
|
Memórias do Instituto Oswaldo Cruz
Fundação Oswaldo Cruz, Fiocruz
ISSN: 1678-8060 EISSN: 1678-8060
Vol. 106, Num. s1, 2011, pp. 52-63
|
Memórias do Instituto Oswaldo Cruz, Vol. 106, Special Issue, pp. 52-63
Original Article
Thrombocytopenia
in malaria: who cares?
Marcus Vinícius
Guimarães LacerdaI, II, I, +; Maria Paula
Gomes MourãoI, II, III; Helena Cristina Cardoso CoelhoII;
João Barberino SantosIV
IFundação
de Medicina Tropical Dr. Heitor Vieira Dourado, Av. Pedro Teixeira 25, 69040-000
Manaus, AM, Brasil
IIUniversidade do Estado do Amazonas, Manaus, AM, Brasil
IIIUniversidade Nilton Lins, Manaus, AM, Brasil
IVUniversidade de Brasília, Brasília, DF, Brasil
+ Corresponding author: marcuslacerda.br@gmail.com
Received 1 April
2011
Accepted 26 May 2011
Abstract
Despite not being
a criterion for severe malaria, thrombocytopenia is one of the most common complications
of both Plasmodium vivax and Plasmodium falciparum malaria. In
a systematic review of the literature, platelet counts under 150,000/mm3
ranged from 24-94% in patients with acute malaria and this frequency was not
different between the two major species that affected humans. Minor bleeding
is mentioned in case reports of patients with P. vivax infection and
may be explained by medullary compensation with the release of mega platelets
in the peripheral circulation by megakaryocytes, thus maintaining a good primary
haemostasis. The speculated mechanisms leading to thrombocytopenia are: coagulation
disturbances, splenomegaly, bone marrow alterations, antibody-mediated platelet
destruction, oxidative stress and the role of platelets as cofactors in triggering
severe malaria. Data from experimental models are presented and, despite not
being rare, there is no clear recommendation on the adequate management of this
haematological complication. In most cases, a conservative approach is adopted
and platelet counts usually revert to normal ranges a few days after efficacious
antimalarial treatment. More studies are needed to specifically clarify if thrombocytopenia
is the cause or consequence of the clinical disease spectrum.
Key words:
Plasmodium falciparum - Plasmodium vivax - malaria - thrombocytopenia
- platelets
Malaria affects
almost all blood components and is a true haematological infectious disease.
Anaemia and thrombocytopenia are the most frequent malaria-associated haematological
complications (Wickramasinghe & Abdalla 2000) and have received more attention
in the scientific literature due to their associated mortality. On the other
hand, thrombocytopenia is less studied, causes negligible mortality and is an
isolated phenomenon; there is no report of a single patient in the literature
who has died only because of malaria-associated thrombocytopenia.
In the current
field of Travel Medicine, the rapid increase in the number of people travelling
to tropical areas has added a great challenge for malaria diagnosis because
the thick blood smear (the standard diagnosis in endemic areas) has high specificity
but only when performed by experienced microscopists. The presence of thrombocytopenia
in acute febrile travellers returning from tropical areas has become a highly
sensitive clinical marker for malaria diagnosis (D'Acremont et al. 2002). Another
study has reported 60% sensitivity and 88% specificity of thrombocytopenia for
malaria diagnosis in acute febrile patients (Lathia & Joshi 2004). The sensitivity
of thrombocytopenia together with the acute febrile syndrome was 100% for malaria
diagnosis, with a specificity of 70%, a positive predictive value of 86% and
a negative predictive value of 100% (Patel et al. 2004).
Thrombocytopenia
is a well-documented and frequent complication in Plasmodium vivax malaria.
In one study, platelet count normalised after treatment and only one patient,
concomitant with the lowest platelet count, exhibited "purpuric lesions" on
the lower extremities (Hill et al. 1964).
