 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memórias do Instituto Oswaldo Cruz, Vol. 106, Special Issue, pp. 34-43 Original Article Antibodies against the Plasmodium falciparum glutamate-rich protein from naturally exposed individuals living in a Brazilian malaria-endemic area can inhibit in vitro parasite growth Lilian Rose Pratt-RiccioI, +; Cesare Bianco-JuniorI; Paulo Renato Rivas TotinoI; Daiana De Souza Perce-Da-SilvaI; Luciene Aquino SilvaI; Evelyn Kety Pratt RiccioI; Vítor Ennes-VidalI; Ana Gisele Costa Neves-FerreiraII; Jonas PeralesII; Surza Lucia Gonçalves Da RochaII; Fabrício Dias-Da-SilvaI; Maria de Fátima Ferreira-da-CruzI; Cláudio Tadeu Daniel-RibeiroI; Joseli De Oliveira-FerreiraIII; Michael TheisenIV; Leonardo José De Moura CarvalhoI; Dalma Maria BanicI ILaboratório
de Pesquisas em Malária Received 15 April
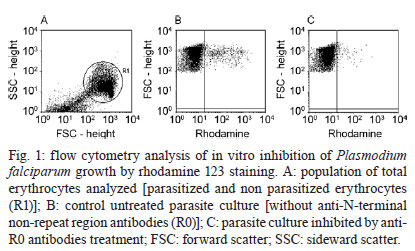
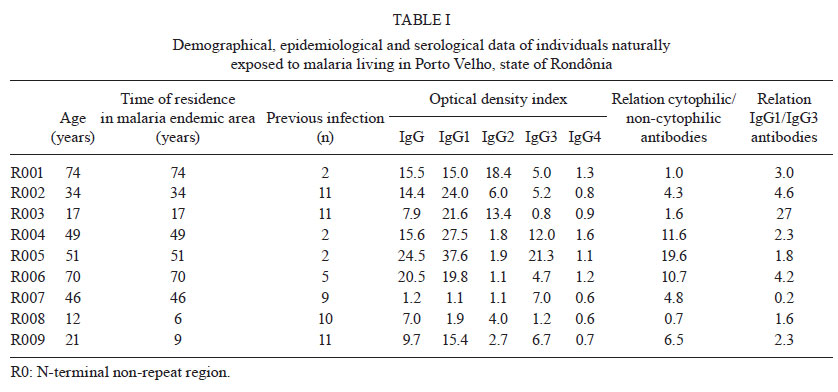
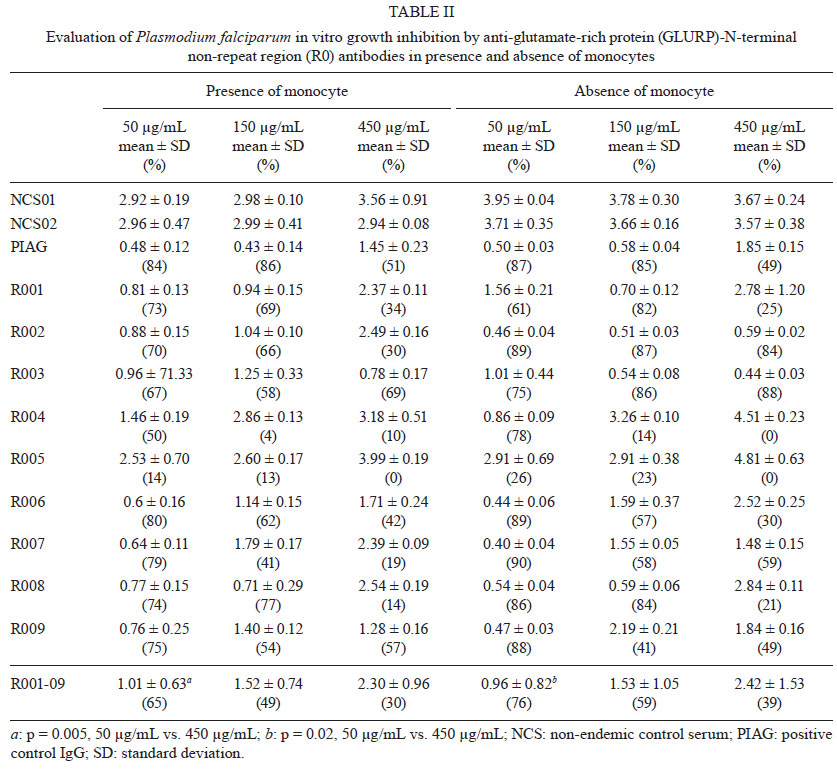
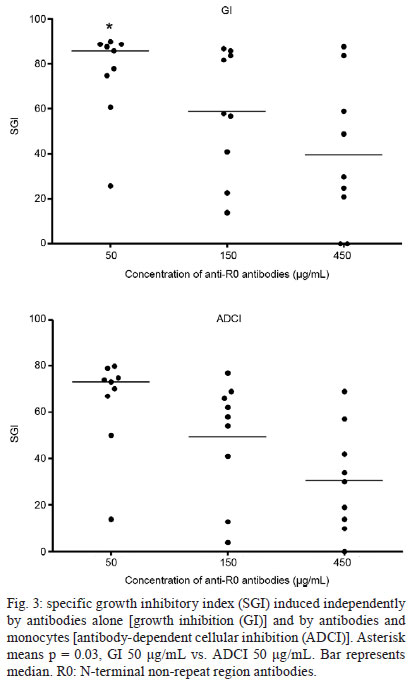
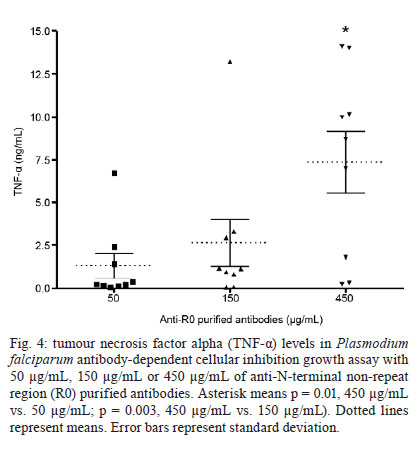
2011 Code Number: oc11138 Abstract The glutamate-rich protein (GLURP) is an exoantigen expressed in all stages of the Plasmodium falciparum life cycle in humans. Anti-GLURP antibodies can inhibit parasite growth in the presence of monocytes via antibody-dependent cellular inhibition (ADCI), and a major parasite-inhibitory region has been found in the N-terminal R0 region of the protein. Herein, we describe the antiplasmodial activity of anti-GLURP antibodies present in the sera from individuals naturally exposed to malaria in a Brazilian malaria-endemic area. The anti-R0 antibodies showed a potent inhibitory effect on the growth of P. falciparum in vitro, both in the presence (ADCI) and absence (GI) of monocytes. The inhibitory effect on parasite growth was comparable to the effect of IgGs purified from pooled sera from hyperimmune African individuals. Interestingly, in the ADCI test, higher levels of tumour necrosis factor alpha (TNF-α) were observed in the supernatant from cultures with higher parasitemias. Our data suggest that the antibody response induced by GLURP-R0 in naturally exposed individuals may have an important role in controlling parasitemia because these antibodies are able to inhibit the in vitro growth of P. falciparum with or without the cooperation from monocytes. Our results also indicate that TNF-α may not be relevant for the inhibitory effect on P. falciparum in vitro growth. Key words: malaria - Plasmodium falciparum - GLURP - antibodies - biological activity - growth inhibition Introduction Malaria remains a major public health problem, which affects approximately 225 million people worldwide and causes around 781,000 deaths, mostly in children under five years old (WHO 2010). In areas where malaria is highly endemic, the parasite rate and density decline with increasing age and severe disease and mortality are usually restricted to early childhood (McGregor 1974, 1987, Cattani et al. 1986, Greenwood et al. 1987). Adolescents and adults are usually free of clinical symptoms of malaria, although they may maintain low parasitemias throughout the transmission season (Marsh & Snow 1999). It has been proposed that these changes reflect the acquisition of clinical immunity against malaria infection. The results from in vivo studies suggest that one of the mechanisms underlying clinical immunity against malaria is the containment of parasite multiplication by antibodies (Cohen et al. 1961, McGregor & Carrington 1963, Sabchareon 1991). Antibodies that inhibit blood stage replication of Plasmodium falciparum are believed to be important in mediating both naturally acquired and artificially induced immunity generated by blood-stage vaccine candidates (Cohen et al. 1969, Good et al. 2004). Therefore, research has pursued a vaccine capable of inducing the formation of specific antibodies in sufficient quantities and mainly functionally able to participate in protecting against the parasite. In this context, several proteins have been identified and selected as candidate molecules for use in the composition of a malaria vaccine. Among these, the P. falciparum glutamate-rich protein (GLURP) appears to be a promising candidate (Hogh et al. 1992, 1993, Dziegiel et al. 1993, Theisen et al. 