 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 3, 2011, pp. 378-380 SHORT COMMUNICATIONS A rapid detection of multidrug-resistant Mycobacterium tuberculosis by a nitrate reductase assay on blood agar Ahmet Yilmaz CobanI, +; Yeliz Tanriverdi CayciI; Aydin DeveciII; Alper AkgunesIII; Meltem UzunIV; Belma DurupinarI IDepartment
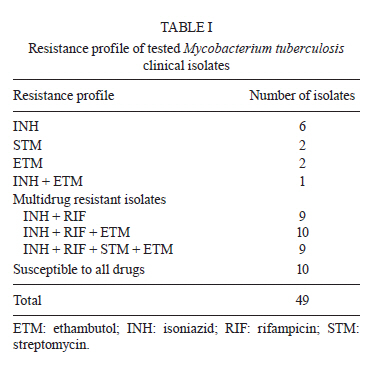
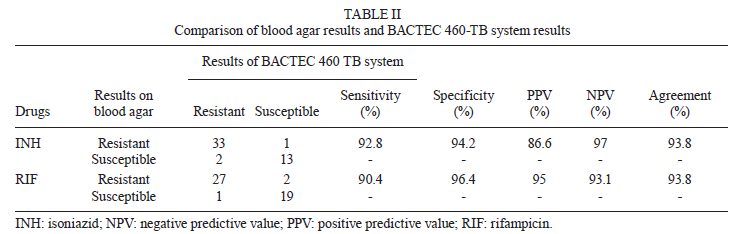
of Medical Microbiology, Medical School, Ondokuz Mayis University, Samsun, Turkey Received 19 November 2010 + Corresponding author: cobanay2003@yahoo.com.tr Code Number: oc11064 ABSTRACT The susceptibility of 49 Mycobacterium tuberculosis clinical isolates to isoniazid (INH) and rifampisin (RIF) (28 multi-drug resistant-tuberculosis samples) was determined by a nitrate reductase assay (NRA) on blood agar. Agreement between the NRA and other testing methods was found to be 93.8% for both INH and RIF. The sensitivity, specificity, positive predictive value and negative predictive value for INH were 92.8%, 94.2%, 86.6% and 97%, respectively. The sensitivity, specificity, positive predictive value and negative predictive value for RIF were 90.4%, 96.4%, 95% and 93.1%. In conclusion, we show here that blood agar can be used effectively for the NRA test. Key words: Mycobacterium tuberculosis - nitrate reductase assay - blood agar Tuberculosis remains an important public health problem and has recently been increasing in incidence (Affolabi et al. 2007). The early detection of antimicrobial susceptibility is especially important for creating an appropriate treatment protocol for patients with tuberculosis. Multi-drug resistant (MDR) tuberculosis isolates present a major challenge for tuberculosis control programs (Shikama et al. 2009). Therefore, microbial susceptibility to at least isoniazid (INH) and rifampisin (RIF) should be ascertained to diagnose MDR tuberculosis. Conventional methods [proportion methods in Löwenstein-Jensen (LJ) and Middlebrook 7H10 agar] for tuberculosis drug susceptibility testing have many disadvantages, including being labour intensive and time consuming. Although several rapid automated testing systems (Bactec 460-TB, Bactec MGIT 960, ESP Culture System II) are available, they cannot be used effectively in developing countries due to their cost (CLSI/NCCLS 2003, Shikama et al. 2009). Developing alternative methods to conventional and rapid automated systems is of great importance. The resazurin microplate method (REMA), microscopic observation drug susceptibility, nitrate reductase assay (NRA), MTT test and broth microdilution method are a few examples of these alternative methods (Palomino et al. 2002, Coban et al. 2004a, b, Mengatto et al. 2006). The NRA test is typically performed on LJ medium; this presents several disadvantages, including the required cooking preparation and potential interactions between antibiotics and phospholipids in the medium (Kent & Kubica 1985). We aimed to investigate INH and RIF susceptibility for determining MDR tuberculosis using an NRA test on blood agar, a method which has recently been developed to test the antibiotic susceptibility of tuberculosis bacilli (Coban et al. 2006). Forty-nine Mycobacterium tuberculosis clinical isolates, including 28 MDR isolates and the reference strains H37Rv (susceptible to all drugs), ATCC 35822 (INH resistant) and ATCC 35820 (streptomycin resistant), were tested in this study. Antibacterial resistance patterns of the clinical isolates are summarised in Table I. Drug susceptibility testing of all isolates was determined by Bactec 460 TB, which is considered the benchmark automated system and is commonly used in diagnostic laboratories. INH and RIF powders were obtained from Sigma-Aldrich, Germany. Stock solutions were prepared according to the manufacturer's instructions and stored at -80ºC. Blood agar-based medium (bioMérieux, SA, Marcy I'Etoile France) was prepared according to the manufacturer's recommendations with some modifications. Five millilitres of glycerol per litre of medium and potassium nitrate (1000 µg/mL) were added to the medium, which was then sterilised using an autoclave. After being cooled to 45ºC, the medium was supplemented with 5% defibrinated sheep blood. Media with antibiotics were prepared from stock antibiotic solutions. Antibiotic concentrations identified by CLSI/NCCLS (2003) for Middlebrook 7H10 agar were used in the blood agar. Five millilitres of medium with final concentrations of 0.2 µg/mL INH and 1 µg/mL RIF was prepared in screw-cap glass tubes and kept in an oblique position to solidify. Three drug-free control media were prepared for each isolate. Two or three colonies freshly grown on LJ medium were dispensed and vortexed for 30 s in screw-cap tubes containing 3 mL of phosphate buffer and 8-10 glass beads. The tubes were then kept in a vertical position for 30 min at room temperature to sediment large particles and