 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 3, 2011, pp. 316-321 ARTICLES Human rhinovirus in the lower respiratory tract infections of young children and the possible involvement of a secondary respiratory viral agent Nayhanne Tizzo de PaulaI; Bruno Moreira CarneiroI; Jonny YokosawaI, +; Guilherme Ramos Oliveira e FreitasI; Thelma Fátima de Mattos OliveiraI; Lourenço Faria CostaI; Hélio Lopes da SilveiraI, II; Divina Aparecida Oliveira QueirózI ILaboratório
de Virologia, Instituto de Ciências Biomédicas, Universidade Federal
de Uberlândia, Av. Pará 1720 Bl. 4C, 38400-902 Uberlândia,
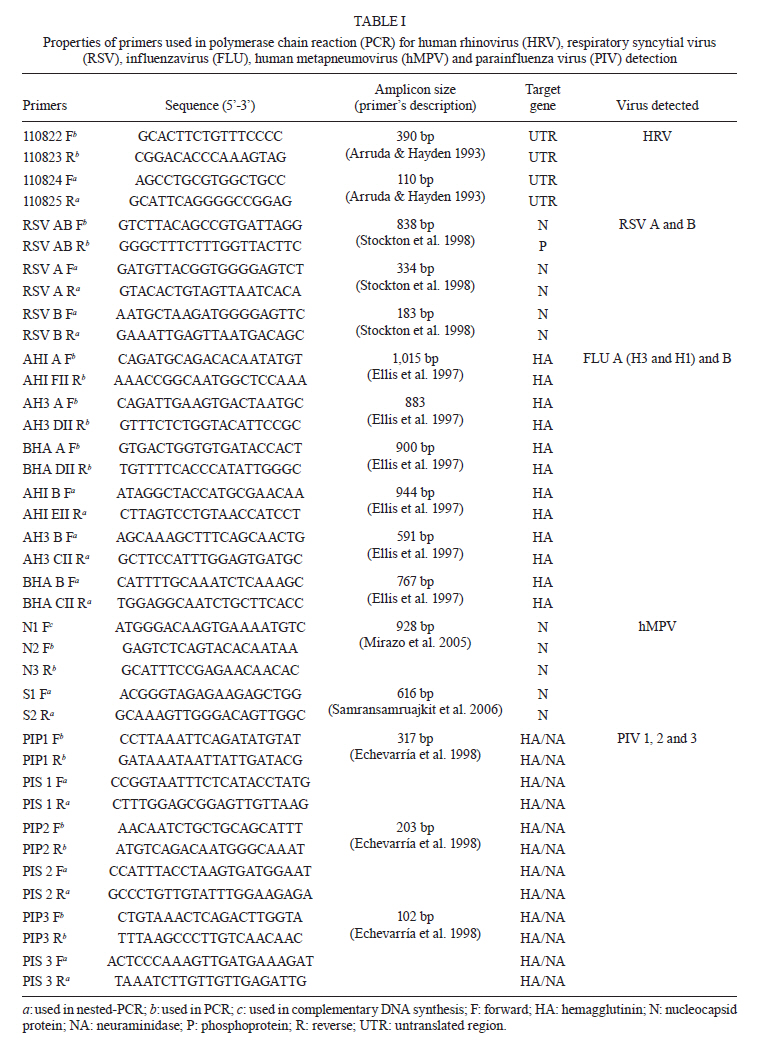
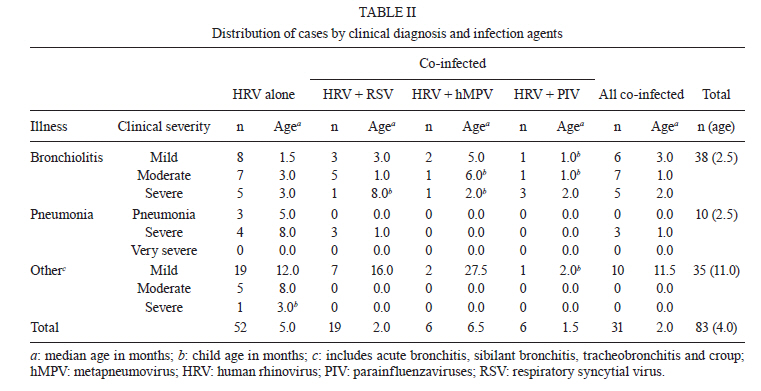
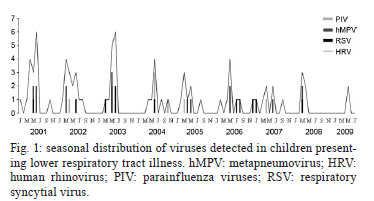
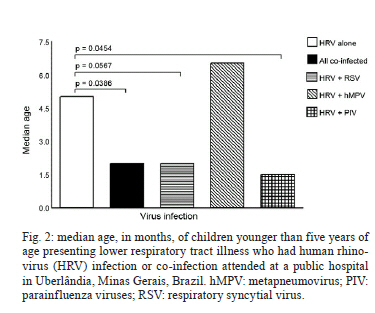
MG, Brasil + Corresponding author: jyokosawa@icbim.ufu.br Financial support: CAPES, CNPq, Fapemig Received 5 October 2010 Code Number: oc11052 ABSTRACT Human rhinoviruses (HRV) are usually associated with mild respiratory symptoms in children. However, some studies have found that HRV can cause severe disease, especially when the patient is co-infected with a second virus. In this study, 532 nasopharyngeal aspirates (NPAs) were collected over a nine-year period from children at the Clinics Hospital of Uberlândia. The collected NPAs were then tested for HRV RNA using the reverse transcription-polymerase chain reaction. Eighty-three specimens from children diagnosed with lower respiratory tract illness (LRTI) were positive for HRV RNA and were then tested for the presence of eight other respiratory viruses. A second virus was detected in 37.3% (31/83) of the samples. The most frequent clinical diagnosis was bronchiolitis, followed by other LRTI and then pneumonia. The frequency of severe disease in children infected with more than one virus was not significantly different from the frequency of severe disease in children infected with HRV alone. Children infected with both HRV and parainfluenza virus (1.5 m.o.) were significantly younger than those infected by HRV alone (5.0 m.o.) (p = 0.0454). Overall, these results suggest that infection with a second virus does not lead to a higher frequency of severe syndromes in children presenting with LRTI. Key words: human rhinoviruses - co-infection - lower respiratory tract - young children Human rhinovirus (HRV) is typically associated with mild upper respiratory tract infections and exacerbation of asthma in children (Gern & Busse 1999, Manoha et al. 2007, Mackay 2008, Kelly & Busse 2008). HRV is a member of the Picornaviridae family and is composed of a non-enveloped particle with a positive-sense single-stranded RNA genome. The genome consists of 11 genes that are translated as a single polyprotein, which is divided into three regions (P1, P2 and P3) that are subsequently cleaved into four mature structural (VP4, VP2, VP3 and VP1) and seven non-structural proteins (2A, 2B, 2C, 3A, 3B, 3CPRO and 3DPOL) (Kirchberger et al. 2007, Kistler et al. 2007, Mackay 2008). Three HRV species have been described: A, B and C (Lau et al. 2007, Palmenberg et al. 2009). Previously, diagnosis of HRV was difficult because culture of the virus was limited (Cheuk et al. 2007, Paranhos-Baccalà et al. 2008). Due to advances in nucleic acid amplification, we can now detect HRV and determine when HRV is the causative agent of lower respiratory tract illness (LRTI) (Choi et al. 2006, Miller et al. 2007, Gerna et al. 2009, Louie et al. 2009). HRV