 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, No. 6, Sept., 2011, pp. 716-724 Original Article Genetic polymorphisms of NAT2, CYP2E1 and GST enzymes and the occurrence of antituberculosis drug-induced hepatitis in Brazilian TB patients Raquel Lima de Figueiredo TeixeiraI; Renata Gomes MoratoI; Pedro Hernan CabelloI; Ligia Mayumi Kitada MunizII; Adriana da Silva Rezende MoreiraII; Afrânio Lineu KritskiII; Fernanda Carvalho Queiroz MelloII; Philip Noel SuffysIII; Antonio Basilio de MirandaIV; Adalberto Rezende SantosIII, + ILaboratório
de Genética Humana, Faculdade de Medicina, Universidade Federal do Rio
de Janeiro, Rio de Janeiro, RJ, Brasil
Received 1 March
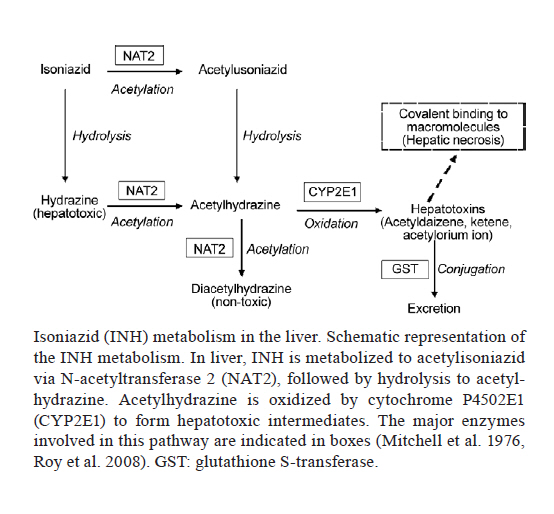
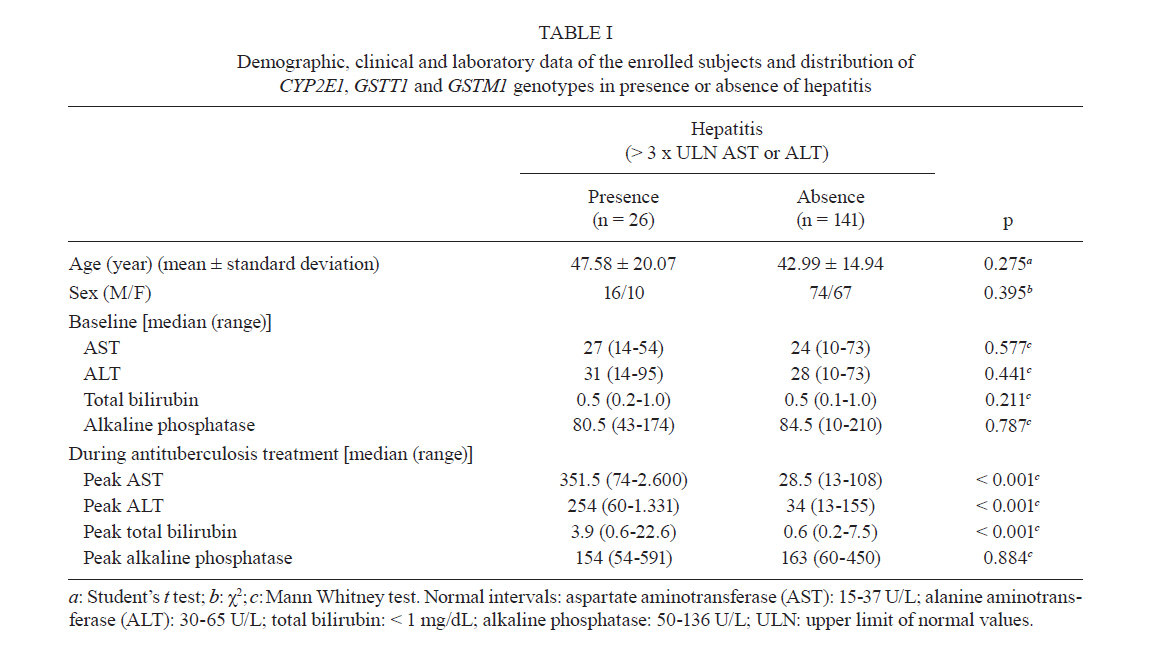
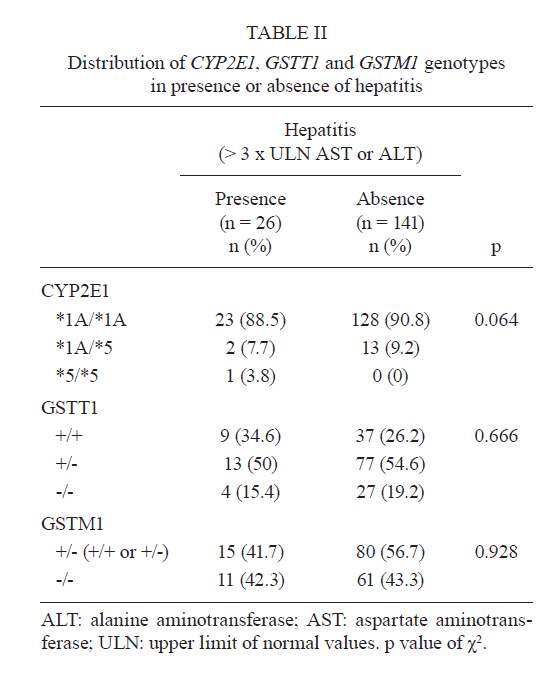
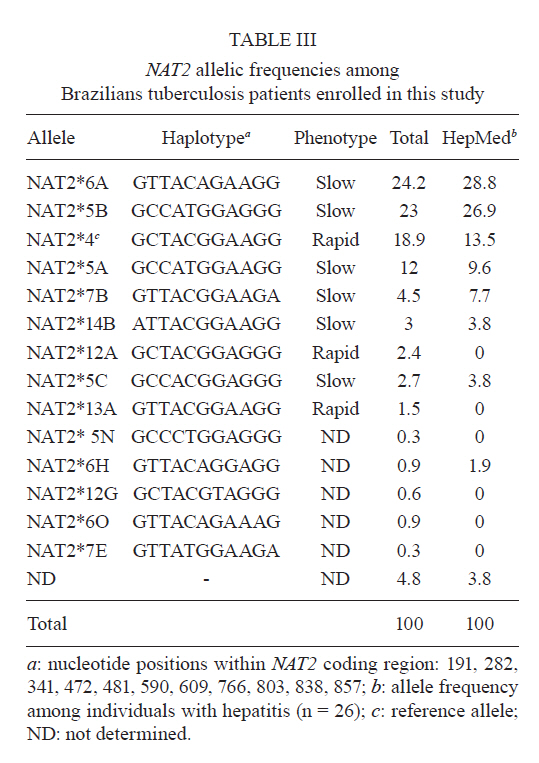
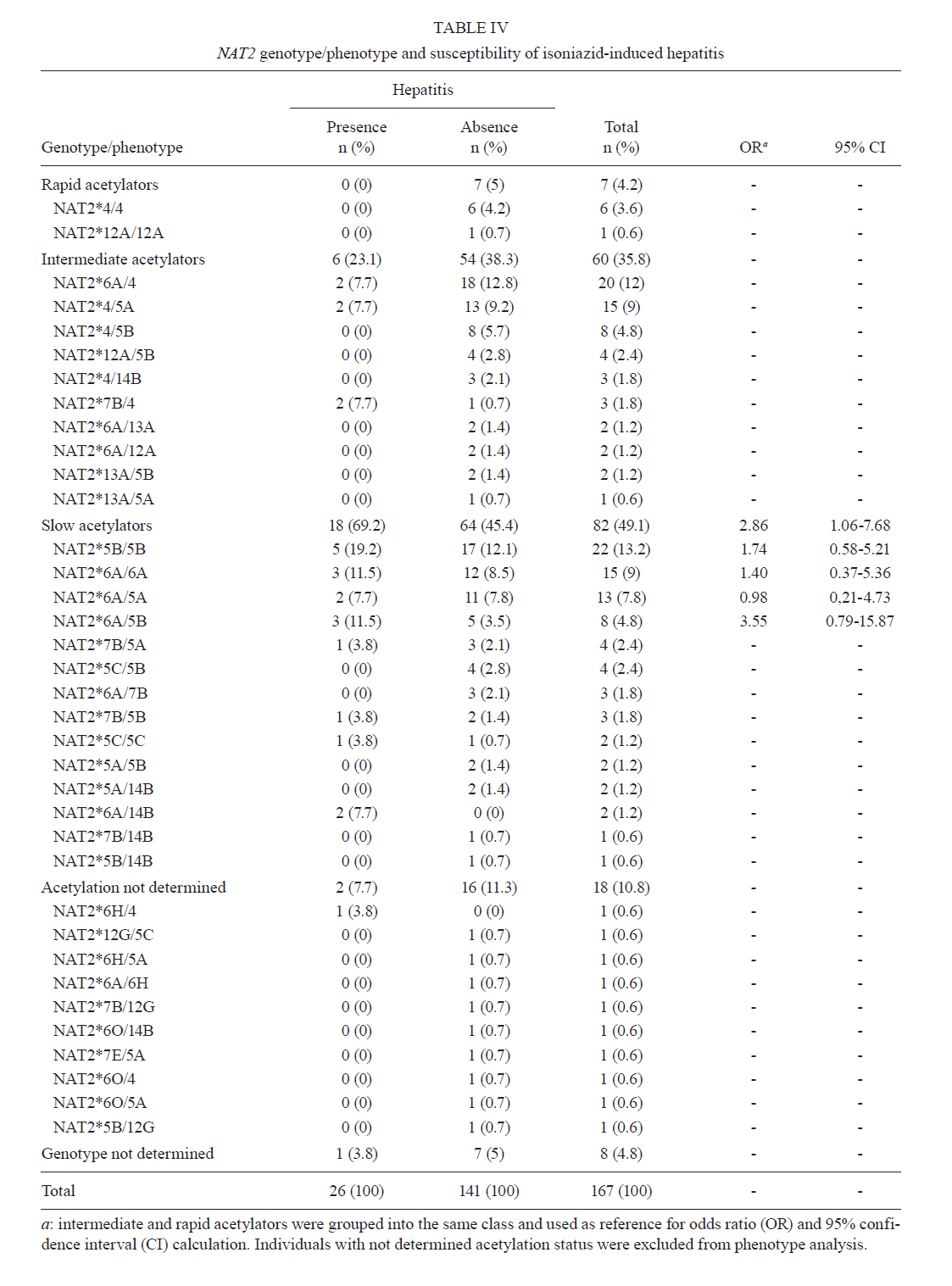
2011 Isoniazid (INH), one of the most important drugs used in antituberculosis (anti-TB) treatment, is also the major drug involved in hepatotoxicity. Differences in INH-induced toxicity have been attributed to genetic variability at several loci, such as NAT2, CYP2E1, GSTM1 and GSTT1, that code for drug-metabolising enzymes. Our goal was to examine the polymorphisms in these enzymes as susceptibility factors to anti-TB drug-induced hepatitis in Brazilian individuals. In a case-control design, 167 unrelated active tuberculosis patients from the University Hospital of the Federal University of Rio de Janeiro, Brazil, were enrolled in this study. Patients with a history of anti-TB drug-induced acute hepatitis (cases with an increase to 3 times the upper limit of normal serum transaminases and symptoms of hepatitis) and patients with no evidence of anti-TB hepatic side effects (controls) were genotyped for NAT2, CYP2E1, GSTM1 and GSTT1 polymorphisms. Slow acetylators had a higher incidence of hepatitis than intermediate/rapid acetylators [22% (18/82) vs. 9.8% (6/61), odds ratio (OR), 2.86, 95% confidence interval (CI), 1.06-7.68, p = 0.04). Logistic regression showed that slow acetylation status was the only independent risk factor (OR 3.59, 95% CI, 2.53-4.64, p = 0.02) for the occurrence of anti-TB drug-induced hepatitis during anti-TB treatment with INH-containing schemes in Brazilian individuals. Key words: hepatotoxicity, tuberculosis, isoniazid, NAT2, CYP2E1, GSTM1, GSTT1 Tuberculosis (TB) is one of the major causes of illness and death worldwide, especially in Asia and Africa. Globally, 9.2 million new cases and 1.7 million deaths from TB occurred in 2006, of which 0.7 million cases and 0.2 million deaths were in human immunodeficiency virus (HIV)-positive individuals (WHO 2008). Brazil is 16th among the 22 countries with the highest burden of TB, with 50 million infected subjects, 110,000 new cases and 6,000 annual deaths (Santos-Filho 2006, MS 2007). According to the guidelines for TB control, treating patients with antituberculosis (anti-TB) drugs is one of the most effective interventions and schemes containing isoniazid (INH), rifampicin, ethambutol and pyrazinamide are used as first-line TB therapy (Santos-Filho 2006, WHO 2008). Despite the availability of effective chemotherapeutic agents to treat TB, side effects such as hepatic disorder and peripheral neuritis are frequent, which limits the clinical use of the drugs and contributes to treatment relapse and