 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 105, No. 6, 2010, pp. 838-841 SHORT COMMUNICATIONS High prevalence of drug-resistant tuberculosis and other mycobacteria among HIV-infected patients in Brazil: a systematic review Ricardo H BammannI, +; Liliana A ZamarioliII; Valdir S PintoI; Carla MP VázquezI; Marcelo N LitvocIII; Giselle B KlautauI; Fernando A Fiúza de MeloIV; Nilton J CavalcanteI; Lucilaine FerrazoliV IInstituto
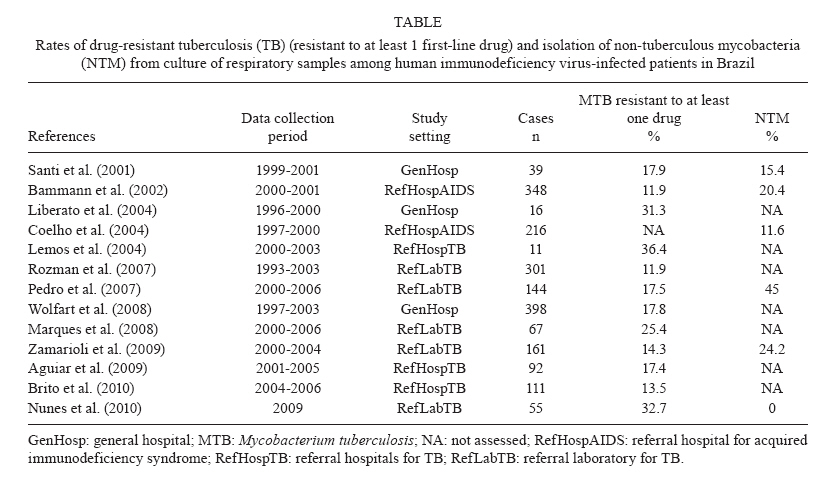
de Infectologia Emílio Ribas, São Paulo, SP, Brasil + Corresponding author: ricbammann@uol.com.br Received 27 march 2010 Code Number: oc10142 ABSTRACT There is a little-noticed trend involving human immunodeficiency virus (HIV)-infected patients suspected of having tuberculosis: the triple-treatment regimen recommended in Brazil for years has been potentially ineffective in over 30% of the cases. This proportion may be attributable to drug resistance (to at least 1 drug) and/or to infection with non-tuberculous mycobacteria. This evidence was not disclosed in official statistics, but arose from a systematic review of a few regional studies in which the diagnosis was reliably confirmed by mycobacterial culture. This paper clarifies that there has long been ample evidence for the potential benefits of a four-drug regimen for co-infected patients in Brazil and it reinforces the need for determining the species and drug susceptibility in all positive cultures from HIV-positive patients. Key words:acquired immunodeficiency syndrome - tuberculosis - drug-resistant - mycobacterial - atypical - Brazil Despite the progress made in controlling tuberculosis (TB) in Brazil, the rates of case detection and treatment success are still below the global targets (WHO 2008a). Human immunodeficiency virus (HIV)/TB co-infection carries even worse numbers, including unfavorable outcome rates above 60% (Diniz et al. 2003) and mortality rates above 25% in some settings (Jamal & Moherdaui 2007). Illness severity is the major cause of treatment failure among co-infected patients, while lack of compliance to the treatment regimen, drug resistance and non-tuberculous mycobacteria (NTM) may also play a role. Mycobacterial culturing is the gold standard among the available diagnostic methods because it has the highest sensitivity and it allows the species to be determined and the drug susceptibility to be assessed. Mycobacterial culturing (in Löwenstein-Jensen solid medium or automated, when available) is a mandatory laboratory procedure in Brazil for all clinical samples from HIV-infected patients with suspected TB (Conde et al. 2009). However, the samples are not routinely sent for culturing, while few regional facilities are equipped to perform mycobacterial culturing and drug susceptibility testing. In order to obtain reliable data on the prevalence of drug resistance and NTM among HIV-infected patients, this study has systematically compiled Brazilian studies containing culture-documented TB data. We carried out a search of the Medline, Latin-American and Caribbean Centre on Health Sciences Information (Lilacs) and Scientific Electronic Library Online (Scielo) databases (in English and Portuguese) in order to conduct a systematic review of the literature related to HIV/TB co-infection in Brazil. The free text terms used were: "AIDS and Tuberculos* and Brazil". The publication years included were from the year 2000 forward. The electronic searches were closed on 1 March 2010. The titles, abstracts and author affiliations were retrieved from the references in each database and those studies in which the diagnosis was confirmed by mycobacterial culture were selected. Based on the selected abstracts, a search was conducted of each article's full text to assess whether the methods clearly established the results for HIV-infected patients under investigation for TB, including mycobacteriological identification and drug susceptibility tests. Two additional criteria were that at least some of the patients had been recruited from the year 2000 forward and at least 70% of the samples in each study were respiratory samples. This systematic review was complemented by a manual search of the annals of Brazilian conferences held in this decade on infectious diseases (held every odd year from 2001-2009) and pulmonology (held every even year from 2000-2008), as well as of the annals of the four recent National Tuberculosis Forums (held in 2004, 2006, 2008 and the last one in May, 2010), following the same inclusion criteria. The Table presents all the selected papers and abstracts. The number of cases in each study corresponds to the number of positive cultures. Screens of Medline, Lilacs and Scielo yielded 105, 81 and 102 citations, respectively. Twenty-two different citations were considered for full-text review. Of the 22 papers reviewed in full, only eight fulfilled the stated criteria. Six papers were excluded because of the data collection period (not including patients after the year 2000), three articles were excluded because they did not clearly discriminate HIV-positive from HIV-negative results, three papers did not include respiratory samples and two thesis citations were excluded