 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 3, 2011, pp. 339-345 ARTICLES Epidemiology of fungal infections in liver transplant recipients: a six-year study of a large Brazilian liver transplantation centre Michelle ZickerI, +; Arnaldo Lopes ColomboI; Ben-Hur Ferraz-NetoII; Luis Fernando Aranha CamargoI, II IUniversidade
Federal de São Paulo, Rua Botucatu 740, 04023-900 São Paulo, SP,
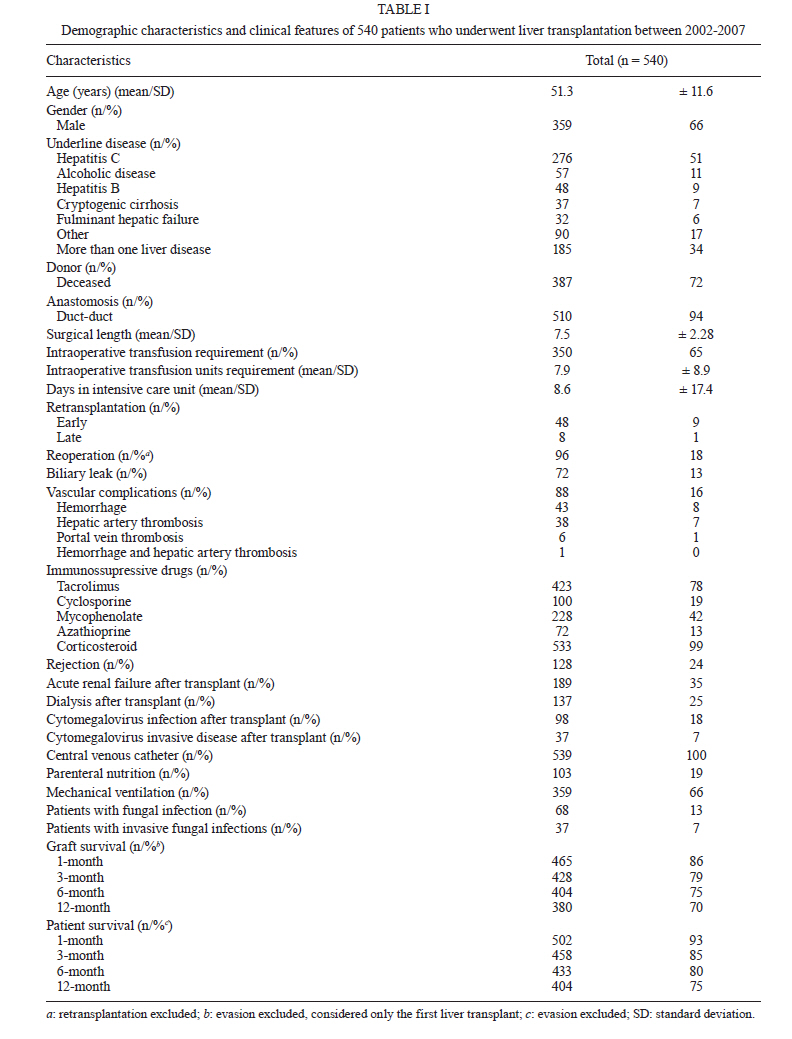
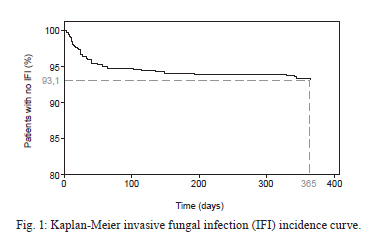
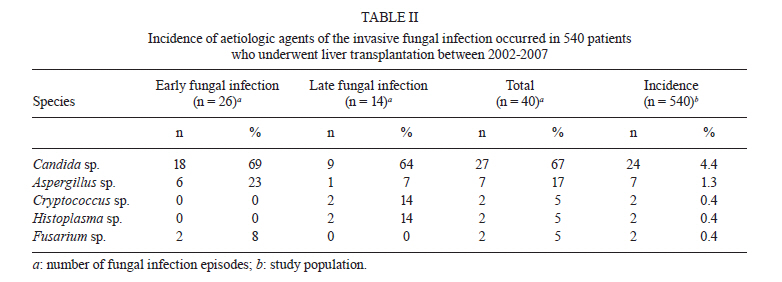
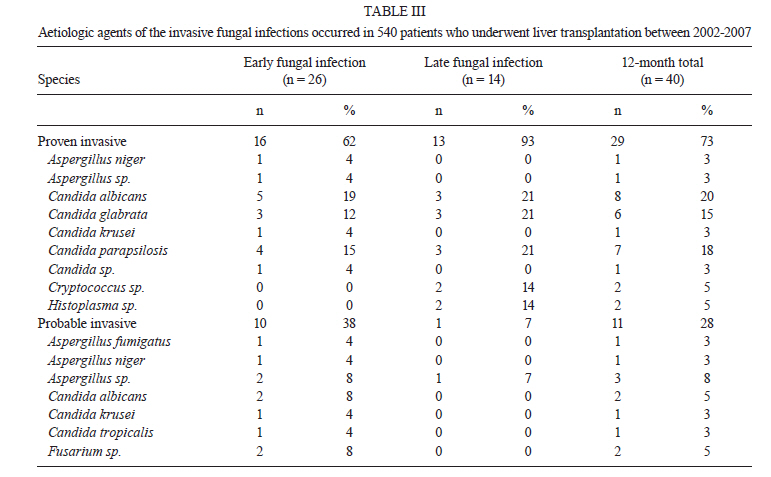
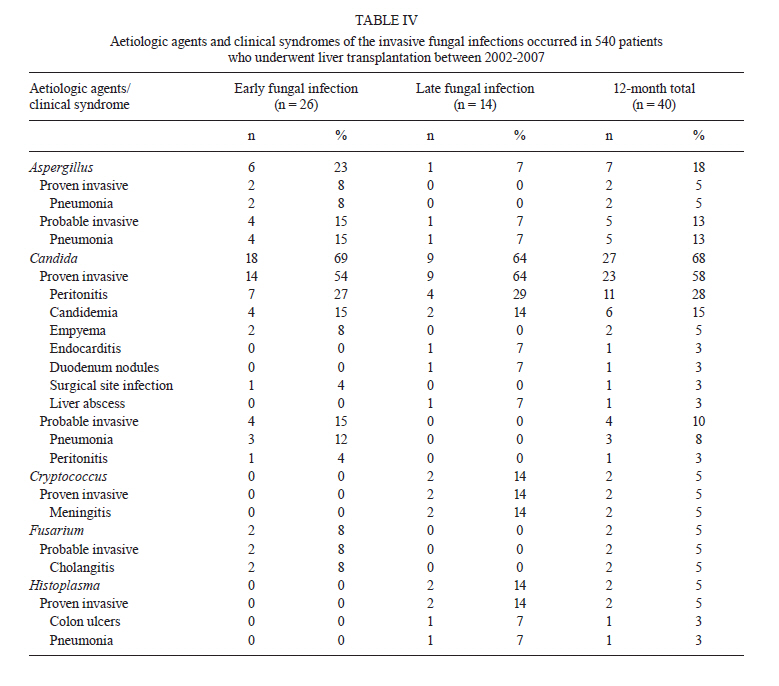
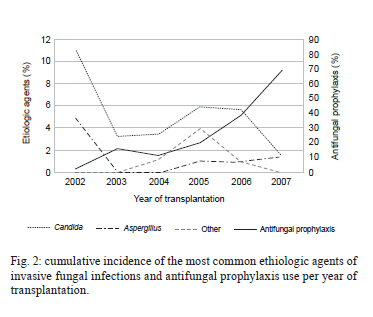
Brasil + Corresponding author: zickerm@yahoo.com.br Received 13 November 2010 Code Number: oc11056 ABSTRACT Liver transplant seems to be an effective option to prolong survival in patients with end-stage liver disease, although it still can be followed by serious complications. Invasive fungal infections (ifi) are related to high rates of morbidity and mortality. The epidemiology of fungal infections in Brazilian liver transplant recipients is unknown. The aim of this observational and retrospective study was to determine the incidence and epidemiology of fungal infections in all patients who underwent liver transplantation at Albert Einstein Israeli Hospital between 2002-2007. A total of 596 liver transplants were performed in 540 patients. Overall, 77 fungal infections occurred in 68 (13%) patients. Among the 77 fungal infections, there were 40 IFI that occurred in 37 patients (7%). Candida and Aspergillus species were the most common etiologic agents. Candida species accounted for 82% of all fungal infections and for 67% of all IFI, while Aspergillus species accounted for 9% of all fungal infections and for 17% of all IFI. Non-albicans Candida species were the predominant Candida isolates. Invasive aspergillosis tended to occur earlier in the post-transplant period. These findings can contribute to improve antifungal prophylaxis and therapy practices in Brazilian centres. Key words: liver transplantation - mycoses - epidemiology Liver transplant appears to be an effective option in prolonging survival and improving the quality of life in patients with end-stage liver disease. Data from The Brazilian Society of Solid Organ Transplant shows that 1,322 liver transplants were performed in Brazil in 2009 (ABTO 2009). Although liver transplant is performed worldwide, it can be accompanied by serious and fatal complications such as infections, which are the most frequent cause of death during the post-transplant period. Invasive fungal infections (IFI) are associated with high rates of morbidity and mortality, in part due to immunosuppression, but also because of the delay in diagnosis as a result of the nonspecific symptoms and poor specificity of currently used laboratory tests (Fung 2002). The incidence of fungal infections after liver transplant ranges from 4-50% and Candida spp and Aspergillus spp are the most common aetiological agents. Other fungal species such as Cryptococcus neoformans, the non-Aspergillus filamentous species and the endemic mycosis agents such as histoplasmosis, coccidioidomycosis and blastomycosis have variable incidences, depending on the geographic origin of the patient (Singh 2000, Fung 2002, Cruciani et al. 2006, Playford et al. 2006). In two recent multicentre studies, the incidence of invasive candidiasis ranged from 68-78.7%, while the incidence of invasive aspergillosis and cryptococcosis varied from 7.9-11% and from 6-7.1%, respectively (Neofytos et al. 