the appearance of multidrug-resistant Mycobacterium tuberculosis strains (Garibaldi et al. 1972, Frieden et al. 2003). The most frequent and serious side effect of these drugs is hepatotoxicity (Garibaldi et al. 1972, Saukkonen et al. 2006). The liver has a central role in drug metabolism and detoxification and is consequently vulnerable to injury. Among the first line anti-TB drugs, INH is mainly responsible for the occurrence of drug-induced hepatic adverse effects and the metabolic intermediates of INH appear to be the cause of hepatotoxicity (Mitchell et al. 1976, Nelson et al. 1976, Woodward & Timbrell 1984). In the liver, INH is metabolised to acetylisoniazid via N-acetyltransferase 2 (NAT2) and is followed by hydrolysis to acetylhydrazine. Acetylhydrazine is oxidised by cytochrome P4502E1 (CYP2E1) to form hepatotoxic intermediates (Nelson et al. 1976, Timbrell et al. 1980). These reactive metabolites can destroy hepatocytes either by interfering with cell homeostasis or by triggering immunologic reactions in which reactive metabolites that are bound to hepatocyte plasma proteins may act as haptens (Lee 2003). The other metabolic pathway to generate toxic metabolites is the direct hydrolysis of INH to hydrazine, a potent hepatotoxin. NAT2 is also responsible for converting acetylhydrazine to diacetylhydrazine, a nontoxic component (Mitchell et al. 1976, Nelson et al. 1976, Woodward & Timbrell 1984) (Figure). Glutathione S-transferase (GST), an important phase II detoxification enzyme, is thought to play a protective role as an intracellular free radical scavenger, which conjugates glutathione with toxic metabolites that are generated from CYP2E1 (Sodhi et al. 1996). Sulphydryl conjugation facilitates the elimination of metabolites from the body and reduces the toxic effect (Hayes et al. 2005) (Figure). The common risk factors for hepatitis include advanced age, sex, malnutrition, complications of diseases, alcohol abuse, HIV infection and viral hepatitis B and C infections (Kimmoun & Samuel 2002, Saukkonen et al. 2006, Yew & Leung 2006). Recent studies have demonstrated that genetic polymorphisms in drug-metabolising enzymes, which influence their activation capacity and the generation of metabolites in the liver, might predispose an individual to hepatic adverse reactions (Ohno et al. 2000, Kita et al. 2001, Roy et al. 2001, Hiratsuka et al. 2002, Huang et al. 2002, 2003, 2007, Roy et al. 2006, Leiro et al. 2008). NAT2 is a polymorphic gene and single nucleotide polymorphisms (SNPs) in its coding region can alter its enzymatic activity (Fretland et al. 2001, Zang et al. 2007). In fact, three major genetically determined phenotypes are observed: rapid, intermediate and slow acetylators, which are inherited as codominant traits (Parkin et al. 1997, Kinzig-Schippers et al. 2005, Chen et al. 2006). The reference NAT2*4 allele and 62 other variants of the NAT2 gene were identified and classified in human populations depending on the combination of up to four SNPs present throughout the NAT2 coding region (louisville.edu/medschool/pharmacology/NAT.html). Currently, a total of 38 SNPs have been identified in the NAT2 coding region, including several rare SNPs described in different populations (Teixeira et al. 2010). Many studies have demonstrated that people with low NAT2 activity have a higher risk of developing hepatic disorders than