because they have not been published yet. Five additional abstracts were identified by a manual search of the annals of national conferences - two on pulmonology, two on infectious diseases and one from the last National Tuberculosis Forum. The Table summarizes all 13 selected papers and abstracts. Regarding the geographical region of data collection, most studies came from Southeastern Brazil (9), followed by the South (2), the Northeast and Central-west (1 study of each region). No studies from the North Brazil were selected. Three studies were performed in general hospitals, three in referral hospitals for TB and two in referral hospitals for AIDS. Five studies were laboratory-based. Data were collected retrospectively in all the studies but two (Liberato et al. 2004, Brito et al. 2010). Seven studies were designed to enrol both HIV-positive and HIV-negative patients. Eight papers included both pulmonary and extra-pulmonary disease. Data concerning resistance to specific anti-TB drugs among HIV-infected patients were discernible in seven of the selected studies (Santi et al. 2001, Lemos et al. 2004, Liberato et al. 2004, Rozman et al. 2007, Wolfart et al. 2008, Zamarioli et al. 2009, Nunes et al. 2010). The global resistance rate (both primary and acquired) to isoniazid alone ranged from 3.6-18.7%, while resistance to rifampicin alone ranged from 0.2-9.1%. Combined resistance to isoniazid and rifampicin ranged from 2-11%. Concerning NTM, the principal species identified were Mycobacterium avium, Mycobacterium kansasii and Mycobacterium fortuitum (Santi et al. 2001, Bammann et al. 2002, Coelho et al. 2004, Pedro et al. 2007). In Brazil, few studies have addressed the problem of drug-resistant TB. The first national survey on resistance to anti-TB drugs was performed in the middle of the 1990s. At that time, resistant TB was found in 10.6% of clinical isolates from patients who attended primary health care facilities and multidrug-resistant TB (MDR-TB) was found in 2.2% (Braga & Hijjar 2003). In response to these findings, government measures enabled the implementation of a national MDR surveillance system (Dalcolmo et al. 2007). A second national survey was begun in 2006 and preliminary data have shown primary and acquired MDR rates of 1.4% and 7.5%, respectively (Kritski 2010). The World Health Organization reports a 0.9% rate of MDR-TB among all new cases in Brazil and 5.4% among previously treated TB cases (WHO 2008b). Among 2,749 MDR-TB cases reported to the national surveillance system between 1995-2007, 7% corresponded to HIV-infected patients (Dalcolmo et al. 2007). However, for some reason, TB-drugs resistance regarding HIV-infected patients is not included in the official statistics. Clinical studies investigating HIV/TB co-infection in Brazil have also been scarce and some of them have only been published in abstract form (in the annals of conferences). The Table demonstrates that among all studies in this review, especially those from Southeastern and Southern Brazil, the proportion of drug-resistant TB samples was high, as was the rate at which NTM were isolated from co-infected patients. It is worth highlighting the fact that in the five studies (Santi et al. 2001, Bammann et al. 2002, Pedro et al. 2007, Zamarioli et al. 2009, Nunes et al. 2010) that assessed both outcomes, the proportion of cultures from HIV-infected patients positive for either Mycobacterium tuberculosis resistant to at least one drug or NTM was over 30%. Although it is difficult to draw comparisons between laboratory-based, hospital-based and population-based studies, taken together these findings are rather worrisome in diagnostic terms and they have clear therapeutic implications. Among M. tuberculosis isolates, the highest rates of drug resistance were found for isoniazid. Preliminary data from the second national survey on resistance to anti-TB drugs revealed primary and acquired resistance rates to isoniazid of 6% and 15.3% and to rifampicin of 1.5% and 8%, respectively. The MDR rates were 1.4% and 7.5%, respectively (Kritski 2010). Among HIV-infected patients, the overall average rates of resistance to isoniazid and to rifampicin varied, but they did not differ much from those of the general population. However, the rate of combined resistance reached over 9% in three settings (Lemos et al. 2004, Rozman et al. 2007, Nunes et al. 2010). In addition to reducing early bactericidal activity against replicating mycobacteria, isoniazid resistance might also inhibit rifampicin's sterilizing effect. According to Riska et al. (2000), MDR-TB reflects the progressive accumulation of individual mutations in various independent genes and not the simultaneous acquisition of resistance to multiple drugs. Resistance to one of the drugs develops first, followed by the development of resistance to another drug, eventually resulting in MDR-TB. Obviously, the entire process must occur in more than one individual patient, being completed after the transmission of strains among various infected patients, with long-term epidemiological consequences. The role of drug-resistant TB as a facilitator of the progression to MDR-TB seems to have been neglected and should