1998, Soe et al. 2004, Pratt-Riccio et al. 2005). The GLURP protein is an exoantigen expressed at all stages of development in the parasite life cycle in human hosts, including on the surface of newly released merozoites (Borre et al. 1991). It is highly antigenic and the gene encoding GLURP exhibits low polymorphism in geographically different P. falciparum isolates (Theisen et al. 1995, Stricker et al. 2000). GLURP contains an N-terminal non-repeat region (R0), a central non-repeat region (R1) and a C-terminal repeat region (R2). Immuno-epidemiological studies performed in high transmission areas have demonstrated a high prevalence of antibodies against GLURP in immune adults (Boudin et al. 1993, Dziegiel et al. 1993) and have shown that high levels of GLURP-specific antibodies are significantly associated with low parasite densities (Hogh et al. 1992, 1993) and protection against clinical malaria (Dziegiel et al. 1993, Dodoo et al. 2000, Oeuvray et al. 2000). Moreover, GLURP is a target antigen for antibodies involved in antibody-dependent cellular inhibition (ADCI) (Theisen et al. 1998), which is believed to be involved in acquired protective immunity against malaria (Khusmith & Druilhe 1983, Lunel & Druilhe 1989, Bouharoun-Tayoun et al. 1990, Bouharoun-Tayoun & Druilhe 1992). In the ADCI mechanism, cytophilic antibodies (IgG1 and IgG3 but not IgG2 and IgG4) act in conjunction with blood monocytes to contain parasite multiplication. In vitro studies have indicated that affinity-purified human IgG against the non-repeat R0 and R2 repeat regions can inhibit parasite growth in the presence of monocytes, although anti-R0 antibodies exerted a greater ADCI effect than anti-R2 antibodies (Theisen et al. 1998). In Brazil, malaria is hypo to meso-endemic, is present throughout the year with clear seasonal fluctuations and is frequently associated with the migratory movements of non-immune individuals to areas where malaria is endemic (Oliveira-Ferreira et al. 2010). The population exposed to malaria in these areas is vulnerable and infections tend to be followed by clinical symptoms (Marques 1987, Castilla & Sawyer 1993). For a long time, asymptomatic cases have been considered rare in Brazil (Prata et al. 1998). However, asymptomatic infection by P. falciparum and Plasmodium vivax have been detected in the states of Rondônia (RO) and Amazonas, suggesting that subjects exposed to malaria in Brazil can also develop acquired resistance to clinical malaria despite the different epidemiological profile from the one observed in Africa (Camargo et al. 1999, Alves et al. 2002, Coura et al. 2006). Because the great majority of growth-inhibitory antibody studies have been conducted in African countries, we aimed to verify the antiplasmodial activity of anti-GLURP antibodies present in the sera from individuals living in a Brazilian malaria-endemic area with a low level of transmission. Subjects, Materials and Methods Study site and volunteers - Written informed consent was obtained from all donors before blood samples were collected. Donors giving informed consent answered a standard questionnaire to evaluate the possible degree of malaria exposure. Venous peripheral blood was collected into heparinised tubes. Plasma was obtained from the blood samples by centrifugation and was aliquoted and stored at -20ºC. The plasma donors comprised nine adult individuals living in rural villages situated near Porto Velho, the capital of RO, in the Brazilian Amazon malaria endemic region. In this region, malaria transmission is unstable with an increase in the number of cases between April-September (Rodrigues et al. 2008). The population of these villages is composed of natives and Brazilian migrants that have inhabited this area for variable periods of time since the 1970s. The age range of the studied individuals was 18-74 years old (41 ± 22). The subjects had spent all or most of their lives in these locations (32 ± 24) and they referred to repeated malaria attacks (7 ± 4). All donors presented parasite-negative thin and thick Giemsa-stained blood smears at the time of blood collection. For the inhibition assays, non-endemic control serum (NCS) samples from two individuals from the malaria laboratory staff [Rio de Janeiro (RJ), Brazil], who had neither