, Rio de Janeiro, Brazil, where they were maintained at -20°C. All CSF samples were analyzed for total and differential cell count, biochemistry and smears for Gram and AFB staining according to routine laboratory methods and data were collected from medical records. A total of 156 CSF samples, most of them investigated for TBM suspicion, were included from patients living in the city of Rio de Janeiro and classified into three groups by diagnosis: (i) TBM patients with proven TBM by M. tuberculosis positive culture, except one patient who responded positively to the specific antituberculosis treatment. All were negative for AFB smear; (ii) other infectious meningoencephalitis (OIM) patients with proven diagnosis of meningitis caused by other microorganisms detected by CSF staining and/or culture with good clinical response to broad-spectrum treatment; (iii) non-infectious neurological disorders (NIND) patients that had chronic intractable headache or multiple sclerosis, included as endemic area controls. Table I (Supplementary data) describes the characteristics of the studied groups and the number of patients with abnormal findings in CSF such as: amount of glucose > 40 mg/dL, leukocytes > 5/mL and protein (PTR2: protein average from < 30 - > 300 mg/dL and PTR3: amount of protein > 300 mg/dL. PTR1: amount of protein < 30 mg/dL was considered normal level). Human immunodeficiency virus (HIV) serology status was obtained by the ELISA Genscreen test (BioRad, France). The study was approved by the ethical committees of the HUCFF/UFRJ and Oswaldo Cruz Institute (411/07). There were statistically significant differences in the average antibody levels detected in CFS-TBM and all non-TB cases with both commercial and in-house tests (p < 0.002), except for IgG-MT10.3, which did not show a difference between TB and OIM groups. The highest mean levels of IgG and IgA in CSF-TBM were obtained with the Lionex TB kit followed by MPT-64 (Tables Ia & b). According to receiver operator characteristic (ROC) analysis, displayed in Fig. 1, sensitivity with the Lionex TB IgG kit was 47.4% and the specificity was 93.7%. Assuming a TBM general prevalence of 5%, a positive predictive value (PPV) and a negative predictive value (NPV) of 28.4% and 97.1%, respectively, was found. Of the total CSF samples tested, 6% (5/83) were situated in the grey zone and, using the upper grey zone cut-off value, sensitivity decreased to 36.8% (7/19) with better specificity (93.7-97.2%) and thus leads to a slight increase in the PPV (40.9%). The IgA Lionex kit was less reactive and also produced a lower number of samples in the grey zone (3.7%, 3/81) (Tables Ia & b, II). Among the single antigens tested with the TBM group, one CSF sample reacted with all antigens for both isotypes, but the majority selectively recognized MPT-64, mainly the IgA isotype (12/19), followed by 16 kDa and 38 kDa antigens primarily for IgG. Five CSF-TBM samples did not react to any of the single antigens tested. Thus, according to ROC analysis (Fig. 1), the highest sensitivity (63.2%) and specificity (95%) were obtained with IgA-MPT-64 and addition of other antigens results did not improve this data (Tables Ia & b, II). These results reflect a PPV of 40% and a NPV of 98% (Table II). Nevertheless, 12.7% (10/79) of the CSF samples were classified in the grey zone and, as in the IgG Lionex kit, had decreased sensitivity (36.8%, 7/19) and, opposite to the commercial test, had lower PPV (27.9%) without affecting NPV or specificity (Tables Ia & b, II). While MPT-64 was preferentially recognized by IgA, for 16 kDa and 38 kDa, IgG antibodies were present in the CSF with sensitivities and specificities of 31.6% and 26.3% and 93.4% and 96.7%, respectively. Both 16 kDa and 38 kDa had PPV < 30% and NPV H" 96%. For IgG, cumulative values of all antigens tested increased the sensitivity to 36.8%, compared to single antigens and their combinations tested, but lowered specificity (Tables Ia & b, II). Although these antigens demonstrated good NPV, all exhibited lower PPV. The grey zone among these antigens is depicted in Tables Ia & b and the CSF samples situated in this area ranged from 3.7-13.6%, with lowered sensitivity and PPV and slightly increased specificity and NPV, compared to ROC analysis (Fig. 2, Tables Ia & b, II). Among those with abnormal PTR levels, Lionex IgG detected all PTR3 and 33.3% of PTR2. The Lionex IgA kit was less reactive. For single antigens, most of the CSF-TBM/PTR3 reacted positively to IgG-MPT-64, 16 kDa, IgA-MPT-64, MT10.3 and to all combinations with MPT-64. Half of the CSF-TBM/PTR2 and PTR1 samples exhibited positive results only with IgA-MPT-64 (Fig. 2). None of the samples in the CSF-NIND group exhibited PTR3 levels, nor did they react with either the commercial kit or in-house tests (Tables Ia & b). All measured cross reactions belonged to CSF samples from patients with meningitis caused by microorganisms such as Streptococcus pneumoniae and Cryptococcus spp, but neither commercial nor in-house tests. Events of cross reactions were observed only in OIM group. These patients developed meningitis caused by microorganisms such as S. pneumoniae and Cryptococcus spp, but neither commercial nor in-house tests exhibited OIM-PTR1 reactivity. Interestingly, HIV infection had no influence on the results