those with high NAT2 activity (Ohno et al. 2000, Kita et al. 2001, Hiratsuka et al. 2002, Huang et al. 2002). However, other authors have observed that rapid acetylation is a risk factor for anti-TB drug-induced hepatitis and the controversy still remains (Mitchell et al. 1975, Singh et al. 1995a, b, Vuilleumier et al. 2006). The activity of CYP2E1 is also modulated by polymorphisms at several sites in the gene and higher activity of this enzyme may increase the synthesis of hepatotoxins and lead to hepatotoxicity. Two polymorphisms upstream of the CYP2E1 transcriptional start site are detectable by Pst I and Rsa I restriction enzymes and appear to be in complete linkage disequilibrium. Three genotypes of CYP2E1 are classified as *1A/*1A, *1A/*5 and *5/*5 by restriction fragment length polymorphism (RFLP) using Rsa I as the restriction enzyme (cypalleles.ki.se/index.htm). The presence of CYP2E1 *1A/*1A as a genetic marker of anti-TB drug-induced liver injury has been evaluated in a few studies with discordant results (Huang et al. 2003, Vuilleumier et al. 2006, Cho et al. 2007). The absence of GST activity due to homozygous null mutations at the GSTM1 and GSTT1 loci may also modulate susceptibility to drug-induced hepatitis, but the results reported in the literature are not homogenous (Roy et al. 2001, Huang et al. 2007, Leiro et al. 2008). Due to differences in NAT2, CYP2E1, GSTM1 and GSTT1 genotype frequencies among ethnic groups, evaluation of these genetic markers in the predisposition to drug-induced hepatitis during TB treatment is needed in admixed populations. Brazilians are members of one of the most heterogeneous population in the world, which is the result of five centuries of ethnic admixture of people from three continents: the European colonisers mainly represented by the Portuguese, the African slaves and the autochthonous Amerindians. Pharmacogenetic studies in this kind of population have important implications because the extrapolation of the data derived from well-defined ethnic groups is clearly not applicable. Recognising the diversity of the distribution of the genes and the high incidence of TB in Brazil, we have reported here the contribution of the NAT2, CYP2E1, GSTM1 and GSTT1 genetic variants to the susceptibility to anti-TB drug-induced hepatitis in TB patients. PATIENTS, MATERIALS AND METHODS Study design and patients - In a case-control design, a total of 167 unrelated active TB patients who had been treated between 1998-2008 were enrolled in this study. The patients had received treatment at the University Hospital Complex, Thoracic Institute/Clementino Fraga Filho University Hospital, Federal University of Rio de Janeiro, Brazil. This public hospital is a reference centre for HIV and other co-morbidities. Annually, approximately 150 TB cases are reported, of which 26% are infected by HIV, 13% have other co-morbidities (cancer, transplant, use of immunessupressors) and 8% have hepatitis or drug-induced hepatotoxicity. We retrospectively identified all of the patients who developed anti-TB drug-induced acute hepatitis (cases) and those who showed no evidence of anti-TB hepatic side effects (controls). The enrolled patients were genotyped to identify the genetic risk factors (polymorphisms in NAT2, CYP2E1, GSTM1 and GSTT1) associated with the susceptibility to anti-TB drug-induced hepatitis in Brazilian