 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 2, 2011, pp. 207-211 ARTICLE Leishmania infection in humans, dogs and sandflies in a visceral leishmaniasis endemic area in Maranhão, Brazil Ilana Mirian Almeida FelipeI, +; Dorlene Maria Cardoso de AquinoI; Oliver KuppingerI; Max Diego Cruz SantosI; Maurício Eduardo Salgado RangelI; David Soeiro BarbosaII; Aldina BarralIII; Guilherme Loureiro WerneckII; Arlene de Jesus Mendes CaldasI IUniversidade
Federal do Maranhão, Rua Viana Vaz 230, 62020-660 São Luís,
MA, Brasil + Corresponding author: ilanamirian@hotmail.com Received 4 September
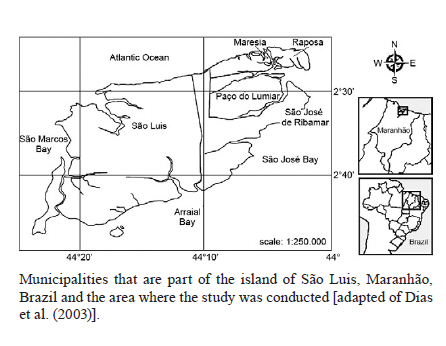
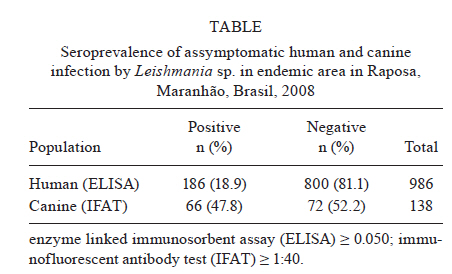
2010 Code Number: oc11034 ABSTRACT Leishmania infection in humans, dogs and sandflies was examined in the endemic visceral leishmaniasis (VL) municipality of Raposa, state of Maranhão, Brazil. In this study, we examined Leishmania chagasi infection in the blood serum of both humans and Canis familiaris and the natural Leishmania sp. infection rate in the sandfly vector, Lutzomyia longipalpis. Enzyme-linked immunosorbent assay, indirect immunofluorescence reaction and polymerase chain reaction were performed to detect Leishmania infections in humans, dogs and sandflies, respectively. Overall, 186 out of 986 studied human beings were infected with L. chagasi parasites, representing an infection prevalence of 18.9%. An even higher infection rate was detected in dogs, where 66 (47.8%) out of 138 were infected. Among all Lu. longipalpis captured (n = 1,881), only 26.7% were females. The Leishmania infection frequency for the vector Lu. longipalpis was 1.56%. Remarkably, all infected sandflies were found in the peridomiciliary area. Furthermore, a high incidence of asymptomatic forms of VL in the human and canine populations was observed. The results of this study suggest autochthonous transmission of L. chagasi in this endemic area for visceral leishmaniasis because infection by Leishmania sp. was identified in all important elements of the transmission chain. Key words: serum prevalence - Lutzomyia longipalpis - visceral leishmaniasis - Maranhão - Brazil Visceral leishmaniasis (VL) is considered an important neglected disease that affects many countries of the world (Desjeux 2004). On the American continent, VL is caused by the protozoan parasite Leishmania chagasi, which is transmitted to humans and other vertebrate hosts (e.g., dogs) through the bite of a female sandfly. Lutzomyia longipalpis is considered to be the main vector for VL in Brazil (Lainson & Rangel 2005). A high proportion of L. chagasi infected persons do not present any clinical symptoms of disease, even after a long incubation period (asymptomatic form) (Evans et al. 1992, Romero et al. 2009). Cohort studies in Brazil have described detection of asymptomatic seroconvertors with a sensitive and specific enzyme linked immunosorbent assay (ELISA) test using crude antigens from promastigotes (Badaró et al. 1986a, c). Extensive surveillance over decades has demonstrated the detection of antileishmania antibodies without clinical symptoms, and this has been well accepted as indicative of asymptomatic infection. Epidemiological studies in VL endemic areas have shown that a percentage of individuals with no history of clinical manifestations show evidence of infection with L. chagasi, as demonstrated by the detection of antileishmania antibodies and/or positivity to the Montenegro skin test. About 20% of these individuals may develop clinical manifestations and the others will remain asymptomatic or progress to the oligosymptomatic form of the disease (Badaró et al. 1986a, b, Evans et al. 1992, Marzochi et al. 1994, Caldas et al. 2001). Malnutrition is considered one of the most important factors associated with the development of clinical symptoms of leishmaniasis (Alvar et al. 2006). The high frequency of Leishmania infection found in human beings, dogs and Lu. longipalpis in previous studies in the municipality of Raposa, state of Maranhão (MA), Brazil, may also be associated with poverty (Caldas et al. 2001, 2002). Notably, the current knowledge on the epidemiology of VL is mainly based on studies examining the prevalence of Leishmania infections only among humans. There are few studies that simultaneously examine L. chagasi infection across several known hosts and carriers. Therefore, the aim of the present study was to determine the asymptomatic L. chagasi infection rates in human beings, dogs and the vector Lu. longipalpis in the VL endemic area of Raposa. PATIENTS, MATERIALS AND METHODS The study was performed from August 2006-July 2008 in Vila Maresia, Vila Marisol and Vila