obtained with Lionex TB ELISA kits or single antigens tested and, surprisingly, TB meningitis/HIV+ patients displayed higher sensitivity when compared to the corresponding HIV- patients. On the other hand, there was a lower proportion of antibody positivity for CSF-OIM samples from patients co-infected with HIV (Fig. 2, Table II, Supplementary data). TB meningitis and pleural TB involve a mucosa/serosa infection with which IgA is usually associated. The data presented in this study reveal that predominantly IgA antibodies are present in the CSF of TBM patients and that, among a panel of recombinant antigens tested, only MPT-64 yielded promising results in detecting IgA antibodies in CSF. In previous studies with pleural TB patients, the predominance of IgA was also noted to react to MPT-64 and a combination of MPT-64 and MT10.3 slightly increased the sensitivity (Kaisermann et al. 2005). In the present study with CSF, IgA reactivity was also mainly obtained for MPT-64 (63.2%) and combination with two or all antigens, including MT10.3, did not increase this sensitivity. However, analysing the test with OD values in the upper grey zone resulted in decreased sensitivity and raised the problem of interpreting intermediate results in clinical practice. For antigen-specific IgG in CSF of TBM patients, 16 kDa and 38 kDa performed better (31.6% and 26.3%) than MPT-64 (21%), but in contrast to IgA, combinations of all antigens led to a slight increase in sensitivity (36.8%) but lowered the specificity. These data corroborate findings that most TB patients develop an antibody-mediated immune response to mycobacterial antigens, but the predominant isotype elicited may be dependent not only on the antigen but also on the site of infection (Chandramuki et al. 2002, Gaseitsiwe et al. 2008). Nevertheless, some of the patient samples were not recognized by any of the recombinant proteins tested, which indicates that single antigens, even those of immune dominant response, must be combined with other molecules that may be recognized by less responsive patients (Raja et al. 2008). In this respect, the appropriate antigen cocktail developed by Lionex in the IgG commercial kit resulted in higher sensitivity, compared to single antigens tested, but, like IgA-MPT-64, 6% of CSF was linked to the grey zone and using a more restricted cut-off based on the upper grey zone cut-off value lowered the sensitivity of the commercial kit (36.8%) but increased the specificity and PPV, compared to ROC analysis. It is important to stress that infection with HIV did not have any adverse effect on the sensitivities obtained with IgA MPT-64 or the Lionex IgG kit containing multiple antigens. Despite the small sample size, our findings confirm previous studies with MPT-64 (Chandramuki et al. 2002). For the other antigens, co-infection with HIV appears to reduce antibody reactivity in CSF-OIM, but to induce reactivity in CSF-TBM, though without statistical significance. This finding may be related to antigen characteristics or to the fact that the mean level of leukocytes, proteins and glucose were higher among TBM/HIV+ (data not shown); however, as our sample is small, further investigation must be done to clarify the correlation of this finding with CD4 count, information that was not available in our sampling. IgG response in CSF has been explored by several authors. Chandramuki et al. (2002) reported lower sensitivity for MPT-64 (12%) and 38 kDa (8%) as compared to the results presented in this study with MPT-64 (21%) and 38 kDa (26.3%) using samples with similar characteristics (BAAR-negative/culture-positive). In contrast, previous studies with the 38 kDa antigen reported sensitivities of 41% and 80% (Kadival et al. 1994, Patil et al. 1996). Recently, Restrepo et al. (2008) described CSF-TBM positive proportions similar to our results for 38 kDa and 16 kDa with a similar number of CSF samples and Wang et al. (2005) detected higher proportions of antibodies for MPT-64, although they tested very few CSF samples. However, none of these authors performed grey zone analyses in their studies. The discrepancies in sensitivity may be related to the disease status of the studied population, for instance, a preferential recognition of certain specific antigens depending on the disease progression and/or due to genetic background of the different geographical population studied (Lyashchenko et al. 1998, Silva et al. 2003, Hoff et al. 2007). Another important question posed is the possibility of whether or not plasma antibodies synthesized in response to previous latent infection could serve as the major source of mycobacterial reactivity in CSF, even though the positive reactivity to mycobacterial antigens always correlates with TBM diagnosis. There is evidence of unspecific intrathecal antibody isotype production in TBM, OIM and NIND and a reported possibility that because of blood-brain barrier damage due to chronic infection by microorganisms, leakage of antibody into CSF occurs (Nerenberg et al. 1978, Kinnman 1981, Walsh & Tourtellotte 1986, Prabhakar et al. 1990, Restrepo et al. 2008). Unfortunately, patient sera were not available and comparison with CSF could not be made; hence, we cannot be sure that the mycobacterial specific antibodies were due to local production in the