individuals. This study was approved by the Ethical Committee of the Oswaldo Cruz Foundation and written informed consent was obtained from all of the enrolled patients. Patients were selected using the following criteria: (i) age above 18 years, (ii) diagnosis of active TB, (iii) treatment with anti-TB drug regimens that include INH at the usual dosage (400 mg/day) and (iv) normal baseline serum transaminases [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)] before treatment for inclusion and (v) positive serological test for the HIV, hepatitis B virus or hepatitis C virus, (vi) alcohol abuse, (vii) history of chronic liver disease and (viii) pregnancy for exclusion. A volume of 3 mL of venous blood was collected from each volunteer and stored at -20ºC. Genomic DNA was isolated from 100 µL of frozen whole blood using the FlexiGene DNA Kit (Qiagen Inc, USA) according to the manufacturer's specifications. After extraction, DNA samples were stored at -20ºC. Liver function monitoring and the diagnosis of drug-induced adverse effects - Liver function tests, consisting of serum transaminases, total bilirubin and alkaline phosphatase measurements were performed once a month, during the patient's visit, using commercial kits according to the manufacturer's instructions. The following values were considered to be normal for the different tests: ALT 30-65 IU/L, AST 15-37 IU/L, total bilirubin up to 1 mg/dL and alkaline phosphatase 50-136 IU/L. Clinical and laboratory checkups were performed more frequently when hepatitis symptoms or abnormal serum transaminases levels were observed. According to the American Thoracic Society criteria (Saukkonen et al. 2006) and the Brazilian Health Ministry, cases are those individuals who showed anti-TB drug-induced hepatitis by an increase in serum transaminase values to higher than three times the upper limit of normal values (> 3 x ULN) and symptoms compatible with hepatitis. NAT2 genotyping and haplotype reconstruction - Genotyping of the NAT2 coding region and computational analysis were performed as previously described (Teixeira et al. 2007). In brief, a 1,093-bp fragment, which contains the entire coding region of NAT2, was amplified by polymerase chain reaction (PCR) and subsequently sequenced on both DNA strands using the primers for amplification and two additional internal primers (Teixeira et al. 2007). Sequencing was performed using the ABI PRISM BigDye Terminator v. 3.1 Kit (PE Applied Biosystems) according to the manufacturer's recommendations on an ABI PRISM 3730 DNA Analyser (PE Applied Biosystems). The sequence analysis and SNP identification were performed using SeqScape Software v.2.5 (PE Applied Biosystems) with the sequence (GenBank: AY331807) as the reference. To solve the haplotype pair of each patient and to define the acetylation status, haplotype reconstruction was performed using the program PHASE v2.1.1 (Stephens et al. 2001, Stephens & Donnelly 2003) with the default model for recombination rate variation (Li & Stephens 2003). Five independent runs with 1,000 interactions, 500 burn-in interactions and a thinning interval of one were performed. The best run that showed the maximum consistency across five runs was chosen. Additionally, the consistency of the results that applied the PHASE algorithm repeatedly with default and varying values of the number of interactions, burn-in