 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 1, 2011, pp. 113-116 SHORT COMMUNICATIONS Presence of maternal anti-HBs antibodies does not influence hepatitis B vaccine response in Brazilian neonates Ana Luiza N JunqueiraI; Viviane R TavaresI; Regina MB MartinsII; Kamilla V FrauzinoI; Agabo M da Costa e SilvaII; Izolina MX RodriguesIII; Ruth MinamisavaI; Sheila A TelesI, + IFaculdade
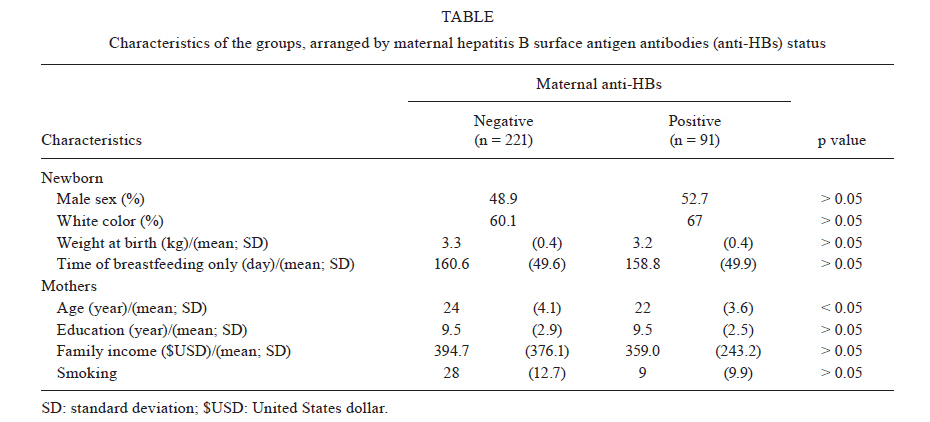
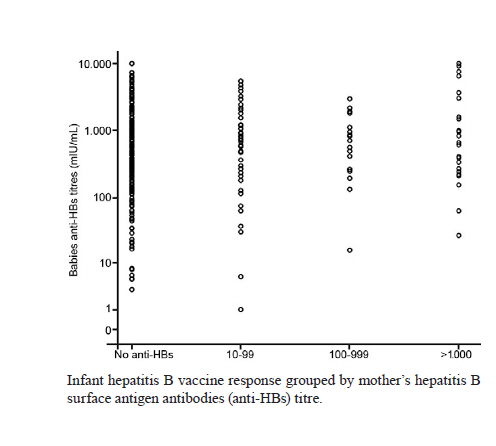
de Enfermagem Received 16 May 2010 Code Number: oc11018 ABSTRACT Recently, it was suggested that maternal hepatitis B surface antigen antibodies (anti-HBs) acquired transplacentally could play a negative role in newborn infants' immune response to the hepatitis B vaccine. We compared the hepatitis B virus (HBV) vaccine response in infants born to mothers previously vaccinated against HBV (n = 91) to infants born to mothers who were not previously vaccinated (n = 221). All newborn infants received three intramuscular doses (10 μg) of HBV vaccine (Butang®) at 0,1 and six months. The first dose was administered at the maternity hospital within 12 h of birth. The geometric mean titres of anti-HBs were not different among newborn infants born to mothers who were anti-HBs-negative (492.7 mIU/mL) and anti-HBs-positive (578.7 mIU/mL) (p = 0.38). Eight infants did not respond to the HBV vaccine. Of them, six were born to anti-HBs-negative mothers and two were born to mothers with anti-HBs titres less than 50 mlU/mL. Despite the mother's anti-HBs-positive status, our data show a good immunogenicity of the Brazilian HBV recombinant vaccine in neonates. Key words: hepatitis B vaccine - newborn infants - antibody response Vaccination is the main strategy for preventing hepatitis B virus (HBV) infection, and 171 of 193 member countries in the World Health Organization have already implemented programs for universal HBV vaccination. The estimated vaccination coverage is 69% worldwide and the American continent region has the highest proportion of vaccines (88%) (WHO 2009). Nowadays, DNA-recombinant HBV vaccine is produced by several countries. The Brazilian recombinant HBV vaccine (Butang®) is produced by Butantan Institute (IB) with genetic engineering technology that uses Hansenulla polymorpha yeast cells (Ioshimoto et al. 1999). The advantage of this yeast expression system when compared to other expression systems (such as Saccharomyces cerevisiae) is that its expression is 4-10 times higher, reducing the production costs (Hieu et al. 2002). This vaccine was introduced in the National Immunization Program in 2001 (MS 2003) and it is highly immunogenic in individuals less than 30 years of age (Baldy et al. 2004, Martins et al. 2004, Oliveira et al. 2006). Although there are no doubts about the efficacy and safety of the HBV vaccine (Zanetti et al. 2008), knowledge gaps regarding true long-term immunity and the role of passively acquired hepatitis B surface antigen antibodies (anti-HBs) on immune response in the vaccinated individuals are still matters of concern (Whittle et al. 2002, Yang et al. 2003, Boxall et al. 2004, Duval et al. 2005, Hammitt et al. 2007, Samandari et al. 2007, Alfaleh et al. 2008, Hu et al. 2008, Van Herck & Van Damme 2008, Boot et al. 2009). Recently, Hu et al. (2008) suggested that maternal anti-HBs acquired transplacentally play a negative role in newborn infants' immune response to the HBV vaccine. Because long-term persistence of anti-HBs protector titres have been related to higher anti-HBs titre peaks after a full vaccine scheme (Whittle et al. 2002, Duval et al. 2005, Hammitt et al. 2007), it should be of great interest to assess whether maternal anti-HBs interfere with the active immune response to HBV vaccine in neonates. Thus, in this study, we compared the neonatal immune response to Butang® in infants born to mothers previously vaccinated against HBV to infants born to mothers who were not previously