CSF. However, in the present series of CSF-NIND samples, there was no antigen-specific reactivity for either of the antibodies and the PTR3 level also was not detected. There are several reports of cross-reactive antibodies that may recognize very similar epitopes from unrelated targets and the antigen-specific antibodies detected in some CSF-OIM may be related to cross reactivity with other infectious microorganisms rather than previous mycobacterial latent infection (Michaud et al. 2003, Predki et al. 2005). In the CSF-OIM of the present series, which were infected with S. pneumoniae and Cryptococcus, a mycobacterial antigen-specific reaction was observed mainly for IgA-16 kDa and the Lionex kit. Recently, these organisms, Neisseria meningitidis plus M. tuberculosis, were identified as the most frequent agents of meningoencephalitis (Selim et al. 2007). In conclusion, to our knowledge, this is the first description of an IgA-MPT-64 antibody presence in CSF/TBM. The in-house test and IgG-ELISA kit, according to our analysis, show that results have to be interpreted cautiously because of the samples with borderline ratios. However, considering the difficulty in diagnosing TBM and the specificity of the tests, the tests may be useful as rapid adjuvant tests using less stringent cut-off values (ROC) while waiting for new test versions based on the adjustment of antigen composition to enhance sensitivity. ACKNOWLEDGEMENTS To Mitchell Raymond Lisbon, for English review and revision. APPENDIXES ELISA (in-house assay) - The assay was performed in polystyrene ELISA plates (Nunc Maxisorp certified, flat bottom, Denmark) separately coated with 50 µL of each antigen in 15 mM carbonate-bicarbonate buffer (pH 9.6) at a predetermined concentration of 1 µg/mL for all antigens and blocked with phosphate buffered saline with 0.01% Tween-20 (PBS-T) containing 5% bovine serum albumin (BSA). The method, design and analysis have been described previously by Kaisermann et al. (2005), with minor modifications. The plates were incubated with a 1:40 dilution of CSF as determined from previous standardised experiments. Horseradish peroxidise-linked goat anti-human immunoglobulin G (IgG) and immunoglobulin (IgA) conjugates (Pierce, Germany) were used at 1:40000 for 16 kDa and 38 kDa and 1:20000 for MPT-64 and MT10.3 antigens in PBS-T containing 1% BSA. The colour was developed by addi- tion of 50 µL of 3,3`,5,5’-tetramethylbenzidine (TMB) solution (Zymed, California, USA) and stopped with 2.5N sulphuric acid solution. In each set of experiments, positive (pooled TB) and negative (pooled control) CSF specimens were used in four serial dilutions as refer- ences. The positive and negative pools consisted of a mixture of 50 µL of 10 samples of TBM-CSF and 30 µL of 15 samples of NIND-CSF, respectively. The prepared pools were distributed in small tubes in aliquots suffi- cient for two sets of experiments. This was done to avoid degradation of the proteins due to successive thawing. Lionex TB ELISA assay - Kits were kindly provided by Lionex Diagnostics & Therapeutics GmbH, Braun- schweig, Germany (www.lionex.de). The kits were used according to the manufacturer’s instructions. Briefly, the test samples and controls (standards ready for use provided by the manufacturer) were diluted to 1:200 in the dilution solution. Then, 100 mL of the clinical speci- mens were added in respective wells of the microplates for detection of IgG, IgM and IgA. After incubation for 45 min at 37°C, the plates were washed three times with 300 μL of washing solution and then 100 μL of conjugate solution was added, except in wells corresponding to the blank. After incubation at 37°C for 30 min and wash- ing as previously described, 100 μL of TMB substrate solution was added into all wells, followed by incuba- tion at 37°C for 10 min in the dark. The reaction was stopped with 100 μL of stop solution. The reading was performed as described by Kaisermann et al. (2005). Both tests were performed without operator knowledge of the group classification of each CSF sample. Data analysis - All specimens were tested in dupli- cate. The analysis of the variation coefficient between the duplicates was < 15% on different plates and days. All CSF samples included in the NIND group may be considered as latently infected. ROC curves were con- structed with the TBM and OIM groups for each of the antigens. A cut-off point was chosen to optimize speci- ficity value; results were expressed as optical density (OD) x 1000. OD in the range of 10% above to 10% below the cut-off value was taken to identify the grey zone. For the OD values of abnormal distribution, a non-paramet- ric test with Mann-Whitney (independent samples) and Kruskal-Wallis was applied to compare group averages. Bivariate odds ratios and 95% confidence intervals were calculated for demographic and clinical characteristics associated with a positive humoral response in TBM. For most statistical analyses, SPSS for Windows, v.13.0 (SPSS Inc, Chicago, IL, USA) was adopted and MedCalc v. 11.2 (Mariakerke, Belgium) was used to calculate PPV and NPV values. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10123s2.jpg] [oc10123f2.jpg] [oc10123f1.jpg] [oc10123t2.jpg] [oc10123t1b.jpg] [oc10123t1a.jpg] [oc10123s1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}