is frequently detected in children diagnosed with bronchiolitis and pneumonia (Manoha et al. 2007, Miller et al. 2007, Louie et al. 2009). Additionally, HRV can cause severe complications in patients that are immunocompromised (Malcolm et al. 2001) or have underlying chronic disorders (Kim & Hodinka 1998, Glezen et al. 2000, Cheuk et al. 2007, Dreschers et al. 2007). Identification of HRV co-infection with other respiratory viruses, such as respiratory syncytial virus (RSV) (Papadopoulos et al. 2002, Miller et al. 2007, Paranhos-Baccalà et al. 2008, Marguet et al. 2009), is possible because of advances in the molecular detection of HRV (Aberle et al. 2005, Jacques et al. 2006, Calvo et al. 2008). Scientists have questioned whether or not HRV co-infections lead to more severe clinical syndromes, cause longer hospitalisations and affect younger children more frequently (Drews et al. 1997, Papadopoulos et al. 2002, Calvo et al. 2007, 2008, Richard et al. 2008, Gerna et al. 2009, Midulla et al. 2010). The objective of this study was to identify cases of HRV co-infection in nasopharyngeal aspirates (NPAs) from children presenting with LRTI and to determine if there is an association between viral co-infection and the clinical severity of bronchiolitis, pneumonia and LRTI. PATIENTS, MATERIALS AND METHODS Patients and clinical specimens - From 2000-2009, a total of 552 NPAs were collected from children presenting with symptoms of acute respiratory disease (ARD) at the Clinics Hospital of Uberlândia, Federal University of Uberlândia (HCU-UFU) in the state of Minas Gerais, Brazil. Patients included in the study were less than five years of age and were admitted to the hospital within five days of the onset of ARD symptoms. The HCU-UFU is a public university hospital that provides health care to students and low-income individuals living in Uberlândia, as well as 120 other cities and towns in the region, covering an estimated population of two million people. This study was approved by UFU's ethics committee according to registration 387/08. Informed consent was obtained from each child's parent. As part of the surveillance for respiratory viruses, samples are routinely screened using an indirect immunofluorescence assay that can detect seven common res-piratory viruses [respiratory syncytial virus, influenzaviruses (FLU) A and B and parainfluenza viruses (PIV) 1, 2, 3 and adenovirus]. Detection of HRV - Samples that were negative or inconclusive in the initial screening (321 samples) were screened for HRV RNA using the reverse transcription-polymerase chain reaction (RT-PCR). RNA was extracted with Trizol® (Invitrogen Corp, Carlsbad, CA) according to the manufacturer's instructions. Complementary DNA (cDNA) was synthesised using the SuperScript® III Reverse Transcriptase mix and an HRV-specific primer according to the manufacturer's protocol. Briefly, 5 µL of total RNA was mixed with 2 pmol of primer 1 (5'-GCACTTCTGTTTCCCC-3') and 10 mM of dNTP mix and incubated at 65ºC for 5 min. Then, 4 µL of buffer 5x FS, 0.1M DTT, 200 units of Superscript III and 20 µL of water was added to the mix, which was then heated at 55ºC for 1 h. Following cDNA synthesis, the enzyme was heat inactivated at 70ºC for 10 min. Amplification of the HRV nucleotide sequence was performed as previously described by Costa et al. (2006). For the first-round of PCR, the cDNA template was amplified with primers 1 and 2 (5'-CGGACACCCAAAGTAG-3'). The