Since the beginning
of the 1970s, there have been reports proposing that malaria-associated thrombocytopenia
is quite similar in P. vivax and Plasmodium falciparum infections
(Beale et al. 1972). However, more recent data in India has shown how thrombocytopenia
exhibited a heightened frequency and severity among patients with P. vivax
infection (Kochar et al. 2010).
In 1903, the young
physician Carlos Chagas (who become more famous afterwards for the discovery
of American trypanosomiasis, which is named after him), published his MD thesis
on the Hematological Studies on Paludism (Chagas 1903). Within it, he described
anaemia and leukocyte abnormalities, but also normal megakaryocytes in the bone
marrow were referred to in patients with acute and chronic malaria from Rio
de Janeiro. He also drew our attention to evidence of bleeding in the 46 patients
he followed.
In the city of
Manaus, state of Amazonas, located in the Western Brazilian Amazon, Djalma Batista
authored Paludism in the Amazon, a book in which he described observations about
patients with malaria seen at his private clinics (Batista 1946). Similar to
Carlos Chagas, there is no mention of platelet count in his study because it
was not routinely performed. However, there is a vivid description of haemostasis
disorders in some patients. Particularly noteworthy is the presence of huge
spleen enlargement and prolonged bleeding time accompanied by recurrent gingival
bleeding.
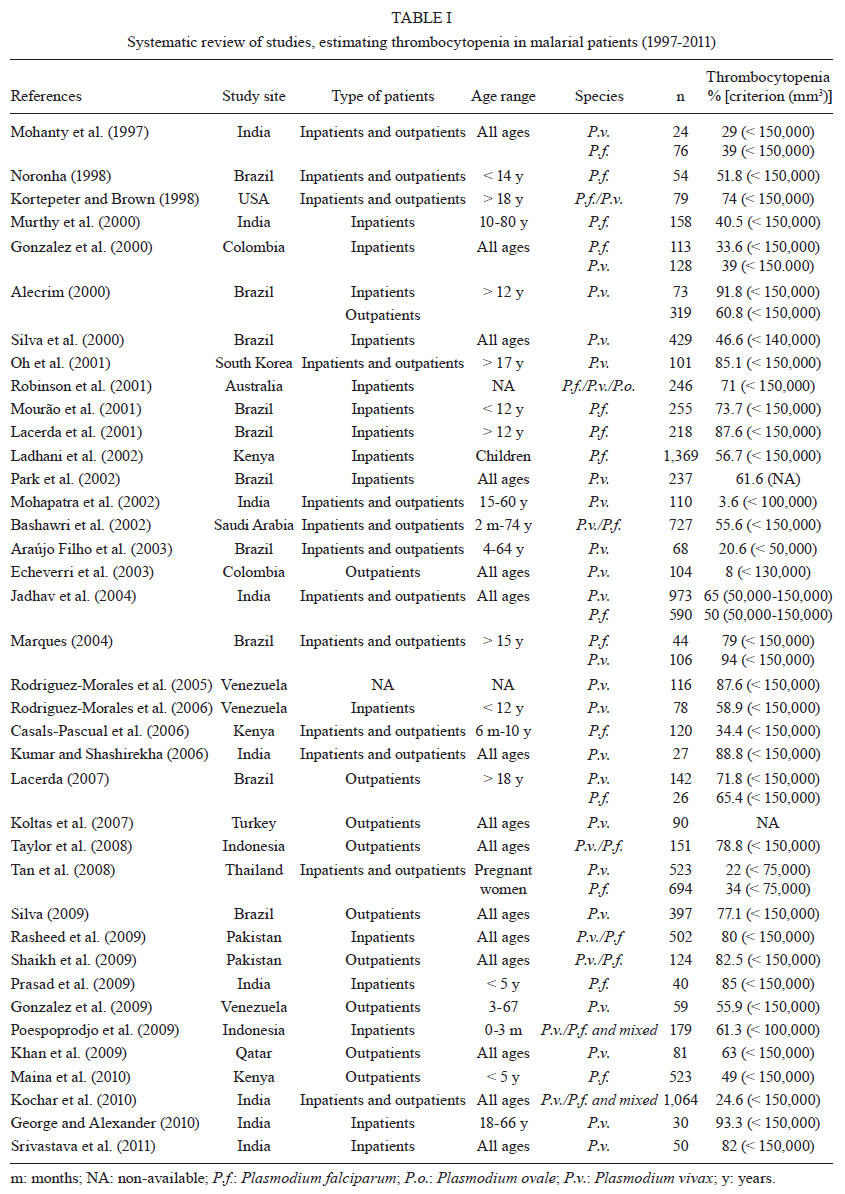
Data on the real
burden of thrombocytopenia associated with malaria is contradictory in the literature
and it is not usually considered when conducting patient selection. Table
I shows the major publications estimating the frequency of thrombocytopenia.