2010, Pappas et al. 2010). The epidemiology of fungal infections in Brazilian liver transplant recipients remains unknown. Obtaining this information may contribute to improvements in antifungal prophylaxis and therapy practices. The aim of this study was to determine the incidence and epidemiology of fungal infections in patients who underwent liver transplant in a large Brazilian liver transplantation centre over a six-year period. PATIENTS, MATERIALS AND METHODS This is an observational and retrospective study. The epidemiological and clinical data were collected from medical registries of all liver transplant recipients > 18 years of age who underwent liver transplantation at Albert Einstein Israeli Hospital between January 2002-December 2007. Albert Einstein Israeli Hospital is a private, tertiary, 489-bed hospital. Almost 700 liver transplants have been performed in this hospital since 2002, when the Solid Organ Transplantation Program was established. All fungal infection episodes occurring within one year of liver transplantation were described regarding the aetiological agent and infection site. Fungal infection was considered "early" if occurred < 90 days after transplantation or "late" if occurred > 90 days after transplantation. Fungal infections were also categorised as shown below: Proven IFI - Was defined as one of the following: at least one positive blood culture for Candida spp or other pathogenic fungi, a positive culture for a pathogenic fungus from a specimen collected from a normally sterile site, a positive culture for a pathogenic fungus from a biopsy specimen (taken across a potentially colonised mucosal surface) plus histopathology confirming fungal elements in tissue with local inflammation, evidence of fungal endophthalmitis based on dilated fundoscopic examination, positive histopathology for fungal elements in a deep tissue biopsy, positive cryptococcal or histoplasma antigen test and clinical or radiographic evidence consistent with cryptococcosis or histoplasmosis, a positive culture or histopathologic evidence of an endemic mycosis (blastomycosis, histoplasmosis or coccidioidomycosis), positive culture for a mould (Aspergillus spp, Fusarium spp, zygomycete) from a non-sterile body site together with clinical, histopathologic or radiologic evidence consistent with IFI, or evidence of fungal elements in a post mortem tissue evaluation (Singhal et al. 2000, Pappas et al. 2006). Probable IFI - Was defined as clinical illness consistent with IFI in the absence of other causes of sepsis, together with positive fungal cultures from one or more non-sterile sites and supporting radiographic or other diagnostic methodologies but without histopathologic confirmation of the disease (Pappas et al. 2006). Superficial fungal infection - Was defined as clinical signs and symptoms of infection and evidence of fungal elements on a non-sterile mucosal surface (oropharyngeal, oesophageal, gastrointestinal, genital) (Pappas et al. 2006). Oropharyngeal candidiasis diagnosis was based on clinical findings and oesophageal infection was diagnosed by the presence of consistent findings in an upper gastrointestinal endoscopic exam. Lower urinary tract infections due to the presence of Candida species were excluded because most cases of candiduria represent colonisation rather than infection and the distinction between colonisation and true infection is loose. Species identification was performed using the API kit (bioMérieux, Marcy I'Etoile, France) or the CHROmagarTM system. Cytomegalovirus (CMV) infection was defined