a history of malaria nor contact with malaria transmission areas, were included in our study as negative controls. Positive control IgG (PIAG, kindly provided by Dr Pierre Druilhe, Institut Pasteur, Paris) was purified from a pool of sera obtained from 30 African adults living permanently in Garitenga, Burkina Faso, where malaria is holo-endemic. Sera donors were free of clinical symptoms and of heavy parasitemia and thus were regarded as immune individuals (Bouharoun-Tayoun et al. 1990, Lundquist et al. 2006). PIAG has previously been found to confer passive protection against malaria and to cause a high ADCI effect (Sabchareon et al. 1991, Galamo et al. 2009). For the enzyme linked immunosorbent assay (ELISA) against the R0 recombinant protein, sera from 25 RJ controls who had neither a history of malaria nor contact with malaria transmission areas were used to establish the normal range of the assay. The study was reviewed and approved by the Oswaldo Cruz Foundation Ethical Committee (258/04). Recombinant GLURP-R0 protein - The recombinant protein R094-489 corresponding to the non-repeat amino-terminal region was expressed in Escherichia coli and purified, as described elsewhere (Theisen et al. 1995). ELISA for R0 recombinant protein - An ELISA with recombinant GLURP-R094-489 was performed as previously described (Theisen et al. 1995). Microtitre 96-well plates (Maxisorp, Nunc, Roskilde, Denmark) were coated overnight at 4ºC with 1 µg/mL of recombinant R0 (100 µL/well) in carbonate-bicarbonate buffer at pH 9.6. Uncoated sites were blocked for 2 h with 2.5% (w/v) powdered milk containing phosphate-buffered saline (PBS) and incubated for 2 h at room temperature (RT) with plasma diluted 1:100 in 1.25% (w/v) powdered milk containing 0.05% (v/v) PBS and Tween 20 (PBS-T20). The plates were washed with PBS-T20, mouse anti-human IgG (Sigma, St. Louis, MO) diluted 1:2,000 in 1.25% (w/v) powdered milk containing PBS-T20 was added and the plates were incubated for 1 h at RT. To detect specific IgG subclasses, plates were incubated for 2 h at 37ºC with murine MAb labelled with peroxidase specific for the human IgG1 (clone 4E3), IgG2 (clone 31-7-4), IgG3 (clone HP 6050) and IgG4 (clone HP 6025) subclasses (Southern Biotech, Alabama, USA). The plates were then washed with PBS-T20 and 100 µL of a solution containing 0.4 mg/mL of o-phenylendyamine and hydrogen peroxide (H2O2) in citrate phosphate buffer, pH 5.0, was added to each well. The plates were incubated for 30 min at RT in the dark and 50 µL of 2N H2SO4 was then added to each well to stop the reaction. Plates were read at 492 nm in a spectrophotometer (Spectramax 250, Molecular Devices, Sunnyvale, CA). The cut-off value was determined as the mean optical density (OD) plus three standard deviations from RJ controls (cut-off values: IgG = 0.122, IgG1 = 0.132, IgG2 = 0.156, IgG3 = 0.143, IgG4 = 0.151). To standardise the OD data obtained in different experiments, OD index was calculated for each immunoglobulin determination as the ratio of the observed OD to the cut-off values. A sample with an OD index > 1.0 was considered positive. IgG purification - IgG was purified from individual plasma samples and from NCS and PIAG by affinity chromatography using a 1-mL Hi-Trap Protein G column (GE Healthcare Life Sciences), according to the manufacturer's instructions. After centrifugation (14,000 rpm, 5 min), the supernatant from each plasma sample was filtered through a 0.45 µm filter (Millipore) and loaded onto a column equilibrated with 0.02 M sodium phosphate buffer, pH 7.0, at a flow rate of 1.0 mL/min. The IgG fraction was eluted with 0.1 M glycine/HCl buffer, pH 2.7, at the same flow rate. The eluate was immediately neutralised with 1 M Tris-HCl, pH 9.0, pooled and dialysed against PBS. The IgG purity was estimated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis upon staining the gels with Coomassie blue dye. GLURP-specific IgG antibody purification - The GLURP-specific IgG antibody was purified from total IgG by affinity chromatography using a 1-mL Hi-Trap NHS-activated affinity column (GE Healthcare Life Sciences) containing GLURP94-489 (R0) immobilised according to the manufacturer's instructions. The total IgG in column buffer (0.02 M sodium phosphate, pH 7.0) was applied to