Most of these data were published in the late 1990s, probably in time with the
surge in the availability of affordable automated machines capable of performing
full blood counts (FBC). Manual platelet counting is time-consuming and usually
needs to be requested by the physician with the routine blood count in most
of the endemic areas for malaria. In only three publications is there an adequate
randomised enrollment of patients with appropriate sample size calculation to
estimate the frequency of bleeding and its association with the respective platelet
count (Lacerda 2007, Silva 2009, Kochar et al. 2010). Only one study has ruled
out other common causes of thrombocytopenia that are also endemic in the studied
area (Lacerda 2007). There is a wide range of thrombocytopenia occurrence in
these reports, which may be explained by distinct selection criteria of the
enrolled patients. There are also differences in the selection of outpatients
or inpatients from tertiary care centres that tend to present with severe thrombocytopenia.
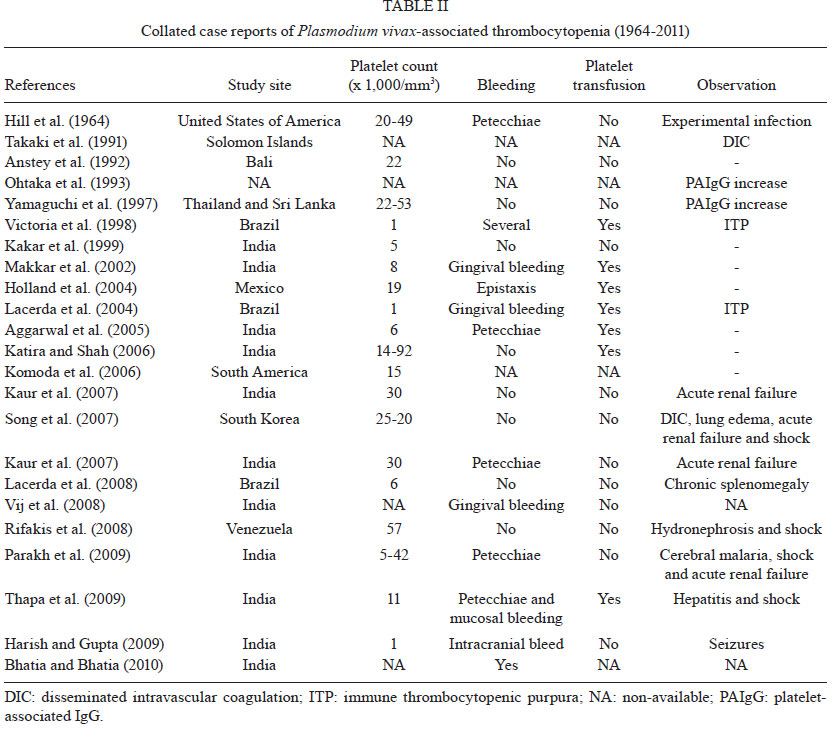
Furthermore, clinical manifestations of thrombocytopenia are usually described
as case reports and most of these are due to P. vivax (Table
II).