Pantoja; all three neighbourhoods are located in the municipality of Raposa situated in the northern coastal region of MA, approximately 28 km from the state capital, São Luis (Figure). In this study, the inclusion criteria for human subjects were the following: living in an endemic area for more than six months, no signs and symptoms of VL (fever for more than 2 weeks, hepatosplenomegaly, weight loss or mucocutaneous pallor) and no previous history of VL. As exclusion criteria, we considered a history of treatment for VL (including treatment failures and relapses), individuals with known immunodeficiency or currently using immunosuppressants and comorbidities (evidence of other conditions leading to splenomegaly, such as schistosomiasis and malaria). In a preliminary census survey, we found 1,417 inhabitants, 986 (70%) of whom participated in the study. This 30% loss was mainly due to internal and external migrations, as well as refusal to participate in the study. Overall, 986 (69.6%) out of 1,417 inhabitants that lived more than six months in the area and did not exhibit clinical VL symptoms participated in the study. From these, 857 individuals (86.9%) were from Vila Maresia, 77 individuals (7.7%) were from Vila Marisol and 52 individuals (5.3%) were from Vila Pantoja. All participants signed an informed consent form and supplied their identification card number, social-economic and epidemiological data. A physical examination was performed to identify common symptoms of the VL or signs suggesting the oligosymptomatic subclinical infection. Blood samples from humans and dogs were collected for the subsequent ELISA and indirect immunofluorescence reaction (IFR) analyses, respectively. ELISA analysis for the presence of Leishmania antibodies was performed at the Laboratory of Immunopathology of the Gonçalo Muniz Research Center of Oswaldo Cruz Foundation (Fiocruz), Bahia (BA), Brazil (Caldas et al. 2001) and was considered to be positive when the absorbance level exceeded 0.050. In the canine census survey, we found a population of 220 pet dogs; among these dogs, 138 (63%) fulfilled the following inclusion criteria: no clinical signs suggestive of VL were present at the time of the survey. Owners who allowed their dogs to participate signed an authorisation form, after which we obtained identification data for the animals, performed physical examinations and collected blood samples for serological tests. Among the 138 dogs selected for the study, 126 animals (87%) originated from Vila Maresia, seven (5%) from Vila Marisol and five (4%) from Vila Pantoja. To detect L. chagasi infection in dogs, an IFR was utilised according to the Biomanguinhos-Fiocruz kit protocol (MS 2006). Infection was considered positive when titer was > 1:40. The study was approved by the Research Ethics Committee of the University Hospital of the Federal University of Maranhão (protocol 249/2006). L. chagasi infected dogs were sacrificed according to protocols established by the Brazilian Ministry of Health (MS 2006) at the Zoonoses Control Center in São Luis. Sandflies were captured with luminous traps of the type Centre for Disease Control from May 2007-May 2008, once per month from 6:00 pm-6:00 am in 12 micro-areas (Sudia & Chamberlain 1998). Two residences per micro-area were randomly chosen and intradomicile and periodomicile traps were set monthly, totalling 48 traps during each year. Lutzomyia species were identified according to Young and Ducan (1994). Leishmania infected females were identified after preparation of DNA crude extracts of Lu. longipalpis individuals according to Mukhopadhyay et al. (2000). Pools with DNA from eight specimens were prepared and submitted to polymerase chain reaction (PCR) amplification of a mini kinetoplast Leishmania DNA target sequence performed according to the protocol of Volpini et al. (2004). The only modification of the PCR conditions was a prolonged extension time from 10-30 s in all PCR cycles. We used the forward primer (5'GGG(G/T)AGGGGCGTTCT(G/C)CGAA3') and the reverse primer (5'(G/C)(G/C)(G/C)(A/T)CTAT(A/T)TTACCAACCCC3') (Miranda 1998). DNA of L. chagasi (MHOM/BR/BA262) was used as a positive control and sterile water was used as a negative control. The amplified PCR products were analysed by separating them on a 1.5% agarose gel. In case of Leishmania infection in any of the pools, PCR analyses were performed for each individual sample of that pool. The frequencies of Leishmania infected humans and dogs were analysed using Epi Info software version 6.04d (CDC, Atlanta, EUA) and Stata 9.0. The prevalence of human and canine Leishmania infection was calculated by dividing the number of