the R0 column at a flow rate of 1.0 mL/min. The column was washed extensively with column buffer. The bound GLURP-specific IgG was eluted with 0.1 glycine/HCl, pH 2.7 and collected over 1 M Tris-HCl, pH 9.0, to neutralise the pH at the same flow rate. Soon after, the eluate was dialysed against PBS and then Roswell Park Memorial Institute (RPMI) 1640 medium and concentrated using an Ultrafree Cl centrifugal filter device (Millipore). The GLURP-specific IgG fraction was filtered through a 0.22 µm Millex filter (Millipore) and the levels were quantified using the Bicinchoninic Acid Protein Assay kit (BCA, Sigma) with bovine serum albumin (BSA) as a standard. Indirect immunofluorescence assays (IFAs) - IFAs were performed to verify if the purified anti-R0 antibodies recognised the native protein. IFA slides were prepared with synchronous cultures of P. falciparum schizonts (strain PSS1) using the method described by Trager and Jensen (1976). IFAs were performed at 37ºC in moist chambers after a 10-min fixation in cold acetone (-20ºC). After incubation with purified antibodies (2-factor dilution from 1:40-1:5120), bound antibodies were detected by reaction with appropriate fluorescein isothiocyanate-conjugated antisera (Sigma). Parasite culture - The P. falciparum line PSS1 (Brazil) was cultured according to a modification of the method described by Trager and Jensen (1976) with serum-free medium. Briefly, parasites were cultured in vitro with freshly prepared blood bank-derived O+ erythrocytes in RPMI 1640 (Sigma) supplemented with 25 mM HEPES buffer, 23 mM NaHCO3 (Sigma), 40 µg/L gentamicin, 4 g/L glycose (Sigma), 0.18 mM hypoxanthine (Sigma) and 10% albumax (Gibco), in an atmosphere containing 5% O2, 5% CO2 and 90% N2 (White Martins, RJ, Brazil). The parasites were synchronised by repeated sorbitol treatments and schizonts were enriched by flotation on plasmagel, as described elsewhere (Lambros & Vanderberg 1979, Reese et al. 1979). Monocyte preparation - Monocytes were obtained from freshly drawn heparinised peripheral blood from a single Brazilian donor without previous exposure to malaria. Peripheral blood mononuclear cells (PBMC) were isolated by density gradient centrifugation (Ficoll-Hypaque). The cells obtained were washed three times in serum-free RPMI 1640 medium and resuspended in RPMI 1640 with 10% albumax (Gibco) at 2 x 107 mL. The PBMC were distributed in 96-well flat-bottomed microdilution plates at 2 x 106 cells/well and cultured at 37ºC in 5% CO2 for 2 h and washed with RPMI 1640 (Sigma). This method allows the recovery of about 2 x 105 cells, which are mostly monocytes (Theisen et al. 2004). For assays in which activated monocytes were used, cells were pretreated for 24 h with recombinant human interferon gamma (IFN-γ) (BD Bioscience) at a final concentration of 100 ng/mL in RPMI 1640 containing 10% albumax. Monocytes were then washed with serum-free RPMI 1640 before use in the ADCI assay. Growth inhibition (GI) and ADCI assays - GI and ADCI assays, in the absence or presence of monocytes, respectively, were performed in parallel in triplicate wells of 96-well flat-bottom culture plates (Falcon). For the GI assay, 50 µL volumes of anti-R0 purified antibodies, at the final concentrations of 50, 150 and 450 µg/mL in RMPI containing 10% albumax, were added to 50 µL of synchronised P. falciparum cultures at the schizont stage at an initial parasitemia of 0.5% and with 5% hematocrit. In the ADCI assay, 50 µL of P. falciparum synchronised cultures at the schizont stage at an initial parasitemia of 0.5% and with 5% hematocrit and 50 µL of anti-R0 purified antibodies at final concentrations of 50, 150 and 450 µg/mL in RMPI with 10% albumax were added to wells containing the adhered monocytes. The experimental controls comprised the following: (i) P. falciparum synchronised cultures at the schizont stage alone, (ii) P. falciparum synchronised cultures at the schi-zont stage with monocytes, (iii) P. falciparum synchronised cultures at the schizont stage with IgG purified from non-endemic control serum, (iv) P. falciparum synchronised cultures at the schizont stage with IgG purified from NCS and monocytes, (v) P. falciparum synchronised cultures at the schizont stage with IgG purified from pooled hyperimmune serum and (vi) P. falciparum synchronised cultures at the schizont stage with IgG purified from pooled hyperimmune serum and monocytes. The plates were maintained at 37ºC in a 5% CO2 for 72 h and, at intervals of 24 h, 50 µL volumes of RPMI with 10% albumax containing the anti-R0 antibodies or IgG from NCS and PIAG at the same concentrations (50, 150 or 450 µg/mL) were added to each well. At the end of the 72 h, the cell culture supernatants from each well were collected individually and stored at -70ºC for later determination of tumour necrosis factor alpha (TNF-α). The mean of parasitemia determined in each series of triplicate wells was calculated in both GI and ADCI assays by microscopic examination and flow cytometry. The specific growth inhibitory index (SGI), which takes into account the possible inhibition induced by antibodies alone (GI) or by antibodies and monocytes (ADCI) was independently calculated as follow: SGI = 100 x [1 - (% parasitemia in the test sample/% parasitemia in the control sample)]. Parasitemia - The parasitemia in each triplicate well was evaluated by flow cytometry using rhodamine 123, a cationic, lipophilic fluorochrome that is incorporated into the mitochondria of viable parasites (Totino et al. 2008). After 72 h of culture, the parasitized erythrocytes were washed in RPMI medium (RPMI-1640, 25 mM HEPES, 0.2% glucose, 23 mM sodium bicarbonate), centrifuged at 350 g for 5 min and resuspended and incubated at 37ºC for 5 min in 50 volumes of 1 µg/mL rhodamine in RPMI. The rhodamine solution was removed by centrifugation (350 g, 5 min) and the parasitized erythrocytes were washed in RPMI and incubated at 37ºC for 30 min in 100 volumes of complete medium. After incubation, the parasitized erythrocytes were resuspended in fresh complete medium and analysed in a flow cytometer (FACSCalibur, Becton Dickinson). To discriminate parasitized (viable parasites) from non-parasitized erythrocytes (no parasite or dead parasites) in the culture samples, non-infected erythrocytes stained with rhodamine 123 were used as negative controls in the flow cytometry analysis (Fig. 1). ELISA for determination of TNF-α levels in culture supernatants - TNF-α was measured using commercial ELISA kits (BD Biosciences). Briefly, enzyme-linked immunosorbent assay 96-well plates (Maxisorp, NUNC, Denmark) were coated overnight at 4ºC with 2 µg/mL of capture antibody in a volume of 100 µL/well in 0.1 M carbonate-bicarbonate buffer, pH 8.2. After washing with PBS-T20, pH 7.4, uncoated sites were blocked for 2 h at RT with 200 µL/well of 0.1% (wt/vol) BSA (Sigma) in PBS with 0.05% sodium azide (Sigma) (PBS/BSA/NaN3). After washing with PBS, the plates were incubated with 100 µL/well of cell culture supernatant or 100 µL/well of recombinant cytokines diluted successively to determine the standard curve. After washing with PBS-T20, the plates were incubated for 1 h at RT with 100 µL/well of 200 ng/mL biotinylated detection anti-body. After washing with PBS-T20, 100 µL of a solution of streptavidin-peroxidase (Sigma) diluted 1:500 in PBS/BSA/NaN3 was added to each well and incubated for 30 min at RT in the dark. The reaction was visualised with 100 mL/well of 2,2'-azino-bis(3-ethylbenzthiazoline-6-sulphonic acid) (Sigma) containing 10 µL of 30% H2O2 for 30 min and 50 µL/well of 20% sodium dodecyl sulfate (Sigma) was used to stop the reaction. Plates were read at 405 nm in a spectrophotometer (Spectramax 250, Molecular Devices). The TNF-α OD values were converted to concentration values (ng/mL) using sigmoidal curve-fit equations derived from the standard curve generated using recombinant TNF-α. Statistical analysis - The data were stored in the Fox-plus® (Borland International, Inc Perrysburg, OH) data bank software. The Statistica (Microsoft, Inc Redmond, WA) and Epi-Info 6 (Centres for Disease Control and Prevention, Atlanta, GA) statistical software programs were used for data analysis. The Student's t-test was used to analyse the differences in mean values; the Chi-square test was used to analyse the difference in prevalence of the positive responses and the Spearman rank coefficient test was used to analyse the correlations between variables. Results Natural infections with P. falciparum induced high levels of IgG antibodies against the GLURP-R0 