In 2005, 138 of
684 (20.1%) malarial cases hospitalised in a tertiary care centre in Manaus
had thrombocytopenia as the cause of admission, which corresponded to 6.8% of
hospitalisations due to all causes in this reference institution (unpublished
observations). Hospitalisation, however, does not add any benefit to the patient
and because there is no evidence for any intervention, this simply increases
public health costs in underdeveloped and under-resourced areas.
Pathogenesis
of malarial thrombocytopenia - Coagulation disturbances - A study
based on 31 American soldiers in Vietnam with chloroquine-resistant falciparum
malaria noted the following changes in the acute phase of the disease using
the same patients as their own controls during convalescence: decrease in the
platelet count and prothrombim activation time, increase in the activated thromboplastin
time, and reduction in factors V, VII and VIII with normal fibrinogen (Dennis
et al. 1967). This report suggested that thrombocytopenia was simply a consequence
of the coagulation disorders presented by these patients, an idea that persisted
for many decades in the literature. In another series of 21 patients with falciparum
malaria, six had developed disseminated intravascular coagulation (DIC). The
authors noted that the patients with more severe thrombocytopenia also had DIC
and that there was correlation between platelet count and C3 protein levels.
However, the reduction in C3 was proportional to that in parasitaemia, suggesting
that thrombocytopenia was not independently associated with C3 (Srichaikul et
al. 1975). In Manaus, 2004, a study with falciparum and vivax patients demonstrated
a negative correlation between platelet counts, thrombin-anti-thrombin complex
and D-dimers, suggesting that the activation of coagulation could be partially
responsible for thrombocytopenia (Marques et al. 2005).
Splenomegaly
- The spleen in malaria has played a crucial role in the immune response against
the parasite, as well as controlling parasitaemia due to the phagocytosis of
parasitised red blood cells (RBCs) (Engwerda et al. 2005). Some data suggested
that platelets were sequestered in the spleen during the acute infection (Skudowitz
et al. 1973). In the experimental model with Plasmodium chabaudi, thrombocytopenia
was absent in splenectomised mice, showing that the spleen was essential for
thrombocytopenia (Watier et al. 1992). The term hypersplenism was proposed to
describe the clinical picture of the enlarged spleen followed by the decrease
in one or more peripheral blood lineages (usually reverted after splenectomy),
probably due to sequestration or destruction of cells inside the spleen, in
liver diseases, which lead to increased portal system pressure. However, it
is recently believed that not only mechanical alterations take place, but also
compromise of haematopoietic growth factors produced in the liver (Peck-Radosavljevic
2001). On the other hand, the isolated spleen enlargement does not explain per
se the destruction of cells as formerly believed. This organ represents
outstanding architectural organisation and controls, with great sophistication,
the exposure of cells screened by it. In patients with malaria, the increase
in the macrophage-colony stimulating factor is associated to thrombocytopenia,
suggesting that macrophages play a role in the destruction of these particles
(Lee et al. 1997). In the comparison of spleens from patients with severe falciparum
malaria vs. those of control and septic patients, it was shown that splenic
dendritic cells are increased in malaria and there is a reduction in B lymphocytes
and macrophages in the splenic cords (Urban et al. 2005). The mechanisms related
to the formation of splenic hematomas are mostly associated with P. vivax
infection and the interface with thrombocytopenia is noted to be imprecise (Lacerda
et al. 2007). In vivax malaria, the role of the spleen in the expression of
vir genes is still unrecognised. P. vivax passing through the
spleen would activate the transcription of polymorphic Vir proteins to escape
from macrophage destruction in this organ. On the other hand, these same proteins
would permit the binding of parasitised RBCs to barrier cells, creating an isolated
microenvironment in the spleen that would be rich in reticulocytes (del Portillo
et al. 2004). More recent studies with the murine model of Plasmodium yoelii
evidenced that there was higher parasite accumulation, reduced motility, loss
of directionality, increased residence time and altered magnetic resonance only
in the spleens of mice infected with the non-lethal 17X strain (Martin-Jaular
et al. 2011). This same model has never been used to study the role of the spleen
in thrombocytopenia, but opens new avenues for functional and structural studies
of this lymphoid organ.