interactions and the thinning interval was pursued. CYP2E1 genotypes identification - To genotype the SNP -1053C>T in the CYP2E1 gene promoter region and to determine the three genotypes (*1A/*1A; *1A/*5 and *5/*5), a PCR with the amplification primers CYP2E1F 5'CCAGTCGAGTCTACATTGTCA3' and CYP2E1R 5'TTCATTCTGTCTTCTAACTGG3' were performed followed by RFLP as previously described (Stephens et al. 1994). Briefly, after the amplification of a 413-bp DNA fragment flanking the -1053C>T SNP, the PCR product was digested with the Rsa I restriction enzyme. Evaluation of the fragment digestions was achieved by electrophoresis on a 2% agarose gel followed by ethidium bromide staining (0.5 µg/mL). GSTT1 and GSTM1 genotype identification - To determine the presence or absence of the GSTM1 and GSTT1 genes, two separate multiplex PCR reactions were performed as previously reported with minor modifications (Bailey et al. 1998, Sprenger et al. 2000). The GSTM1 wild-type allele (+) was identified by the PCR method using primers M1 5'CTGCCCTACTTGATTGATGGG3' and M2 5'CTGGATTGTAGCAGATCATGC3' to obtain a 273-bp PCR product (Bailey et al. 1998). Co-amplification of a 536-bp fragment of the @@β-globin gene using the primers Beta1 5'GGTTGGCCAATCTACTCCCAGG3' and Beta2 5'GCTCACTCAGTGTGGCAAAG3' was performed as an internal control. The PCR reaction mixture was performed in a total volume of 50 µL containing 100 ng of genomic DNA, 240 ng of each GSTM1 primer and 10 pmoles of each @@β-globin primer, PCR Gold buffer (1x), 3 mM MgCl2, 0.1% Triton X-100, 0.2 mM of each dNTP and 2U AmpliTaq Gold® DNA polymerase (PE Applied Biosystems). Amplification conditions consisted of an initial denaturing step of 95ºC for 10 min, followed by 30 cycles of 95ºC for 30 s, 64ºC for 1 min and 72ºC for 6 min. The homozygous GSTM1 null genotype (-/-) was detected by the absence of the 273-bp fragment. Individuals who presented with the 273-bp fragment were classified as +/- (+/+ or +/-) and contained at least one wild-type allele. For GSTT1 genotyping and identification of the three genotypes (GSTT1*A/GSTT1*A, GSTT1*A/GSTT1*0 and GSTT1*0/GSTT1*0), a 1,460-bp GSTT1*0 specific fragment was co-amplified with a 460-bp fragment corresponding to the GSTT1*A allele in a single reaction tube using primers T1 5'CCAGCTCACCGGATCATGGCCAG3', T2 5'GAGATGTGAGGACCAGTAAGGAAGG3', T3 5'CAGTTGTGAGCCACCGTACCC3' and T4 5'GAGGGGGCCAGCAACTATCG3' (Sprenger et al. 2000). PCR was performed in a 50 µL reaction mix containing 150 ng genomic DNA, PCR buffer (1x), 100 ng of each primer, 1.5 mM MgCl2, 100 µg/mL bovine serum albumin, 0.2 mM of dNTPs and 2U DNA polymerase (Biotools, Madrid/Spain). Amplification conditions consisted of a touchdown PCR with an initial denaturing step (94ºC for 5 min) followed by 20 cycles of 94ºC for 1 min, 68ºC for 1 min (with a decrease of 0.5ºC per cycle at the annealing temperature) and 72ºC for 1 min and 30 s. An additional 15 cycles of 94ºC for 1 min, 58ºC for 1 min and 72ºC for 1.5 min were performed. Evaluation of the PCR amplicons was achieved by electrophoresis on a 2% agarose gel followed by ethidium bromide staining. Statistical analysis - Data are expressed as the mean ± standard deviation (for normal distribution) or as the median with range (for non-normal distribution). Expected genotype frequencies were calculated from the respective single allele frequencies according