vaccinated. This investigation followed 459 women and their newborn infants at four maternity hospitals located at the eastern region of the city of Goiânia, Goiás (GO): Maternity and Hospital East Goiânia (n = 129), Nossa Senhora de Lourdes Maternity (n = 138), Vila Nova Hospital and Maternity (n = 102) and São Lucas Hospital (n = 90) in Goiânia, between March-November 2007. In these maternity hospitals, a total of 681 newborn infants were born to mothers who lived in the study region (n = 182, n = 190, n = 166 and n = 143, respectively). To be included in the investigation, the mother must have tested negative for HBV surface antigen (HBsAg) and human immunodeficiency virus (according to a pregnancy screening) and must have been aged < 30 years. Newborn infants were required to have an Apgar score > 8, a weight > 2.5 kg and no evidence of congenital disease. All newborn infants received three intramuscular doses (10 μg) of HBV vaccine (Butang®, IB, Brazil, lots 0511197/A and 0510182/B) at 0,1 and six months of age. This vaccine has proven to be highly immunogenic and safe (Baldy et al. 2004, Martins et al. 2004, Isolani et al. 2006, Oliveira et al. 2006). The first dose was administered at the maternity hospital within 12 h of birth. The second and third doses were administered in the subjects' households. About 45 days after the third vaccine dose, blood samples (3 mL) were collected and anti-HBs titres were determined by automatic analysis using the immuno-enzymatic microparticles method (MEIA) (AxSYM® Ausab®, Abbott, Germany). Samples with anti-HBs titres greater than 1,000 mIU/mL were diluted 1:10 and retested by MEIA. The immunoprotection criterion was defined as an anti-HBs concentration greater than or equal to 10 mIU/mL. Blood samples from the mother were collected upon study enrolment. In order to exclude those mothers who presented total HBV core antigen antibodies (anti-HBc) due to a previous HBV infection, all samples were tested for total anti-HBc antibodies by enzyme-linked immunosorbent assay (Hepanostika anti-HBc, Uni-Form). Samples that tested negative for total anti-HBc underwent quantitative analysis for anti-HBs as described above. The Student t test or the Kruskal-Walis test was used to compare continuous variables and the Chi-square test or the Fisher's exact test was used to compare categorical variables. Statistical significance was assessed at the 0.05 probability level in all analyses. The geometric mean of anti-HBs titres was calculated with a 95% confidence interval. Statistical evaluations were performed using SPSS version 11.0 (SPSS Inc, Chicago, US, 1999). Participation in the study was voluntary. The newborn infants' mothers signed an authorization form that had been approved by the Human and Animal Research Ethical Committee of the Maternity and Children's Hospital, Goiânia. Of the 459 mother-baby pairs, four pairs were excluded because the mothers were anti-HBc-positive and 143 pairs did not complete the full investigation. The characteristics of non-participant pairs (n = 147) were similar to participant pairs (n = 312) (p > 0.05). Of the 312 participating mothers, 221 (70.8%) tested negative for anti-HBs, 49 (15.7%) had anti-HBs titres between 10-99 mIU/mL, 18 (5.8%) between 100-999 mIU/mL and 24 (7.7%) greater than or equal to 1,000 mIU/mL. The geometric mean titres (GMT) of anti-HBs was 173.2 mIU/mL. Table shows the characteristics of the groups studied, arranged by maternal anti-HBs status. Sex, race, weight at birth, time of breastfeeding, mother's education level, family income and mother's smoking status did not differ between infants born to anti-HBs-positive mothers and infants born to anti-HBs-negative mothers (p > 0.05). The mean of age of anti-HBs-positive mothers was lower than anti-HBs-negative mothers (p < 0.01). Among the 312 infants, 304 (97.4%) responded to the HBV vaccine. Of those, 30 (9.6%) had anti-HBs titres between 10-99 mIU/mL, 168 (53.8%) between 