Bone marrow
alterations - The finding of a P. vivax trophozoite inside a human
platelet suggested that thrombocytopenia could be the result of invasion of
these particles by the parasites themselves, similar to what was classically
proposed for RBCs. As these same authors did not find parasites inside megakaryocytes,
they proposed that the penetration took place in the peripheral circulation
(Fajardo & Tallent 1974). However, this observation was never seen again
in the literature. Likewise, a "dysmegakaryopoiesis" was proposed, similar to
what happened in the human malarial anaemia model, where dyserythropoiesis was
triggered by cytokines (Menendez et al. 2000). In the few studies that examined
the bone marrow for this purpose, megakaryocytic lineage was apparently preserved
(Naveira 1970, Beale et al. 1972). Thrombopoietin indeed seems to rise during
the acute disease even in the presence of liver compromise, suggesting that
no bone marrow inhibition is seen (Kreil et al. 2000). Additional data from
FBC samples in vivax patients showed that there is a significant negative correlation
between platelet count and mean platelet volume (Lacerda 2007), suggesting that
megakaryocytes are able to release mega platelets in the circulation to compensate
for the low absolute number of platelets in the periphery. Similar results were
shown in children with falciparum malaria (Maina et al. 2010). These mega platelets
are probably able to sustain a good primary haemostasis that could explain the
low frequency of severe bleeding in malarial patients, as shown in Table
II. Non-human primates, on the other hand, are an unexplored model to study
megakaryopoiesis alterations and its implication on thrombocytopenia (Llanos
et al. 2006).
Antibody-mediated
platelet destruction - There is evidence that platelet-associated IgG (PAIgG)
is increased in malaria and is associated with thrombocytopenia. However, this
is a generic definition for all types of IgGs that may be found on the platelet
surface, including antibodies stored inside platelet α-granules.
Therefore, increased PAIgG could also be interpreted as platelet activation
and exposition of IgGs on the surface, and not necessarily auto-immunity, as
suggested in anecdotal case reports where antibodies against glycoproteins were
detected in malaria (Panasiuk 2001, Conte et al. 2003). The detection of auto-antibodies
against platelets by flow cytometry (Rios-Orrego et al. 2005) should not be
seen as specific for malaria, as natural auto-antibody formation is a common
defence of the infected organism and is frequently seen in most viral, bacterial
and parasitic diseases without any repercussion (Daniel-Ribeiro & Zanini
2000). Molecular mimicry, however, provides evolutionary advantage for microorganisms
that escape immune aggression (Daniel-Ribeiro 2000). The relationship between
malaria and auto-immunity has been discussed in the literature and the first
epidemiological association was made based on the presence of fewer auto-immune
diseases in malarigenous areas (Greenwood 1968). The formation of circulating
immune complexes (CIC) in vivo in malaria, as well as in other infectious diseases,
is a continuous process from antigens and antibodies and/or complement elements.