serum positive individuals by the total number of humans and dogs, respectively, multiplied by 100. The formula for calculating the natural infection rate of Lu. longipalpis by Leishmania sp. was the following: natural infection rate = number of positive infected females x 100/total number of examined insects. RESULTS Individual blood samples from 986 persons were examined by ELISA for L. chagasi infections in Vila Maresia, Vila Marisol and Vila Pantoja. From these, 186 persons were found to be infected by the parasite, representing a L. chagasi infection rate of 18.9% in the examined population (Table). The examination of 138 individual dog blood samples by IFR detected L. chagasi infections in 66 animals, indicating an infection rate of 47.8%. Among the 1,932 trapped phlebotomines, 554 (27%) were females. Taxonomic analysis of these sandflies identified six distinct species: Lu. longipalpis, Lutzomyia evandroi, Lutzomyia flaviscutellata, Lutzomyia lenti, Lutzomyia sordelli and Lutzomyia wellcomei. The majority of the trapped sandflies, 1,368 (97.02%) of all collected flies, belonged to the species Lu. longipalpis. Among the collected Lu. longipalpis, 505 (26.7%) were females. More sandflies (74.5%) were captured in the peridomestic areas than in the intradomicile areas. Furthermore, a higher frequency of sandflies was found during the months of May 2007 (12.12%) and February 2008 (40.19%) in the rainy season vs. the dry season months of October 2007 (6.91%) and December 2007 (5.58%). Five of the 56 Lu. longipalpis pools (each pool consisted of 8 Lu. longipalpis females, representing 448 females in total) analysed by PCR amplified a specific 120 bp mini kinetoplast DNA Leishmania target region, indicating Leishmania sp. infection. Additional PCR analysis of the 40 individual Lu. longipalpis females from the five infected pools detected Leishmania sp. infection in seven females. Thus, a natural Leishmania infection frequency of 1.56% was determined. DISCUSSION A higher L. chagasi infection frequency among humans was established in this study (18.9%) when compared to a previous study in the same municipality (13.5%) (Caldas et al. 2001). The rates of infection among humans were much higher than those observed in other surveys in the North and Northeast Regions of Brazil, such as in the states of Ceará (prevalence of 4.5%) and Pará (3.4%), but similar to those recorded in the states of Piauí (13.9%) and BA (16.1%). The rates in this study were also higher than what was previously seen in a different area of the state of MA (17.5%) (Badaró et al. 1986a, Evans et al. 1992, Werneck et al. 2002, Nascimento et al. 2005, Rosas Filho & Silveira 2007). Such differences might reflect not only variations in the magnitude of transmission between these areas but also differences in the diagnostic methods used and the age distribution within the studied population. Ryan et al. (2006), while studying two villages in Kenya, found a linear relationship between seroprevalence for VL and age. Because our study included all age groups this feature could be an explanation for the high prevalence reported here. Other studies reported similar L. chagasi infection frequencies in regions with both high and low VL endemicities (Barão et al. 2007, Romero et al. 2009). Compared to the L. chagasi infection rate in human beings, a relatively high L. chagasi infection frequency of 47.8% was found in dogs. The L. chagasi infection rate in dogs was approximately twice that found in another endemic area of MA where 25% of dogs were found to be infected with L. chagasi (Guimarães et al. 2005). However, a study performed in an endemic area in São Luis demonstrated an even higher frequency (67%) (Barbosa et al. 2010). Yet another study examining L. chagasi infection in dogs in the Northeast Region of Brazil found a lower infection rate than this current study (37.8%) (Amóra et al. 2006). Different Leishmania infection frequencies for humans and dogs are expected due to the different diagnostic methods employed, temporal variability and discrepancies between the dynamics of transmission between the canine and human population. Variations in the transmission dynamics might possibly be explained by distinct local susceptibility profiles of human and dog, the possibility of different vertebrates serving as Leishmania reservoir and distinct demographic socio-environmental conditions of the community (Werneck 2008). Lu. longipalpis accounted for more than 97% of all sandflies captured and was by far the most predominant sandfly species in the investigated peridomicile and intradomicile areas. This vector has also been found to be the principal Lutzomyia