be given priority. The data shown in the Table reveal high rates of combined resistance, which in Brazil are more commonly attributable to reactivation TB (Melo et al. 2003). Although there is no mention of HIV co-infection, Brazil is among the countries listed as having at least one extensively drug-resistant TB case reported (WHO 2008b). We believe that inappropriate treatment may have significantly contributed to the high mortality rate associated with HIV/TB co-infection. In addition to the well-known high rates of treatment non-compliance, other aggravating factors include delayed diagnosis and treatment together with a lack of controls over laboratory results and patients' treatment regimens. One situation that physicians often face in clinical practice is that of an HIV-infected (immunosuppressed) patient suspected of having TB. In such cases, positivity for NTM in a sputum culture, even if not confirmed by laboratory analysis according to the American Thoracic Society (ATS) (Griffith et al. 2007) criteria or any other criteria, is likely to be given considerable weight in the therapeutic decision-making process, which will probably result in the prescription of a specific treatment regimen. The diagnostic criteria adopted by the ATS emphasize the need for bacteriological identification in samples sent for culturing. In Brazil, as in other countries, the rate of suspicion of pulmonary TB based on a single sputum sample sent for laboratory analysis is quite high - over 65% of cases, even in referral centres (Zamarioli et al. 2009). Therefore, questions and criticism regarding the identification of these agents (as to whether it indicates simple colonization or disease caused by NTM) are justified and it is imperative that the clinical team be reminded of their obligation to request the additional samples required in order to confirm the diagnosis. This paper aims to draw attention to the fact that in HIV-infected patients suspected of having pulmonary TB (based on clinical and radiological manifestations or even on the presence of acid-fast bacilli in the sputum), the triple-treatment regimen recommended in Brazil for years has been ineffective in about one-third of the cases. This lack of efficacy is likely due to resistance to at least one drug or to infection with NTM. This evidence is the fruit of routinely sending samples for mycobacterial culture and it acts to reinforce policy for the National Tuberculosis Control Program (NTCP): we need sputum cultures from all HIV-positive patients in addition to all other cases of treatment failure. Dowdy et al. (2008) constructed a decision-analysis model to estimate the incremental cost-effectiveness of TB culturing from the perspective of a public-sector TB control program. They concluded that TB culturing is a potentially cost-effective tool for use among HIV-positive patients in resource-constrained settings, but integration with existing clinical systems and strengthening of post-analytical processes is required to maximize its impact. Maruza et al. (2008) suggest that TB treatment of HIV/TB co-infected patients without etiologic confirmation at the discretion of experienced physicians in referral centres did not increase the risk of unfavorable outcomes. However some variables should be closely monitored due to increased risk, for instance: the presence of other opportunistic diseases, a low CD4 lymphocyte count, a high viral load, dyspnoea, disseminated TB and changes in the TB treatment regimen due to adverse reactions or intolerance. Our results suggests that prescribing empirical treatment without laboratory confirmation of the diagnosis puts a great number of patients at risk for receiving inappropriate treatment, particularly in the context of HIV/TB co-infection. The Brazilian NTCP has recently decided to change the current triple-treatment regimen to a four-drug regimen (including rifampicin, isoniazid, pyrazinamide and ethambutol, similar to that employed in the rest of the world). It remains unclear whether this new treatment regimen will increase the rates of treatment success among patients with HIV/TB co-infections. It is also possible that there will now be a greater risk of toxicity and of interaction between the anti-TB drugs and the antiretroviral drugs. There may be some concerns regarding the recommended prophylactic use of isoniazid in HIV-infected patients. However, this increase in the spectrum of TB treatment represents a new perspective in the approach to HIV/TB co-infection in Brazil and, combined with the directly observed therapy short-course strategy, it is now essential for treating inadvertent drug-resistant TB and preventing MDR-TB. This study confirms that there has long been ample evidence of the potential benefits of such treatment for co-infected patients in Brazil. It is also important to stress the need to encourage the adoption of molecular methods for earlier detection of drug-resistant TB and of genotyping for earlier identification of the different mycobacterium species, as well as to reduce the related costs. REFERENCES
Copyright © 2010 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc10142t1.jpg] |
| |||||||||

{kind=link}