by the presence of a positive CMV pp65 antigenemia result (> 1 cell/105 white blood cells) or a positive CMV polymerase chain reaction result (> 10 copies/106 white blood cells) after transplantation. Data analyses were performed in PASW Statistics 18 (SPSS, Chicago, IL, USA). Mean and standard deviation or median and range were used for continuous variables, while categorical variables were summarised with counts and percentages. Graft survival analysis was performed based on the first liver transplantation and excluding patients that were lost during follow-up within one year of transplant. Cumulative incidences per year of the most commonly encountered pathogens were calculated. IFI incidence within one year of transplantation was estimated using the Kaplan-Meier method. For patients who underwent multiple transplant procedures, the date of first transplantation was used to calculate time to infection. The three-month and 12-month mortality rates after an IFI episode were also calculated. RESULTS Patients - A total of 596 liver transplants were performed in 540 patients. Sixty-six percent of the patients were male and the mean age was 51.3 years. Hepatitis C was the underlying liver disease in 276 (51%) patients. Tacrolimus and corticosteroid were the most frequent primary immunosuppressive drugs administered. Overall, 68 (13%) patients developed at least one fungal infection episode and 37 (7%) had at least one episode of IFI. The 12-month patient and graft survival rates were 70% and 75%, respectively. Demographic data and clinical features are summarised in Table I. Fungal infections - Seventy-seven fungal infections occurred in 68 (13%) patients. IFI accounted for 52% of (40 from 77 episodes) all fungal infections and tended to occur early (< 90 days) in the post-transplant period, as shown in Fig. 1. Invasive candidiasis was the most common fungal infection during both the early and late post-transplant periods and was described in 4.4% of the liver recipients. Candida species accounted for 82% (63 from 77 episodes) of all fungal infections and for 67% (27 from 40 episodes) of all IFI. Non-albicans Candida isolates were more likely to occur than Candida albicans. Aspergillus species accounted for 9% (7 from 77 episodes) of all fungal infections and for 17% (7 from 40 episodes) of all IFI. The incidence of aspergillosis in the study population was 1.3%. Invasive aspergillosis tended to occur during the early post-transplant period. Cryptococcosis, histoplasmosis and fusariosis accounted for 5% each of all IFI (Tables II, III). Most fungal infections that were considered "early" had a median time of onset of 13 days (range 1-78 days). IFI accounted for 44% (26 from 59 episodes) of all early fungal infections. Among early IFI (proven and probable), pneumonia due to Aspergillus spp and peritonitis due to Candida spp were the most common clinical syndromes reported. Late fungal infections had a median time onset of 135 days (range 102-365 days). Most late infections (78%) were classified as invasive infections and peritonitis due to Candida spp was the most frequent diagnosis (Table IV). Among the early superficial fungal infections, there were 32 infections due to Candida species (25 episodes of oral candidiasis, 4 of esophagitis, 2 of vaginitis and 1 of gastric candidiasis) and one episode of lower urinary tract infection due to Trichosporon pullulans. During the late post-transplant period, there were only four episodes of Candida esophagitis. Overall, 300 (55.5%) patients used antifungal agents as empiric or