 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 4, August, 2011, pp. 541-545 ARTICLES Projecting the effectiveness of RotaTeq® against rotavirus-related hospitalisations in Brazil Antoine Chaouki El KhouryI, +; Thomas Christopher MastII; Max CiarletIII; Leona MarksonI; Michelle Gail GoveiaIV; Veridiana MunfordV; Maria Lucia RáczV IGlobal
Health Outcomes Financial support: Merck & Company, Inc Received 5 November
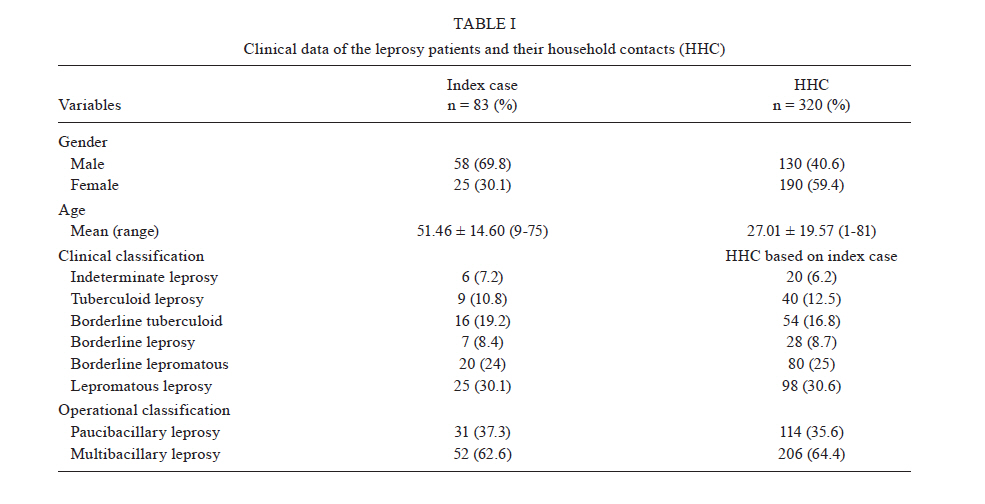
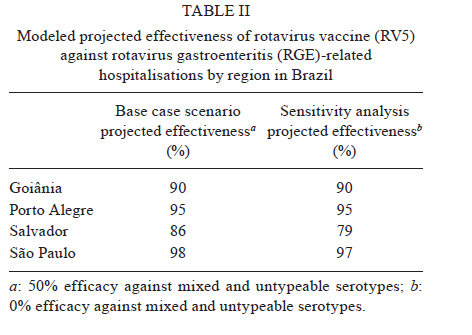
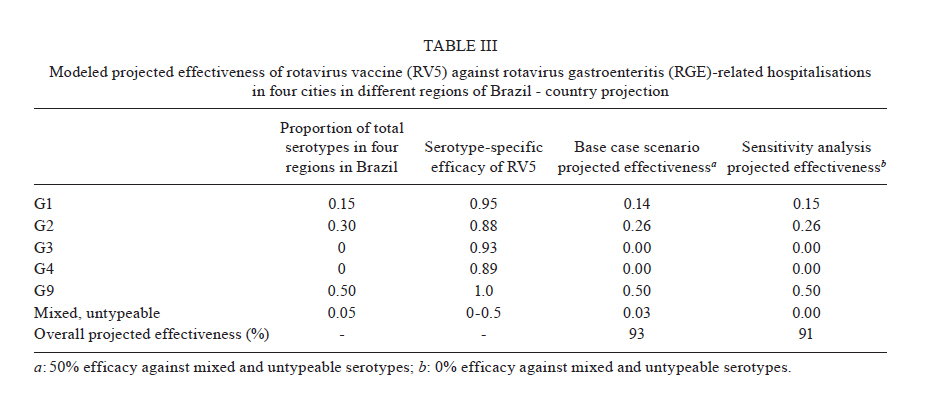
2010 Code Number: oc11092 ABSTRACT RotaTeq® (Merck & Company, Inc, Whitehouse Station, NJ, USA) is an oral pentavalent rotavirus vaccine (RV5) that has shown high and consistent efficacy in preventing rotavirus gastroenteritis (RGE) in randomised clinical trials previously conducted in industrialised countries with high medical care resources. To date, the efficacy and effectiveness data for RV5 are available in some Latin American countries, but not Brazil. In this analysis, we projected the effectiveness of RV5 in terms of the percentage reduction in RGE-related hospitalisations among children less than five years of age in four regions of Brazil, using a previously validated mathematical model. The model inputs included hospital-based rotavirus surveillance data from Goiânia, Porto Alegre, Salvador and São Paulo from 2005-2006, which provided the proportions of rotavirus attributable to serotypes G1, G2, G3, G4 and G9, and published rotavirus serotype-specific efficacy from the Rotavirus Efficacy and Safety Trial. The model projected an overall percentage reduction of 93% in RGE-related hospitalisations, with an estimated annual reduction in RGE-related hospitalisations between 42,991-77,383 in the four combined regions of Brazil. These results suggest that RV5 could substantially prevent RGE-related hospitalisations in Brazil. Key words: rotavirus - RotaTeq - effectiveness - hospitalisation - Brazil Rotavirus is the leading cause of hospitalisation and death due to acute gastroenteritis among infants and young children worldwide. Globally, more than two million hospitalisations and an estimated 527,000 deaths in children under five years of age are attributed to rotavirus annually (Parashar et al. 2003, 2009). Rotavirus is an important cause of childhood morbidity and mortality in Brazil, a country with a birth cohort of approximately four million, the largest of all Latin American countries (Nakagomi et al. 2008, PRB 2009). In Brazil, rotavirus accounts for an estimated 3,525,053 episodes of diarrhoea, 655,853 outpatient visits, 92,453 hospitalisations and 850 deaths annually in children five years of age or younger (Sartori et al. 2008). The significant morbidity and mortality related to rotavirus gastroenteritis (RGE) results in a tremendous economic burden on health care systems worldwide and greatly impacts families of children infected with the virus (Mast et al. 2009, Rheingans et al. 2009). International health agencies have determined that the development of rotavirus vaccines is the best means of preventing morbidity and mortality due to rotavirus infection (Bressee et al. 2005, Guarino et al. 2008). The five most prevalent rotavirus genotype/serotype combinations, which account for over 90% of cases of human rotavirus disease worldwide, are G1P1A[8] (Bressee et al. 2005), G2P1B[4], G3P1A[8], G4P1A[8] and G9P1A[8] (Gentsch et al. 1996, Santos & Hoshino 2005, Matthijnssens et al. 2008). A recent surveillance study of cities in different regions in Brazil (Goiânia, Midwest Region, Porto Alegre, South Region, Salvador, Northeast Region, and São Paulo, Southeast Region) from 2005-2006 identified G9 as the predominant rotavirus serotype, followed by G2 and G1 (Munford et al. 2009). In another surveillance study in the state of Minas