 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 3, 2011, pp. 390-393 SHORT COMMUNICATIONS Monitoring the circulation of rotavirus among children after the introduction of the RotarixTM vaccine in Goiânia, Brazil Ana Maria Tavares Borges+; Menira Dias e Souza; Fabíola Souza Fiaccadori; Divina das Dores de Paula Cardoso Instituto de Patologia
Tropical e Saúde Pública, Universidade Federal de Goiás,
Goiânia, GO, Brasil Financial support: CNPq Received 17 September
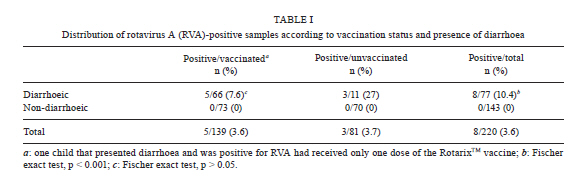
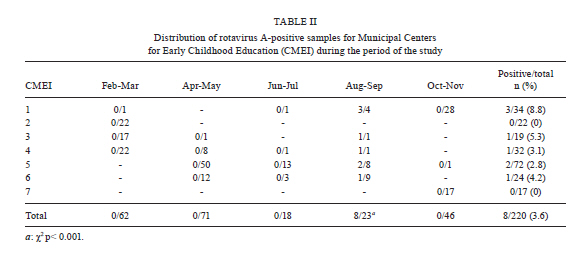
2010 Code Number: oc11084 Abstract The epidemiological features of rotavirus A (RVA) infection differ between children from developing and developed countries which could result in differences in vaccine efficacy around the world. To evaluate the impact of RotarixTM on RVA prevalence, we monitored RVA genotypes circulating in Goiânia by monitoring virus in faecal samples from children that had or had not been previously vaccinated. From February-November of 2008, 220 faecal samples were collected from children in seven day-care centres. RVA detection was performed by two methodologies and the results were confirmed by polyacrylamide gel electrophoresis. From the 220 samples, eight were RVA-positive (3.6%) and five were from children that had received either one or two doses of the vaccine. All positive samples were collected from children with diarrhoea during August and September. Genotyping of the RVA characterised five of the viral samples as genotype G2P[4] and one as G8P[4], suggesting that G2P[4] was the predominant circulating genotype in Goiânia during the study. The fact that vaccinated children were also infected by RVA suggests that the vaccine does not fully protect against infection by the G2[P4] RVA genotype. Key words: rotavirus - rotavirus infections - rotavirus vaccine - epidemiology Gastroenteritis is a prevalent cause of childhood morbidity and mortality (Boschi-Pinto et al. 2008). Various agents are implicated in the aetiology of acute gastroenteritis, including rotavirus A (RVA), which is one of the most important aetiological agents of this syndrome, especially among children. Other studies have shown that more than 90% of children less than five years of age have been infected at least once by RVA and that most fatal cases associated with RVA infection occur in developing countries (Glass et al. 2006). The epidemiological characteristics of RVA infection, such as seasonality, mortality, mean age of infection, circulating genotypes, transmission route and minimum infectious dose differ among studies conducted in developed and developing countries, which could have an impact on the efficacy of the vaccine against RVA in different parts of the world (Parashar & Glass 2009). Different approaches have been used in the development of vaccines against RVA (Vesikari et al. 1984, Midthun & Kapikian 1996, Bresee et al. 1999, WHO 2009). In the last two decades, more vaccines against RVA have been developed and tested in clinical trials. Two vaccines, RotarixTM (GlaxoSmithKline) and Rotateq (Merck), have been licensed and are currently available in different parts of the world (Vesikari et al. 2006, WHO 2009). RotarixTM, an oral attenuated monovalent vaccine formulated with strain RIX4414 genotype G1P[8] (Gentsch et al. 2009), was first included in the Brazilian immunisation program in March of 2006. This study was performed to evaluate the impact of RotarixTM on RVA occurrence in Goiânia, state of Goiás (GO), Brazil, through detection and molecular characterisation of the virus in samples from vaccinated and unvaccinated children. For this study, 220 faecal samples were collected from an equal number of children in seven day-care centres [Municipal Centers for Early Childhood Education (CMEIs)] from February-November of 2008 in Goiânia. RVA was detected using two commercial kits with different detection methods: immunochromatography (Rotavirus adenovirus latex strip-Operon Biotechnologies, Germany) and the immunoenzymatic assay (Ridascreen® Rotavirus/r-biopharm). The positive results were confirmed by polyacrylamide gel electrophoresis, as previously described by Pereira et al. (1983), using a 20% faecal suspension in phosphate buffered saline (pH 7.4). The positive RVA samples were genotyped by reverse transcription-polymerase chain reaction (PCR) followed by Multiplex nested-PCR using the primers described by Gentsch et al. (1992), Gouvea et al. (1994) and Das et al. (1994). This study has been approved