amplification conditions used were as follows: 95ºC for 1 min, 40 cycles of 94ºC for 1 min, 48ºC for 1 min and 72ºC for 1 min and a final step of 72ºC for 5 min. One microlitre of the first-round PCR product was used as the template for the second-round PCR with primers 3 (5'-AGCCTGCGTGGCTGCC-3') and 4 (5'-GCATTCAGGGGCCGGAG-3'). The second-round PCR amplification conditions were the same as the first-round except that 30 cycles were run instead of 40. Co-infection testing - Clinical specimens that were positive for HRV RNA and were collected from patients who presented with a clinical diagnosis of LRTI were selected for additional screening for eight respiratory viruses. Briefly, RSV A and B and FLU A and B were detected using multiplex two-step PCR reactions with previously described primers and conditions (Stockton et al. 1998). Human metapneumovirus (hMPV) was detected using a protocol that was previously described by our group (Carneiro et al. 2009). Finally, PIV 1-3 were detected using the primers and conditions published by Echevarría et al. (1998). Primer sequences, expected fragment lengths and viral primer targets are listed in Table I. Due to the limited specimen volume, samples in which a second virus was detected were not tested for the presence of an unlikely triple infection. RSV A and B and FLU A and B (Stockton et al. 1998) were the first viruses tested for, followed by hMPV (Carneiro et al. 2009) and PIV 1-3 (Echevarría et al. 1998). This order was chosen according to clinical relevance of co-infections in children as determined by the literature (Aberle et al. 2005, Calvo et al. 2008, Cilla et al. 2008, Richard et al. 2008) and because of the circulation rate of the most common viruses in the region (Costa et al. 2006). Clinical criteria - Clinical syndromes were characterised as bronchiolitis, pneumonia or other LRTI (acute bronchitis, sibilant bronchitis, tracheobronchitis and croup). A responsible physician performed classification of clinical severity at the time of sample collection. Bronchiolitis was characterised as mild, moderate or severe according to the parameters defined by the "clinical score of respiratory failure in bronchiolitis" adapted by De Boeck et al. (1997). Pneumonia was classified as pneumonia, severe pneumonia or very severe pneumonia according to criteria defined by the World Health Organization (WHO 2005). Clinical scores adapted by Taussig et al. (1975) were used to classify the other LRTI syndrome clinical scores. Statistical analysis - The data were analysed using Graphpad Prism 4.0 (GraphPad Software Inc San Diego, CA, USA). The evaluation of the median ages of different groups was performed using the Mann-Whitney U test and Fisher's exact test was used to analyse the difference between clinical manifestations in children with either a single or dual viral infection. RESULTS Eighty-three patients diagnosed with LRTI had specimens that were positive by RT-PCR for HRV RNA. Co-infection with a second virus was found in 37.3% (31/83) (Table II) of the 83 specimens. RSV was detected as the second virus in 23% (19/83) of the specimens, followed by hMPV and PIV, which were both detected in 7% (6/83) of the specimens, and three cases each of PIV-1 and 2 were detected. FLU A and B and PIV-3 were not detected in these samples. Regarding seasonality, Fig. 1 shows that from 2000-2009, HRV, RSV, hMPV and PIV co-circulate and that outbreaks occurred primarily between February-June (mid-summer to late autumn) with the highest incidence in April and May. Bronchiolitis was the most common clinical manifestation, accounting for 45.8% (38/83) of cases, followed by LRTI (acute bronchitis, sibilant bronchitis, tracheobronchitis and croup) in 42.2% (35/83) of cases and pneumonia in 12% (10/83) of cases. An analysis of the severe cases of bronchiolitis, pneumonia and LRTI revealed no statistical differences in the frequency between single infection (HRV alone) and dual infection (p > 0.05). Also, no difference was observed between patients infected with a single virus who presented with moderate to severe illness compared to those with dual infection (p > 0.05) (Table II). The median age of children with dual virus infection was two months, which was significantly different from the mean age of children infected with HRV alone (5.0 m.o.) (p = 0.0386). The median age of children co-infected with HRV and PIV (1.5 m.o.) was significantly lower than the median age of children infected with HRV only (p = 0.0454). Additionally, younger children (2.0 m.o.) seemed to be more prone to co-infection with HRV and RSV than to suffer from a single HRV infection (p = 0.0568) (Fig. 2). DISCUSSION In this study, the rate of HRV co-infection with other respiratory viruses was found to be similar to rates in other countries (Calvo et al. 2007, Cilla et al. 2008). The high frequency of HRV co-infection with RSV has been observed previously (Papadopoulos et al. 2002, Paranhos-Baccalà et al. 2008, Richard et al. 2008, Gerna et al. 2009). In our region, the high prevalence of HRV and RSV co-infection may be related to seasonal trends (Costa et al. 2006, Oliveira et al. 2008); HRV and RSV infections peak concurrently. Previous reports suggested that co-infection with viral respiratory diseases may result in a more severe clinical manifestation than infection with only one virus (Aberle et al. 2005, Cilla et al. 2008, van der Zalm et al. 2009). Richard et al. (2008) suggested that dual infection is a risk factor for more severe illness, which is independent of the host's condition. Moreover, HRV-RSV co-infections have been associated with a higher likelihood of presenting with severe clinical syndromes than infection with HRV alone (Aberle et al. 2005). However, our results show that LRTI associated with viral co-infection does not result in a higher incidence of severe syndromes compared to infection with HRV alone. Other groups have reported similar results (Williams et al. 2004, Choi et al. 2006, Calvo et al. 2007, Louie et al. 2009). In contrast to previous reports (Calvo et al. 2007, 2008, Cheuk et al. 2007, Bonzel et al. 2008), we observed that HRV-PIV co-infection (median of 1.5 m.o.) was more common in younger children. According to van der Zalm (2009), younger children may be more prone to co-infection because they have a less developed immune system. In conclusion, our results indicate that HRV co-infection with a second respiratory virus is not responsible for more severe LRTI in young children. ACKNOWLEDGEMENTS To the laboratories of Immunology, Parasitology, Molecular Biology, Physiology and Genetics, UFU, for allowing us to use their facilities and the health care professionals of the Clinics Hospital of Uberlândia for the screening of patients. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11052f1.jpg] [oc11052f2.jpg] [oc11052t1.jpg] [oc11052t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}