microbiologically documented therapy. Only 138 (25.5%) patients received antifungal prophylaxis. Fluconazole at 50 mg daily was administered to 88 patients (mean time: 11.4 days ± 6.0). Forty patients received fluconazole at 200 mg per day (mean time: 15.1 days ± 9.9) and seven patients received fluconazole at 100 mg daily (mean time: 10 days ± 5.9). Conventional amphotericin B was administered to only three patients at different doses: 10 mg, 25 mg and 40 mg (mean time: 10 days ± 4.6). Fig. 2 shows the cumulative incidence per year of the most commonly encountered pathogens. It is worth noting that the incidence of invasive candidiasis has decreased since 2005, while antifungal prophylaxis use has increased since that time. No considerable change in the Aspergillus incidence has been observed. The three-month and 12-month survival rates after IFI was 67.5% and 54%, respectively. DISCUSSION The incidence of fungal infections in liver transplantation varies by the presence of risk factors and depends on the studied period of time. Recently many centres have reported a lower incidence of fungal infections, even in the absence of antifungal prophylaxis. The evolution of immunosuppressive drug regimens and improvement in surgical techniques may explain this trend (Singh 2000). In the present study, IFI was described in 7% of liver recipients, which reflects a population with few risk factors. Similar incidences were previously described in low risk patients, while higher rates are found in patients with many risk factors (Patel et al. 1996, Rabkin et al. 2000, Fung 2002, Husain et al. 2003). In addition to a decreased need in intraoperative transfusion and shorter post-transplantation Intensive Care Unit (ICU) stay, a low proportion of patients underwent choledochojejunostomy or had CMV infection. Singh et al. (2002) reported a correlation between the incidence of fungal infection and evolution of transplantation practices. Most IFI episodes were due to Candida species and non-albicans Candida isolates were more likely to be present than C. albicans. Aspergillus spp and Cryptococcus spp ranked second and third after Candida. The reported incidence of candidiasis in liver transplantation ranged from 35-91%, while the incidence of Aspergillus and Cryptococcus ranged from 9-45% and from 3-7%, respectively (Singh 2000, Salavert 2008). The wide range in the incidence rates of candidiasis in previously reported studies can be explained by differences in the classification of fungal infections as invasive or superficial with regards to non-sterile mucosal infection and lower urinary tract. Candida infections are generally derived from endogenous flora. Conditions that predispose a patient to Candida colonisation are frequent in liver transplant recipients and can lead to overgrowth in the hepatobiliary, gastro-intestinal and genitourinary tracts and facilitate fungaemia and dissemination. The frequency of non-albicans Candida isolates has increased. Proposed explanations include: widespread use of fluconazol in the pre and post-transplant period, prolonged pre-transplant hospitalisation, nosocomial acquisition and use of broad-spectrum antibiotics (Anonymous 2004). In this study, 38.5% of patients received empiric fluconazole, 67.6% received broad-spectrum antibiotics and 10% stayed in the ICU before transplant. Six out of seven episodes of invasive aspergillosis occurred in the early post-transplant period. Environmental factors (the hospital was under construction for expansion), the improvement of diagnostic tests, earlier clinical