region in most naturally exposed individuals from RO analysed in this study (Table I). The levels of anti-GLURP-R0 IgG antibodies were positively correlated with age (p = 0.03, r = 0.7167) and with the time of residence in malaria-endemic areas (p = 0.04, r = 0.7000). No association between the anti-R0 IgG antibody response and the reported number of previous malaria episodes was observed. There was a predominance of IgG1 R0-specific antibodies over IgG2, IgG3 and IgG4 (p = 0.01, IgG1 vs. IgG2; p = 0.02, IgG1 vs. IgG3; p = 0.002, IgG1 vs. IgG4). No associations between age, time of residence in malaria endemic areas or the number of previous malaria infections and the levels of anti-R0 IgG subclasses could be detected (Table I). IgG antibodies were affinity-purified against GLURP-R0 from the nine Brazilian individuals and from a pool of serum from hyperimmune African adults (PIAG). All 10 of the anti-R0 IgG preparations recognised the natural parasite protein by IFAs (Fig. 2). As expected, IgG purified from two blood donors that were never exposed to malaria (NCS) did not react with the parasite. The anti-R0 IgG antibodies purified from Brazilian donors strongly inhibited the growth of P. falciparum in vitro independently of the presence of monocytes. Indeed, eight of nine (89%) samples exhibited a parasite GI of more than 50% at a concentration of 50 µg/mL. Interestingly, this inhibitory activity tended to decrease with increasing antibody concentration. The samples R006, R007, R008 and R009 inhibited parasite growth to the same extent as the anti-R0 IgG antibodies purified from PIAG, especially in the absence of monocytes (Table II). A higher level of GI was observed as compared to ADCI at a concentration of 50 µg/mL IgG (p = 0.03) (Fig. 3). In the presence of monocytes, there was an inverse relationship between the ADCI activity and the concentration of anti-R0 affinity-purified IgG in the assay. The mean parasitemia at the concentrations of 50 µg/mL and 150 µg/mL was lower than the mean at the 450 µg/mL concentration (p = 0.007; 50 µg/mL vs. 450 µg/mL; p = 0.008; 150 µg/mL vs. 450 µg/mL) (Table II). Interestingly, higher levels of TNF-α in the supernatant were observed in the ADCI test performed in the presence of monocytes at a concentration of 450 µg/mL of purified anti-R0 (p = 0.01; 50 µg/mL vs. 450 µg/mL; p = 0.003; 150 µg/mL vs. 450 µg/mL) (Fig. 4). In parallel, we performed P. falciparum in vitro culture in the presence of 10, 5, 2.5 or 1.25 ng/mL of recombinant TNF-α. Independently of the TNF-α concentration, no difference in the mean parasitemia was observed (mean of 3.3 ± 0.3 without TNF-α, 3.4 ± 0.2 at 10 ng/mL of TNF-α 3.3 ± 0.1 at 5 ng/mL of TNF-α 3.5 ± 0.2 at 2.5 ng/mL of TNF-α and 3.4 ± 0.5 at 1.25 ng/mL of TNF-α, p > 0.05). Discussion Several studies have shown that antibodies, especially cytophilic antibodies, may have an important role in the development of antimalarial immunity. Malaria-associated clinical and anti-parasite immunity, known as premunition, is not sterilising, is strain-independent, requires many years of continuous challenges and is short-lived (Bouharoun-Tayoun & Druilhe 1992, Luty et al. 1994, Bouharoun-Tayoun et al. 1995, Aribot et al. 1996, Shi et al. 1996, Sarthou et al. 1997, Taylor et al. 1998, Oeuvray et al. 2000, Ndungu et al. 2002). Although antibodies can act directly by inhibiting merozoite invasion and preventing the schizont rupture (Bolad & Berzins 2000), cytophilic antibodies can also act in cooperation with monocytes to contain the proliferation of parasites, using a mechanism called ADCI. Based on the considerations that (i) GLURP is an antigen target for antibodies involved in ADCI (Theisen et al. 1998, 2000, Oeuvray et al. 2000, Hermsen et al. 2007) and (ii) that anti-R0 antibodies showed a more potent effect than anti-R2 antibodies (Theisen et al. 1998), we evaluated the role of anti-R0 antibodies purified from individuals living in RO in inhibiting, both directly and in cooperation with monocytes, the in vitro growth of P. falciparum. The potential importance of GLURP in immunity to malaria has been demonstrated in the present study by the fact that antibodies against the R0 region were able to promote a potent inhibition of parasite growth in vitro. This finding suggests