100-999 mIU/mL and 106 (34%) greater than or equal to 1,000 mIU/mL. The GMT of the anti-HBs titres was 519.1 mIU/mL. Infants born to mothers whose anti-HBs titres were greater than or equal to 10-99 mIU/mL had a GMT of 534.4 mIU/mL (range: 1.0-5,421). This was similar to that found in newborn infants with mothers having anti-HBs titres between 100-999 mIU/mL (GMT = 511.8 mIU/mL; range: 14.6-2,938), in newborn infants with mothers having anti-HBs titres greater than or equal to 1,000 mIU/mL (GMT = 746.5 mIU/mL; range: 24.9-10,002) and even in newborn infants born to mothers who were anti-HBs-negative (492.7 mIU/mL; range: 3-10,000) (p > 0.05) (Figure). Among those newborn infants who did not respond to the HBV vaccine (n = 8), six were born to mothers testing anti-HBs-negative and two were born to mothers whose anti-HBs titres were low (19.2 mIU/mL and 49.2 mlU/mL). Similar to other studies (Martins et al. 2004, Isolani et al. 2006, Luna et al. 2009), we found that almost all (97.4%) infants developed protector anti-HBs titres following three Butang® doses, emphasizing the good immunogenicity of the Brazilian HBV vaccine in newborns. Regarding immunoprophylaxis against vertical HBV transmission, some authors have reported lower anti-HBs titres in newborn infants receiving HBV immunoglobulin plus HBV vaccine at birth than in newborn infants receiving the HBV vaccine only (Pongpipat et al. 1989, Yang et al. 2003). More recently, Hu et al. (2008) have suggested that high maternal anti-HBs titres due to previous immunization could also interfere with the active immune response to HBV vaccine in newborn infants. However, in contrast to these reports, we did not find any association between the level of maternal anti-HBs and HBV vaccine response in the neonates studied. Rather, newborn infants whose mothers had anti-HBs titres > 1,000 mIU/mL presented the highest GMT of anti-HBs. Also, among the eight infants who did not respond to the HBV vaccine, the mothers of six were anti-HBs-negative and the mothers of the other two had anti-HBs titres less than 50 mIU/mL. In our investigation, which is consistent with the findings of Hu et al. (2008), all the newborn infants were healthy and the vaccines were not injected in the dorsogluteal region, which has been associated with low vaccine response (CDC 1985). However it is worthy of note that the concentration of recombinant HBsAg administered to our newborn infants was twice the amount that was used by Hu et al. (2008) (10 μg vs. 5 μg). Thus, we could speculate that this higher antigen concentration was sufficient to compensate the binding of maternal anti-HBs to Butang® vaccine HBsAg, adequately challenging the babies' immune systems and consequently eliciting high anti-HBs titres. This investigation has limitations, though. Blood samples were not collected from infants after the first and second vaccine dose for anti-HBs testing and the kinetic of anti-HBs following the vaccine doses was not investigated between groups. Also, we studied 312 mother-baby pairs, but the number of participants may have been insufficient to detect differences between groups (type II statistical error). This is the first investigation to compare the immunogenicity of Butang® in newborn infants born to mothers vaccinated or not vaccinated against HBV, confirming the Brazilian HBV vaccine's efficacy of immunogenicity in neonates despite the mother's HBV vaccine status. However, with the increasing number of women vaccinated against HBV worldwide (WHO 2008) and the possible role of anti-HBs titre peak on long-term persistence of anti-HBs protector titres (Samandari et al. 2007, Bialek et al. 2008, Lu et al. 2008), further studies will be needed to evaluate the immune response to different vaccine schemes, including different concentrations of recombinant HBsAg. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11018f1.jpg] [oc11018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}