Gerais, Brazil, from 2005-2007, 80% of rotavirus-positive stool samples were G1 (Nunes et al. 2010). These data highlight the diversity of rotavirus serotypes, with variations in prevalence, seasonality and genotype distribution among the different regions of Brazil (Matthijnssens et al. 2008). The diversity of rotavirus serotypes has important implications for the implementation of an effective rotavirus vaccine in a given region (Santos & Hoshino 2005). RotaTeq® [rotavirus vaccine (RV5), live, oral, pentavalent (Merck & Company, Inc, Whitehouse Station, NJ, USA) designated as RV5 by the Advisory Committee on Immunization Practices (Cortese & Parashar 2009)] was first introduced in the United States of America (USA) in February 2006. RV5 contains five human-bovine reassortant strains, each expressing a different human VP7 or VP4 rotavirus surface protein on the backbone of the parental bovine rotavirus WC3 strain (Vesikari et al. 2006, Heaton & Ciarlet 2007). The human surface proteins represent common human VP7 G serotypes - G1, G2, G3, and G4 - and the most common human VP4 P serotype, P1A[8] (Santos & Hoshino 2005, Martella et al. 2006, Matthijnssens et al. 2008). RV5 showed high and consistent efficacy in preventing RGE in randomised clinical trials that were previously conducted in countries with high standards of medical care (Vesikari et al. 2006, 2007, Block et al. 2007). In addition, recent effectiveness studies in the USA and Nicaragua showed that RV5 is effective in protecting against rotavirus-related hospitalisations (Patel et al. 2009, Boom et al. 2010). However, because of the variation in the regional and global distributions of rotavirus serotypes, it is important to account for local surveillance data, if available, to accurately predict vaccine effectiveness in regions where no trials or effectiveness studies have been conducted (Gentsch et al. 1996). The objective of this analysis was to project the potential effectiveness of RV5 against RGE-related hospitalisations in Brazil. METHODS This analysis utilised a mathematical efficacy projection model that was originally developed to project the efficacy of a live attenuated rotavirus vaccine in India (Rose & Singer 2008); the original model was validated using data from a phase II clinical trial with known rotavirus serotype distribution. The model used the vaccine efficacy obtained from phase III clinical trials as a baseline and adjusted the serotype specific efficacy by weights derived from the proportion of strains in India to generate the overall effectiveness of the monovalent vaccine in India. Although Rose and Singer (2008) use the term "projected efficacy", the term "projected effectiveness" will be used throughout this paper because the aim is to project the real impact of RV5 on the reduction in rotavirus-related hospitalisations. The current analysis adapted the Rose and Singer model to estimate the expected weighted serotype-specific effectiveness against RGE-related hospitalisation for Brazil using the proportion of locally prevalent serotypes and the published serotype-specific efficacy results from the Rotavirus Efficacy and Safety Trial (REST) (Vesikari et al. 2006, Rose & Singer 2008). Serotype data used in this model included published hospital rotavirus surveillance data collected in four cities from different regions in Brazil - Goiânia, Porto Alegre, Salvador and São Paulo - from 2005-2006, providing the proportions of rotavirus attributable to serotypes G1, G2, G3, G4 and G9 (Table I) (Munford et al. 2009). The model inputs for baseline serotype-specific vaccine efficacy were derived from the large-scale RV5 clinical trial, REST, that demonstrated the efficacy against RGE-related hospitalisations and emergency department (ED) visits for serotypes G1 [95%; 95% confidence interval (CI) 91.6-97.1], G2 (88%; 95% CI < 0-98.5), G3 (93%; 95% CI 49.4-99.1), G4 (89%; 95% CI 52.0-97.5) and G9 (100%; 95% CI 67.4-100.0) check the efficacy among infants from 11 countries (United States, Finland, Germany, Belgium, Sweden, Italy, Jamaica, Costa Rica, Mexico, Puerto Rico and Guatemala) (Vesikari et al. 2006, Munford et al. 2009). Given that the efficacy against mixed and non-typeable serotypes is unknown, sensitivity analyses of the modelled effectiveness were conducted. The base case scenario assumed an efficacy of 50% against mixed and non-typeable serotypes. The sensitivity analysis assumed an efficacy of 0% against mixed and non-typeable serotypes. Lastly, assuming that the routine vaccine delivery program for RV5 in Brazil will eventually reach vaccine coverage of 50-90%, the reduction in RGE-related hospitalisations was estimated by applying the projected efficacy against RGE hospitalisations to the number of RGE-related hospitalisations in children under five years of age in Brazil (Sartori et al. 2008). A sample calculation for the projected effectiveness by region in Brazil follows. In Goiânia, 32% of the total serotypes were G1. To obtain the projected effectiveness against rotavirus-related hospitalisation, the proportion of G1 in Goiânia (32%) was multiplied by the G1 serotype-specific efficacy of 95% as reported in REST (0.32 × 0.95 = 0.304). This calculation was done for G1, G2, G3, G4 and G9, respectively. The sum of the weighted serotype-specific data for Goiânia yielded a projected effectiveness of 90%. As noted, the efficacy for non-typeable serotypes was assumed to be 0% for the sensitivity analysis and 50% for the base case scenario calculations. The calculation of the overall effectiveness is based on the serotype-specific efficacy and the proportion of strains; this model does not project effectiveness against serotype-specific RGE-related hospitalisation. Similar methodology was used to calculate the projected effectiveness for Porto Alegre, Salvador and São Paulo. The overall effectiveness projections for Brazil used the pooled total proportions of each serotype for the four regions. RESULTS Projected effectiveness against RGE-related hospitalisations by region in Brazil - The modelled projected effectiveness against RGE-related hospitalisations for RV5 for São Paulo, Salvador, Goiânia and Porto Alegre are shown in Table II. The overall projected effectiveness by region in Brazil was estimated to be between 79-98%. Projected effectiveness against RGE-related hospitalisation in four combined regions in Brazil - country projection - The overall effectiveness in Brazil was estimated at 93% in the base case scenario (Table III). Based on the estimated 92,453 hospitalisations due to RGE annually in Brazil (Sartori et al. 2008) and assuming 50-90% vaccine coverage, the estimated expected annual reduction in RGE-related hospitalisations attributable to vaccination in children less than five years of age in Brazil is between 42,991-77,383 in the base case scenario. DISCUSSION The previously validated mathematical model applied in this study projected that RV5 is expected to have effectiveness against RGE-related hospitalisations ranging between 79-98% in four major Brazilian populations - Goiânia, Porto Alegre, Salvador and São Paulo; the overall effectiveness in Brazil, based on the projections in these four regions combined, is expected to be at least 93%, resulting in a total reduction of 42,991-77,383 hospitalisations. A recent case-control effectiveness study of RV5 in Nicaragua, a country with resource-constrained medical care, showed that the effectiveness against severe diarrhoea within one year after vaccination was 69% (Patel et al. 2009). An effectiveness study in USA showed that RV5 prevented 100% of rotavirus gastroenteritis-related hospitalisations and ED visits