to the Hardy-Weinberg equation. The observed and expected gene frequencies were compared using a χ2 test for Hardy-Weinberg equilibrium, except for the GSTM1 genotype, for which the heterozygous frequency was not determined. Qualitative variables were compared using a χ2 test with Yates correction or Fisher's exact test when appropriate. Quantitative variables were analysed using Student´s t test for normal distribution or Mann-Whitney U-test (2 groups) and Kruskal-Wallis test (up to 2 groups) for non-normal distribution. Odds ratios (OR) and confidence intervals (CI) were calculated to evaluate the susceptibility of NAT2 haplotypes, genotypes and inferred acetylation status to anti-TB drug-induced hepatic adverse effects. Multivariate analysis was performed to evaluate the adjusted risk of anti-TB drug-induced hepatic adverse effects in the different genotypes using a stepwise logistic regression analysis. All of the analyses were performed using the statistical software SPSS 12.0 for Windows (SPSS Inc, Chicago, IL). All of the statistical tests were evaluated at a 0.05 significance level. Results Among the 167 individuals enrolled in this study, 26 were diagnosed with anti-TB drug-induced hepatitis. No statistical differences in age, sex and basal liver function tests between the cases and controls were observed (Table I). The medians of ALT, AST and total bilirubin during treatment were significantly different between the cases and controls, showing clinically significant liver injury among cases (Table I). The CYP2E1 and GSTT1 genotypes under investigation were in Hardy-Weinberg equilibrium (p > 0.05). No significant differences in the frequencies of CYP2E1, GSTM1 and GSTT1 genotypes existed between the cases and the controls (Table II). After NAT2 sequencing and haplotype pair reconstruction, 14 NAT2 alleles were identified, of which two were new and are described here for the first time (Table III). Although the distribution of the NAT2 alleles between the cases and controls was not statistically different, the alleles with low activity were more frequent in cases, while the functional alleles were more frequent in the control group (Table IV). The genotypes of eight individuals (4.8%) could not be solved after the reconstruction by PHASE v2.1.1. In addition, we identified 10 other individuals for whom the acetylation status has not yet been characterised (Table IV). Therefore, a total of 18 (10.8%) individuals were excluded from the NAT2 analysis. Of the 149 remaining individuals analysed for the NAT2 acetylation status, 82 (55.03%) were slow acetylators, 60 (40.27%) were intermediate acetylators and only seven (4.7%) individuals showed rapid acetylation genotypes. The slow acetylators had higher median serum ALT and AST levels than rapid/intermediate acetylators during the treatment (ALT: p = 0.03; AST: p = 0.01). No association of any specific NAT2 genotype with susceptibility for the occurrence of anti-TB drug-induced hepatitis was present (Table IV). The risk of anti-TB drug-induced hepatitis occurrence was significantly higher in slow acetylators than in rapid/intermediate acetylators (22% vs. 9%, OR 2.86, 95% CI, 1.06-7.68, p = 0.04) (Table IV). Variables such as age, sex, acetylation status and CYP2E1, GSTM1 and GSTT1 genotypes were further analysed in a multivariate logistic regression model. After adjustment, slow