CIC seems to modulate the immune response to several antigens that remain sequestered
in B lymphocyte or dendritic cell-rich follicles for a longer time, which contributes
to the formation of B-cell immunological memory, as seen in vaccine studies
(Davidson 1985). During acute malaria, thrombocytopenia is most probably associated
with the binding of parasite antigens to the surface of platelets to which antimalarial
antibodies also bind, leading to the in situ formation of immune complexes
(ICs) (Kelton et al. 1983). In an experimental model with Plasmodium berghei,
the same correlation between platelet count and IC's was evidenced (Grau et
al. 1988). No association was found with IgM (Beale et al. 1972). It is clear
that CICs are elevated in vivax and falciparum malaria, but their role in the
development of thrombocytopenia is still obscure (Touze et al. 1990, Tyagi &
Biswas 1999) as well as its immune suppressing effect (Brown & Kreier 1982,
Shear 1984). Because the generation of IC's is proportional to the amount of
available antigen, the negative correlation between platelet count and peripheral
parasitaemia reported in many studies (Lacerda 2007, Silva 2009) corroborates
ICs as a potential mechanism of platelet destruction. The presence of amino
acid residues tyrosine 193 [9Y(193)] and serine 210 [S(210)]
on apical membrane antigen-1 (AMA-1) was significantly associated with normal
platelet counts in P. vivax malaria independent of the level of parasitaemia
that also provides supporting evidence for this (Grynberg et al. 2007). In only
one study, circulating monocytes were found to phagocytose platelets, but this
mechanism still needs to be associated to thrombocytopenia more closely (Jaff
et al. 1985). The finding of immune thrombocytopenic purpura (ITP) secondary
to malarial infection is rare and may be due to idiosyncratic auto-immune mechanisms
not well understood (Lacerda et al. 2004).
Oxidative stress
- Free radicals may play an important role in the platelet destruction in malarial
infection. There is evidence that the decrease in total cholesterol in vivax
malaria is due to lipidic peroxidation (Erel et al. 1998). Also, in vivax malaria,
there is a negative correlation between platelet count and platelet lipid peroxidation
in addition to the positive correlation between platelet count and the activity
of gluthatione peroxidase and superoxide dismutase, which are considered anti-oxidant
enzymes (Erel et al. 2001). In a study of 103 patients with acute falciparum
malaria, there was a negative correlation between platelet count and nitrogen
reactive intermediates (Santos 2000). There is also a strong association between
platelet count and intra-platelet gluthatione peroxidase, suggesting that a
compensatory mechanism is presented by platelets to face the oxidative burst
found in malaria (Araujo et al. 2008).
Platelet aggregation
- Platelets from patients with acute malaria are highly sensitive to adenosine
diphosphate (ADP) addition in vitro (Essien & Ebhota 1981), and it is believed
that ADP release following haemolysis could contribute to higher platelet aggregation.
Actually, the incubation of platelets with P. falciparum-parasitised
RBCs also increases platelet aggregation per se in vitro, especially
after ADP and thromboxane A2 addition (Inyang et al. 1987). Even
electron microscopic examination of non-stimulated, fresh platelets from malarial
patients show centralisation of dense granules, glycogen depletion and microaggregates
and phylopoids as a sign of in vivo activation, which could be responsible for
a pseudo-thrombocytopenia due to sequestration of these activated particles
in the interior of the vessels (Mohanty et al. 1988). Contradictory data were
presented showing aggregation impairment in severe falciparum patients after
ADP addition in vitro (Srichaikul et al. 1988). P. falciparum induces
systemic acute endothelial cell activation and the release of activated von
Willerbrand factor (vWF) immediately after the onset of the blood-stage infection
(Mast et al. 2007). Even without consumptive coagulopathy, the increase in soluble
glycoprotein-1b (GP1b) concentrations results from vWF-mediated GP1b shedding,
a process that may prevent excessive adhesion of platelets and parasitised erythrocytes
(Mast et al. 2010). Antimalarial drugs have also been shown as potential inhibitors
of platelet aggregation in vivo and in vitro, what precludes careful inclusion
and exclusion criteria of patients to be used in clinical research (Cummins
et al. 1990).
The relationship
between thrombocytopenia and severe malaria - Severe thrombocytopenia (platelet
count under 50,000/mm3), despite not being considered severe malaria
according to World Health Organization criteria (WHO 2010) due to the inability
to cause death per se, has been occasionally associated with severity
(Gerardin et al. 2002, Rogier et al. 2004) or not (Moulin et al. 2003). But
thrombocytopenia has also been described in severe vivax patients (Kochar et
al. 2005, Andrade et al. 2010). In 17 patients from Manaus affected by any of
the WHO malaria severity criteria with confirmed P. vivax monoinfection,
14 presented with thrombocytopenia, suggesting that this haematological complication
can be explored as a marker of the severity for this species (Alexandre et al.