that whatever the native conformation and the schizont/merozoite distribution of GLURP, the R0 region is accessible to antibodies at some critical point during parasite development. Our results showed that anti-R0 IgG antibodies purified from individuals living in RO, a Brazilian endemic area with low levels of transmission, were able to promote a strong inhibition of P. falciparum growth at 50 µg/mL and that, curiously, there was a tendency towards reduced frequency of GI with increasing concentration of antibodies. These results were independent of the presence of monocytes. Our findings are different from those reported by Theisen et al. (1998), who observed that anti-R0 antibodies purified from eight adults immune to malaria living in Liberia had no direct effect, but promoted a strong inhibition of P. falciparum growth in cooperation with monocytes in ADCI. Furthermore, studies have also reported that antibodies directed to other P. falciparum antigens, such as P126 and MSP-3, have little or no direct effect on the growth of P. falciparum in vitro and can only inhibit the parasite growth in cooperation with monocytes (Bouharoun-Tayoun et al. 1990, 1995, Oeuvray et al. 1994). A limitation in our ADCI assay was the use of a single monocyte donor for the experiments. Both the source of the monocytes and the existence of different subpopulations can affect the outcome of ADCI assays. Shi et al. (1999) have shown that monocytes from different donors or from the same donor collected at different times, exhibited wide variation in inhibiting parasite growth in ADCI assays. More recently, Chimma et al. (2009) have shown that monocytes from healthy individuals differed in their ADCI effect depending on whether the donor was exposed or not to malarial infection. In addition, monocyte subsets defined by the expression of CD14 and CD16 presented different inhibitory activities against P. falciparum, with CD14hiCD16+ monocytes showing greater activity than the classical CD14hiCD16- phenotype (Chimma et al. 2009). Therefore, the use of a single donor in our study does not allow us to take into account the variations in the intrinsic ability of monocytes to inhibit parasite growth. Our data suggest that anti-R0 antibodies purified from individuals living in RO are able to directly inhibit the in vitro growth of P. falciparum. We could argue that the direct effect of GLURP antibodies on inhibiting parasite growth could be due to the neutralisation of free merozoites and, consequently, inhibiting the merozoite invasion of erythrocytes (Perkins 1991). One could also hypothesise that these antibodies could access the parasite inside the red blood cells just before merozoite release, thus interfering with dispersion, because the erythrocyte membrane undergoes extensive morphological, structural and functional changes during Plasmodium infection, leading to changes in permeability (Lyon et al. 1989). Moreover, it has been demonstrated that intracellular P. falciparum parasites can capture fluorescent macromolecules through the parasitophorous duct, which would be permeable to IgG molecules (Pouvelle et al. 1991, Pouvelle & Gysin 1997). In fact, Jensen et al. (1982) have demonstrated that incubation of P. falciparum infected-erythrocytes with sera from immune humans caused the appearance of "crisis forms", i.e., intracellular degeneration of the parasite. Thus, the antibodies could also act by inhibiting intracellular schizogony. The observation in this study of a direct inhibitory effect (in the absence of monocytes) does not exclude the possibility that the ADCI phenomenon exists and may effectively operate in vivo. There is a limited knowledge about how growth-inhibitory antibodies are acquired, and it is unclear whether these antibodies can be acquired quickly after a limited exposure or if repeated exposure over an extended period is required (McCallum et al. 2008). In this study, we demonstrate that inhibitory antibodies can be quickly acquired after a limited number of previous malaria infections because four out of the nine studied individuals reported up to five episodes of malaria. Our data show a significant decrease in the frequency of GI with increasing antibody concentration. Previous studies using anti-GLURP and anti-MSP3 antibodies