acetylation was the only risk factor for anti-TB drug-induced hepatitis (OR 3.59, 95% CI, 2.53-4.64, p = 0.02). We have also performed similar analyses classifying individuals into three acetylation phenotypes (slow, intermediate and rapid acetylators) and observed similar results (OR 3.47, 95% CI, 2.43-4.47. p = 0.02), which confirmed the association with only the slow acetylator phenotype. Discussion The association of INH with hepatitis during anti-TB treatment has already been reported (Steele et al. 1991, Salpeter 1993, Fountain et al. 2005). In addition, an association with other drugs with this outcome has been reported in combination with INH (Tostmann et al. 2008). NAT2, which is expressed in the liver, is the main enzyme involved in INH metabolism. In agreement with the literature data from other populations (Ohno et al. 2000, Kita et al. 2001, Hiratsuka et al. 2002, Huang et al. 2002), our findings suggest that NAT2 is the genetic factor that is responsible for the predisposition to anti-TB drug-induced hepatitis in Brazilian individuals. The incidence of elevated levels of serum transaminases was significantly higher in slow acetylators than in rapid/intermediate acetylators. These results corroborate the current hypothesis that the acetylator status may be a risk factor for the hepatic side effects of INH. Indeed, slow acetylators acetylate not only INH more slowly but also acetylhydrazine, the immediate precursor of toxic intermediates, to harmless diacetylhydrazine (Ellard & Gammon 1976, Lauterburg et al. 1985). This protective acetylation is further suppressed by INH competition. Therefore, slow acetylators may be prone to higher accumulation rates of INH toxic metabolites. In addition, another important route for generating toxic intermediates from INH is by the direct hydrolysis of INH without acetylation (Timbrell et al. 1977). This reaction produces hydrazine, which can induce hepatic injury (Timbrell et al. 1977, 1980). Pharmacokinetic studies have shown that the serum concentration of hydrazine is significantly higher in slow acetylators than in rapid acetylators, likely due to the high concentration of INH. The high amount of INH disposed of through this pathway is likely to lead to enhanced hydrolysis to hydrazine because the rate of metabolic conversion of INH to acetylisoniazid is lower in slow than in rapid acetylators (Sarma et al. 1986, Fukino et al. 2008). All of these drug disposal processes may support the finding that slow acetylators are prone to INH-induced hepatitis. Few studies have reported the absence of a relationship between acetylation status and hepatitis during TB treatment (Singh et al. 1995a, b, Vuilleumier et al. 2006) or observed that rapid acetylators could be susceptible to this type of side effect (Mitchell et al. 1975). Here, genotyping of the NAT2 gene was performed by sequencing, overcoming the possible problems of misclassification of the acetylation status. Another important aspect to be considered here is that in our study, patients were treated with 400 mg of INH instead of the 300 mg used in the study conducted by Vuilleumier et al. (2006). CYP2E1, one of the cytochrome P450 enzymes, may convert acetylhydrazine into hepatotoxins that affect anti-TB drug-induced hepatotoxicity. Some studies have shown the relationship between the CYP2E1*1A/*1A genotype and the risk of anti-TB