2010). From the case reports described in Table II,
the association between severe cases with thrombocytopenia is evident. However,
that can be due to bias publication, where prospective studies would be needed
to validate this association. On the other hand, considering that many studies
point to a clear negative correlation between platelet count and parasitaemia
(Grynberg et al. 2007, Silva 2009), it should be investigated if thrombocytopenia
could be used in the surveillance of drug resistance, where higher parasitaemias
for prolonged periods are usually found. Interestingly, in areas where thrombocytopenia
and other types of clinical severity are frequently reported, resistant parasites
are also being simultaneously detected (Santana Filho et al. 2007, Tjitra et
al. 2008), possibly explaining why the prevalence of thrombocytopenia worldwide
is not homogeneous.
On the other side
of the clinical presentation of plasmodial infection, platelet counts were never
performed in asymptomatic parasite carriers. However, due to the very low parasitaemia
(sometimes submicroscopic) presented by these patients, it is possible that
platelet counts are normal and parallel clinical symptoms (Suarez-Mutis et al.
2007).
Avoiding the consensual
understanding that platelets are particles devoted to the maintenance of primary
haemostasis, it has been shown that platelets participate in the pathogenesis
of microvascular malaria, adhering to the endothelium when it is previously
stimulated with tumor necrosis factor (TNF) (Lou et al. 1997). Even in the non-stimulated
cerebral endothelium, platelets may adhere and facilitate the adhesion of P.
falciparum-parasitised RBCs, through CD36 is ubiquitous in endothelial cells
and, coincidentally, platelets (Wassmer et al. 2004). Platelets therefore act
by stabilising and strengthening bridges between RBCs and endothelial cells,
which is considered the cornerstone of severe falciparum malaria. Rosetting
of parasitised RBCs is also mediated through CD36 in platelets in severe malaria
(Pain et al. 2001, Chotivanich et al. 2004). In mice infected with P. berghei
ANKA, mice deficient of tissue and uroquinase plasminogen activators demonstrated
less capillary sequestration of platelets and less severe malaria (Piguet et
al. 2000). Blocking GPIIb with anti-CD41 monoclonal antibodies in the first
day of murine infection with P. berghei also led to higher production
of interleukin (IL)-10, IL-1α,
IL-6, interferon-α
and TNF and less mortality among mice, suggesting that platelets may act as
cofactors of severe malaria (Sun et al. 2003, van der Heyde et al. 2005). There
was also an inverse correlation between platelet count and TNF in patients with
vivax infection and no association between specific mutation G→A
in the position 308 in the TNF gene (a polymorphism whose functional
effect upon severe disease is hypothesised) and platelet count was observed.
More severe patients presented more severe thrombocytopenia and higher TNF levels
(Silva 2004). Platelets stimulated by parasitised RBCs may also trigger apoptosis
in endothelial cells pre-treated with TNF in a pathway mediated by tumor growth
factor (TGF)-β1
from platelets (Wassmer et al. 2006a, b). Recent evidence showing P. vivax-infected
RBCs adhering to lung endothelial cells and to the placental tissue ex vivo
indicates that in vivax, mechanisms similar to those associated with falciparum
severity may be involved (Carvalho et al. 2010). The contribution of platelets
to this adhesion, however, requires further investigation.