have shown a dose-related ADCI effect up to a certain IgG concentration, followed by a decline in the ADCI effect at increasing IgG concentrations (Theisen et al. 2001). This observation may be due the fact that in the ADCI assay, bridging of a monocyte and a merozoite by a specific antibody recognising a surface structure on the merozoite leads to secretion of soluble factors by the monocyte that mediate parasite killing in vitro. At low antibody concentrations, the ADCI effect is weak due to the low number of activated monocytes. At increasing IgG concentrations, there will be an increasing ADCI-effect, which persists up to an optimal ratio between the antigen and antibody. At very high IgG concentrations, competition can occur between specific IgG antibodies bound to the Fcγ receptors on the monocytes and soluble specific IgG antibodies for the binding to surface epitopes on the merozoite; this would lead to a relatively lower number of activated monocytes and, consequently, a lower ADCI effect. These data suggest that the optimal anti-parasite activity will occur within a limited range of antibody concentration and therefore either a lack or excess of antibody could decrease the effectiveness of the response. If this effect observed in vitro is also true in vivo, it may raise additional concerns for vaccine development. Since the experiments performed by Clark et al. (1990), demonstrating the participation of TNF-α in the death of intracellular parasites, many researchers have attempted to evaluate the possible antiplasmodial role of this cytokine. Studies performed by Stevenson et al. (1990, 1995) have demonstrated that protection against infection by Plasmodium chabaudi depends on the production of IFN-γ and TNF-α. Another study showed that repeated injections of TNF-α in mice infected with Plasmodium yoelii reduced parasitemia and prolonged the survival of mice infected with a lethal strain of the parasite (Taverne et al. 1987). Bouharoun-Tayoun et al. (1995) have demonstrated that one of the consequences of monocyte activation in ADCI is the release of parasitostatic factors, including TNF-α. Considering this, we verified whether the levels of this cytokine produced by monocytes in the presence of anti-R0 antibodies could be related to the degree of inhibition of in vitro growth of P. falciparum in ADCI. Interestingly, the highest levels of TNF-α were observed in wells containing 450 µg/mL of anti-R0 purified, which were exhibited lower inhibition of parasite growth, suggesting that TNF-α had no effect or even stimulated, parasite growth. To test this hypothesis, we added recombinant TNF-α to the P. falciparum cultures at concentrations of 10, 5, 2.5, and 1.25 ng/mL and compared the results with the results obtained with cultures without recombinant TNF-α. We did not observe an inhibition of parasite growth at any of the concentrations of TNF-α. These results corroborate previous studies showing that incubation of erythrocytes parasitized with P. yoelii with high concentrations of TNF-α does not affect infectivity (Taverne et al. 1987) and that the addition of TNF-α to co-culture of monocytes and erythrocytes parasitized by P. falciparum has no effect on parasite growth (Hviid et al. 1988, Muniz-Junqueira et al. 2001). However, if lymphocytes are added to this co-culture, a decrease in the P. falciparum growth has been reported, suggesting that TNF-α has a pleiotropic effect and that the protective effect of TNF-α depends on the interaction between different factors, such as monocytes, lymphocytes, antibodies and other cells and molecules (Muniz-Junqueira et al. 2001). In conclusion, our data suggest that the antibody response induced by the R0 region of the GLURP protein in naturally exposed individuals in the Brazilian population may have an important role in controlling parasitemia because these antibodies were able to inhibit the in vitro growth of P. falciparum, regardless the presence of monocytes. Furthermore, our results indicate that TNF-α has no apparent direct effect on the in vitro growth of P. falciparum. References
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc11138f3.jpg] [oc11138t2.jpg] [oc11138f4.jpg] [oc11138t1.jpg] [oc11138f1.jpg] [oc11138f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}