by the Committee in Ethics and Research from the Hospital Materno Infantil (protocol 22/08). Statistical analysis was performed using either the Chi-squared test or the Fisher's exact test. Statistical significance was accessed at p < 0.05. From the 220 collected samples, 139 were obtained from children that had been previously vaccinated with RotarixTM (1 or 2 doses) and 81 from unvaccinated children. Seventy-seven samples were considered diarrhoeic and 143 were not. Of the total samples, 3.6% were positive for RVA. If we only consider the samples collected from children with diarrhoea, 10.4% (p < 0.001) were positive for RVA, which confirms the relevance of diarrhoeal symptoms during RVA infection (Costa et al. 2004). Previous studies conducted in children from the same region found that 14.4-37.2% of the samples were positive for RVA (Cardoso et al. 2003, Costa et al. 2004), which was higher than the rate observed in the present study. Even if we consider the small sample size, which is a limitation of this study, our data still suggests that there was a decrease in RVA prevalence after the introduction of the vaccine by the Brazilian National Immunization Program. Recent studies conducted in both developed and developing countries have also reported a decrease in RVA circulation after the introduction of RotarixTM (De Vos et al. 2006, Leite et al. 2008, Correia et al. 2010, Lanzieri et al. 2010, Zeller et al. 2010). Among the positive samples, five were obtained from children that had completed the vaccination scheme, which includes two doses of RotarixTM (p > 0.05), and one had received only one dose (Table I). Regarding the gender of the children, five of the eight RVA-positive children were male and three were female. The RVA-positive samples were obtained from children at CMEIs in five districts. Therefore, it is unlikely that the virus spread from child to child inside the CMEIs; instead, the samples reflect the viral circulation in Goiânia during 2008. RVA infection was only detected during August and September of 2008, which is statistically significant (p < 0.001) (Table II). Previous studies conducted in the Central West Region have reported a clear RVA season (dry season April-August) (Cardoso et al. 2003, Andreasi et al. 2007). However, 2008 was somewhat atypical in that the dry season lasted until September (data from National Institute of Meteorology of Goiânia). Therefore, our results also indicate that the circulation of RVA in the Central West Region occurs predominantly during the dry season of the year (Cardoso et al. 2003). Viral genotyping showed that two of the eight RVA-positive samples could not be P-typed, whereas all positive samples could be G-typed; seven samples were characterised as G2 and one was characterised as G8. Five of the samples were genotype G2P[4] and one was G8P[4]. We acknowledge the small number of RVA-positive samples; however, a predominance of RVA genotype G2P[4] was observed as compared to the other genotypes, which suggests that the vaccine may not induce a protective response against this genotype. A predominance of the G2P[4] genotype has also been observed in different parts of Brazil, such as Aracajú (Gurgel et al. 2007), Recife (Nakagomi et al. 2008), Uberaba (Domingues et al. 2008), Rio de Janeiro (Carvalho-Costa et al. 2009), São Paulo (Sáfadi et al. 2010), Salvador and Goiânia (Munford et al. 2009). Nevertheless, the changing circulation pattern of RVA throughout the year should not be disregarded. Many countries where the vaccine was not implemented, such as El Salvador, Guatemala and Honduras (Patel et al. 2008), have also reported the emergence of the G2P[4] genotype. This is the first study conducted in Goiânia to evaluate the occurrence of gastroenteric virus among children in day-care. It is also the first study on RVA prevalence in children of this region after the introduction of RotarixTM by the National Immunization Program in 2006. Despite the small sample number, our findings suggest a decrease in RVA circulation among children under five years of age and the predominance of G2P[4] genotype, which could be associated with the introduction of the RotarixTM vaccine in children in Brazil. Further studies on RVA circulation are being conducted to better evaluate the possible impact of vaccination on viral prevalence and the emergence of genotypes in the region. References
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11084t2.jpg] [oc11084t1.jpg] |
| |||||||||

{kind=link}
{kind=link}