suspicion and the fact that higher risk patients have undergone transplant after the implementation of model for end-stage liver disease (MELD) in Brazil as a criterion in prioritising patients in the waiting list can explain this finding. The incidence of invasive aspergillosis compared to the incidence of cryptococcosis in liver transplant recipients is different from the incidences found in kidney transplant recipients. The incidence of aspergillosis in kidney transplant recipients is lower (0-26%) than the incidence of cryptococcosis (0-39%). The opposite has been seen in liver transplantation (Singh 2000). The main risk factor related to the development of cryptococcosis after solid organ transplantation is the immunosuppressive regimen, particularly the use of corticosteroid drugs (Vilchez et al. 2002, 2003). In contrast to kidney recipients, most liver recipients are no longer receiving corticosteroid drugs during the late post-transplant period, a time when higher incidences of cryptococcosis have been observed. However, during the pre-transplant period, liver recipients are under a greater risk of acquiring invasive aspergillosis due to their greatly immunosuppressed body. The higher survival rate of kidney recipients compared to liver recipients is another possible explanation for the differences in incidence rates between cryptococcosis and aspergillosis (Pappas et al. 2010). Patients tended not to receive antifungal prophylaxis. A decrease in fungal infections due to Candida, particularly those classified as "superficial," has been observed since 2005. No relevant change has occurred in the Aspergillus incidence. This finding is consistent with an increase in the use of antifungal prophylaxis targeting the Candida species during the same period. The present study shows three-month and 12-month survival rates after IFI of 67.5% and 54%, respectively. Mortality rates after an invasive fungal episode ranged from 50-92% in previous reports (Neofytos et al. 2010). Recently, Pappas et al. (2010) observed a 12-month survival of 59% in a surveillance study performed in solid organ transplant recipients. In a similar study, Neofytos et al. (2010) reported a three-month survival of 70% in a mixed population of organ recipients, but lower rates were observed in liver recipients, probably as result of the acuity of systemic illness and the patients' underlying compromised status. The inclusion of oral and oesophageal candidiasis as superficial infections based on clinical findings and without a positive culture is a limitation of this study. However, as this is a retrospective study based on medical records and little data are available about the epidemiology of fungal infections in Brazilian liver transplant recipients, we decided to retain this information in our analysis. Another limitation is the occurrence of two reported cases of biliary tract fusariosis. Patients presented with fever, no response to antibiotics and a positive biliary fluid culture for Fusarium. Although both patients had recovered after institution of antifungal therapy, the possibility of colonisation could not be completely excluded. In summary, this paper showed significant data regarding the epidemiology of fungal infection in Brazilian liver transplant recipients. These data can contribute in the improvement of antifungal prophylaxis and therapy practices. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11056t1.jpg] [oc11056t2.jpg] [oc11056f1.jpg] [oc11056t4.jpg] [oc11056t3.jpg] [oc11056f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}