and 100% of their related costs (Wang et al. 2010). These results may be indicative of the effectiveness that would be evident in certain regions of Brazil, depending on how similar their populations and their medical care resources are to those of Nicaragua or the USA. Overall, the modelled effectiveness for Brazil is within the published estimates of effectiveness of Nicaragua and USA. Knowing that rotavirus serotypes can vary from region to region, these effectiveness projections used the most recent rotavirus surveillance data from four regions of Brazil to obtain each region's weighted serotype-specific effectiveness (Munford et al. 2009). The sensitivity analysis also accounted for variations in the effectiveness against mixed and non-typeable serotypes that may also affect overall vaccine effectiveness. Other studies have used alternative projection methodology to project the potential efficacy of RV5. One study projected that over a 10-year period, 45% of RGE-related hospitalisations could be prevented by vaccination in USA during an evaluation period following the implementation of the RV5 vaccination program (Curns et al. 2009). By the end of the study period, more than 65% of children under five years of age would be fully vaccinated and approximately 75% of rotavirus-related hospitalisations would be prevented (Curns et al. 2009). This study used a regression analysis approach that, similar to our method, incorporated vaccine efficacy data from REST; however, additional inputs for their model included previous estimates of hospitalisations, efficacy assumptions for one and two vaccine doses and increasing vaccine coverage rates over time. Another study that assumed 90% vaccine effectiveness and used timing and coverage similar to the diphtheria, tetanus and pertussis vaccine, projected that 70% of deaths due to rotavirus in Ghana could be prevented (Arvay et al. 2009). Lower rates of mortality prevention were projected when assumptions for vaccine effectiveness, timing of vaccine administration and coverage rates were varied and/or reduced. As in any modelled projections, there are limitations to this analysis. The number of rotavirus-related hospitalisations prevented by vaccination with RV5 depended on the projected efficacy of the vaccine used in the model. The efficacy of the vaccine depends on the availability and location of surveillance data used for the model inputs, as well as the seasonality of the disease, which may change over time. Changes in surveillance patterns over time and the tested populations may affect the predicted effectiveness of the vaccine by changing the underlying modelling assumptions. The projection methodology used in this study, as well as the previously published projection methods, provide useful information about the effectiveness of RV5 in regions where no clinical trials have been conducted. A recent World Health Organization (WHO) sponsored consultation on the use of rotavirus vaccines concluded that "even vaccines with lesser efficacy in developing countries, compared with industrialised countries, would still lead to substantial public health benefits" and that "criteria, such as the WHO mortality strata and local epidemiology of rotavirus infection, would be appropriate measures for extrapolating the clinical data to other regions and countries" (Steele et al. 2009). In conclusion, our study predicts that RV5 can have a substantial impact on RGE-related hospitalisations in Brazil. Information pertaining to RV5 potential effectiveness in Brazil may be useful to policymakers in Brazil when evaluating changing epidemiology in the region and ongoing rotavirus vaccination programs. REFERENCES
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11092t2.jpg] [oc11092t1.jpg] [oc11092t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}