species in other endemic areas (Araújo et al. 2000, Ximenes et al. 2000, Michalsky et al. 2009). Lu. longipalpis has been reported to adapt easily to the anthropic environment and has been shown to be important for VL epidemiology (Rangel & Vilela 2008). Higher numbers of Lu. longipalpis were found during the rainy season compared to the dry season, but we could find sandflies throughout the whole year, suggesting that Leishmania parasites can be transmitted in this region during the entire year. In recent years, PCR-based diagnostic methods have been described for leishmaniasis, with a wide range of sensitivities and speciûcities. An excellent target for a sensitive and rapid detection method is the kinetoplast mini-circle DNA, which is present at thousands of copies per cell (Salotra et al. 2001). The natural infection rate of Lu. longipalpis by Leishmania sp. in our study was 1.56%, which is high when compared to another study (Silva et al. 2007). This might be explained by the methodology used in our work and also the higher levels of deforestation and degraded living conditions in our studied area. Notably, all infected sandflies were found in the peridomicile areas where we could observe a large number of animals, mainly chickens and dogs (Moreira et al. 2003, Rotureau 2006). The relatively high L. chagasi infection rate found simultaneously in human, dog and Lu. longipalpis populations is an important aspect for understanding the L. chagasi transmission cycle in the study area. This result implies that the municipality of Raposa exhibits a favourable environment for L. chagasi transmission, which predominantly occurs in the peri-urban areas. These areas in Raposa are characterised by the destruction of the natural environment by human invasion and deforestation (Caldas et al. 2002). This favours Lu. longipalpis adaptation to peri-urban areas. The absence of sylvatic animals in the destructed area may result in altered blood feeding behaviour encouraging blood sucking on domestic animals (e.g., dog) and human beings. Therefore, the high Leishmania infection rate of human beings, dogs and vectors reveals favourable conditions for the maintenance of the L. chagasi transmission chain and the occurrence of the disease in Raposa. Interestingly, a high prevalence of VL was found between the years 2004-2006 in Raposa. The VL prevalence rate varied during the described period from 130-306 cases per 100,000 inhabitants (Silva et al. 2008). An important limitation of this study is that both ELISA for diagnosis of asymptomatic infection in humans and genus specific PCR assay for detecting infection in sandflies may not be the most valid techniques to employ. Consequently, prevalence estimates of infection by L. chagasi might not be accurate (Aransay et al. 2000, Romero et al. 2009). However, we were less concerned in providing exact prevalence estimates than with showing autochthonous transmission in the area by identifying L. chagasi infection in all important elements of the transmission chain. Although the approach used might not guarantee that all detected infections are caused by the species L. chagasi, epidemiological support is given to our conclusions both by the fact that cases of VL were reported in that region and that infections were detected in the known VL host, vector and reservoir populations. The possibility of serological cross-reaction with other Leishmania or Trypanosoma cruzi is not likely because there are no records of Chagas disease or cutaneous leishmaniasis in that area. Findings such as those described in this study indicate the necessity of performing more studies to examine Leishmania infection rate simultaneously in human, dog and Lu. longipalpis populations to shed light on particularities of Leishmania transmission dynamics and thus uncover more features of VL epidemiology. Control measures implemented by health authorities should consider the complexities involved in the transmission dynamics of Leishmania infection in local areas. Incorporation of novel technologies, such as geographic information systems, for monitoring the spread of disease, environmental and health education policies and a better integration between the community and local health providers are necessary to assure quality of health care to VL patients and to minimise L. chagasi transmission rates in Raposa. ACKNOWLEDGEMENTS To Prof. Dr Ana Lúcia Abreu Silva and Prof. Dr José Ma-nuel Macário Rebêlo, for field research support, and to Jorge Luís Pinto Moraes, for sandfly collection. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11034f1.jpg] [oc11034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}