drug-induced hepatitis (Huang et al. 2003, Vuilleumier et al. 2006). However, a recent study in a Korean population did not confirm those results (Cho et al. 2007). In the studied population, in contrast with the findings for the Taiwanese population (Huang et al. 2003), the mutant homozygous CYP2E1 *5/*5 is rare (0.5% vs. 4.7%, respectively) (Sigimura et al. 1995, Huang et al. 2003). Indeed, we found only one individual with CYP2E1 *5/*5 genotype among the 167 patients enrolled in this study (0.6%) with no association between the CYP2E1 genotypes and hepatic side effect occurrence. The discrepancy of our results may be due to the differences in the frequencies of wild-type CYP2E1*1A and mutant CYP2E1*5 alleles among Brazilian individuals. Therefore, further studies with a larger sample size should be performed in the Brazilian population to better evaluate the relationship between the CYP2E1 genotypes and adverse reactions during TB treatment. Finally, the frequencies of homozygous GSTM1 and GSTT1 null genotypes in this study were in accordance with other studies in a Brazilian population (Suarez-Kurtz et al. 2007), showing the consistency of our data. Few studies have observed the relationship between GST genotypes and anti-TB drug-induced hepatotoxicity (Roy et al. 2001, Huang et al. 2007, Leiro et al. 2008). Indeed, Roy et al. (2001) have observed a significant association between the homozygous GSTM1 null polymorphism and the anti-TB drug-induced hepatotoxicity in Indian TB patients. Recently, Huang et al. (2007) have found similar results in a Chinese population. In contrast, the presence of the homozygous GSTT1 null polymorphism was similar between the cases and the controls in both studies. However, the same analysis in Spanish TB patients showed an opposite effect; the homozygous GSTT1 null polymorphism was highly associated with anti-TB drug-induced hepatotoxicity and no significant associations were found between the homozygous GSTM1 null polymorphism and hepatotoxicity (Leiro et al. 2008). Therefore, further studies should be performed to evaluate the role of these genetic factors in the susceptibility to hepatitis occurrence. To our knowledge, this is the first study in which the four candidate genes, which are known to be involved in the INH metabolic pathway, were evaluated simultaneously as risk factors for anti-TB drug-induced hepatitis in an admixed population. Here, the decision to exclude other variables that are potentially associated with hepatitis was pursued to confirm the association of genetic factors with the key outcome. Genotyping interindividual variability at the NAT2 locus as an additional laboratory tool to predict anti-TB drug-induced hepatitis and other side effects is an emerging reality and will help not only in the determination of the most suitable dosage for individual patients, but also in the reduction of necessary outpatient visits and hospitalisations. Acknowledgements To the nursing service of the Hospital Tuberculosis Control Program/Thoracic Diseases Institute/Clementino Fraga Filho University Hospital, for sample collection, and for the support from the PDTIS-FIOCRUZ sequencing and Bioinformatics Platforms. References
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11121t2.jpg] [oc11121t4.jpg] [oc11121t1.jpg] [oc11121f1.jpg] [oc11121t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}