aerosols. The supernatant was then transferred to another tube and adjusted to McFarland 1 standard; in addition, bacterial suspension was then diluted 1:10 with phosphate buffer from the bacterial suspension and adjusted to McFarland 1 standard (Angeby et al. 2002). Two hundred microlitres of bacterial suspension adjusted to McFarland 1 standard was inoculated into a screw-cap tube containing blood agar with antibiotic. An equal volume of the 1:10 dilution was inoculated into three screw-cap tubes containing drug-free blood agar. All tubes were incubated at 37ºC. Five hundred microlitres of freshly prepared Griess reagent (1 part 50% hydrochloric acid, 2 parts 0.2% sulphanilamide and 2 parts 0.1% n-1-naphthyl-ethylenediamine dihydrochloride) was added to the drug-free tubes on the seventh day of incubation. The Griess reagent was added to tubes containing antibiotics when a colour change was observed. Results were reported according to colour changes; if a colour change was not observed, the incubation period was extended to the 10th and 14th days (Angeby et al. 2002). Results were obtained on the seventh day for 44 isolates and on the 10th day for five isolates. One false INH-resistant isolate and two false INH-susceptible isolates were found by NRA, as determined by Bactec 460 TB. False RIF resistance and susceptibility by NRA comparing with Bactec 460 TB were determined in two isolates and one isolate, respectively. Agreement was found to be 93.8% for both INH and RIF. The sensitivity, specificity, positive predictive value and negative predictive value for INH were found to be 92.8%, 94.2%, 86.6% and 97%, respectively. The sensitivity, specificity, positive predictive value and negative predictive value for RIF were 90.4%, 96.4%, 95% and 93.1% (Table II), respectively. The NRA method has been directly or indirectly compared with other reference methods, including the Bactec 460 TB, Bactec MGIT 960, REMA test and proportion method in LJ medium, for determining antibiotic susceptibility in tuberculosis (Sanchotene et al. 2008, Ani et al. 2009, Rosales et al. 2009, Shikama et al. 2009, Visalakshi et al. 2010b). Forty-nine M. tuberculosis clinical isolates were indirectly tested by NRA in this study. The specificities of the NRA test for INH and RIF were found to be 94.2% and 96.4% and the sensitivities were found to be 92.8% and 90.4%, respectively. NRA results agreement was found to be 93.8% for both drugs. Results were available between days seven-14, with the majority being available by the 10th day. In this study, results were obtained on the seventh day for 44 isolates and on the 10th day for five isolates. NRA is used to determine secondary drug susceptibility in addition to its use for determining the susceptibility of M. tuberculosis clinical isolates to primary anti-tuberculosis drugs. The sensitivity of NRA for kanamycin, ethionamid, ofloxacin, cycloserine and para-aminosalicylic acid susceptibility has been reported to be 86.4-100% and NRA specificity has been found to be 98.4-100% (Visalakshi et al. 2010a). Martin et al. (2005) have shown complete agreement between the results of the NRA and the reference method for determining ofloxacin susceptibility. They also performed an NRA test in Middlebrook 7H11 instead of in LJ medium. Devasia et al. (2009) have reported that NRA tests were sensitive and specific in determining the fluoroquinolone resistance of M. tuberculosis clinical isolates. It has also been shown that an adapted NRA test could be used to determine primary anti-tuberculosis drug susceptibility (Syre et al. 2003, 2006). Affolabi et al. (2008) have evaluated NRA using a liquid medium in assaying the susceptibility of 144 clinical isolates to INH and RIF. They found the test sensitivity to be 100% for both drugs and the specificity for INH and RIF to be 99.2% and 99.3%, respectively. It has been also demonstrated that NRA is a reliable method for determining the minimal inhibitory concentration of INH, RIF and ethambutol (Kumar et al. 2005). Blood agar has been shown to be useful in testing the drug susceptibility of tuberculosis. This study shows that it can also be used to perform an NRA test. The critical concentration (1 µg/mL) recommended for drug susceptibility testing on Middlebrook 7H10 for RIF was used instead of the critical concentration (40 µg/mL) recommended for testing on LJ medium. Unlike LJ medium, blood agar does not require cooking for solidification and does not have a risk of antibiotic interactions with any of its contents. This is in marked contrast to LJ, in which phospholipids can interact with antibiotics. In conclusion, we have shown that blood agar can be used to perform NRA tests, which are useful in drug susceptibility testing for determining MDR tuberculosis in developed and developing countries. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11064t2.jpg] [oc11064t1.jpg] |
| |||||||||

{kind=link}
{kind=link}