In children in
Kenya suffering from falciparum malaria, an inverse correlation between platelet
count and plasmatic IL-10 was seen (Casals-Pascual et al. 2006). This interpretation
is not straightforward, because IL-10 is generally associated with protection
against severe disease. The authors hypothesise, though, that IL-10 could reduce
platelet counts to avoid infected-RBC adhesion to the endothelium, as if thrombocytopenia
was a mechanism of defence against severe disease and not the cause. Studies
of vivax infection have shown thrombocytopenia to be associated with an increase
in IL-1, IL-6, IL-10 and TGF-β
(Park et al. 2003).
The role of platelet-derived
microparticles (MPs) (submicron-sized vesicles released from cells upon activation
or apoptosis) has yet to be determined in vivo. There is evidence that these
MPs participate in the endothelial activation responsible for severe cerebral
malaria in murine models (Combes et al. 2006). MPs were also associated with
coma and thrombocytopenia in severe falciparum malaria patients (Pankoui Mfonkeu
et al. 2010). Apparently, there is an increase in the amount of MPs in vivax
malaria patients, which may play a role in the acute inflammatory symptoms of
this disease (Campos et al. 2010); this role requires further investigation.
Clinical management
of malarial thrombocytopenia - To date, there is no robust evidence on how
to manage patients with malaria and thrombocytopenia. Platelet transfusion has
been widely followed, but with no confirmed efficacy. The indication of prophylactic
platelet transfusion when platelet counts are under 10,000/mm3 probably
applies only when the bone marrow is compromised and is not able to release
efficacious platelets (Rebulla 2000). This does not seem to be the case in malaria.
Keeping platelet counts between 50,000 and 100,000/mm3 is a formal
indication only in patients undergoing surgical procedures (Rebulla 2001). In
a tertiary care centre in the Western Brazilian Amazon over a 12-month period,
10.4% (20/191) of patients who received platelet transfusion were diagnosed
with vivax or falciparum malaria (Lacerda et al. 2006). The dosage was usually
below that recommended in the literature (Schlossberg & Herman 2003). In
40% of patients, the only justifications for transfusion were maintaining a
platelet count below 10,000/mm3 and discrete bleeding. In a further
6% of patients, only a very low platelet count was described. In this group
of 40% of patients, the alleged reason was minor bleeding despite having non-severe
thrombocytopenia; in 33%, no indication was verified. These data point to the
little existing evidence of the recommendations for platelet transfusion in
these patients. The corrected count increment to evaluate transfusion efficacy
was not calculated for any patient. The low efficacy of platelet transfusion
in general is well described for several acute infectious diseases (de Paula
et al. 1993), probably due to peripheral immune mechanisms of destruction that
do not spare the transfused platelets. Indications for platelet transfusion
in cases when DIC is suspected and diagnosed, the formal clinical indication
persists, as recommended elsewhere (Franchini 2005). Due to the impossibility
of using frozen platelets in routine clinical practice, other platelet substitutes
and preparations are being investigated (Blajchman 2003). Except in atypical
cases of ITP with severe bleeding, there is no evidence for the use of human
intravenous immunoglobulin, even in cases of severe thrombocytopenia (Lacerda
et al. 2004).
The use of corticoids
has never been followed, probably due to the fact that the recovery of thrombocytopenia
following antimalarial treatment is seen in almost all cases, with good prognosis
for all species that infect humans (Lacerda 2007) and with the lack of robust
evidence of immune-mediated destruction of platelets as a major mechanism. It
was also found that in patients with cerebral falciparum malaria, dexamethasone
exacerbated the neurological symptoms and increased the frequency of gastrointestinal
bleeding (Warrell et al. 1982, Hoffman et al. 1988). However, in none of these
studies was platelet recovery analysed as a secondary endpoint.
Immune modulators
are also candidates in the adjuvant antimalarial therapy (Muniz-Junqueira et
al. 2005, Mohanty et al. 2006), based on the drug-induced inhibition of adhesion
molecules in RBCs and platelets (Muniz-Junqueira 2007). The exploration of drugs
known by their anti-inflammatory effect, modulating TNF, e.g., pentoxyfylline
and thalidomide, upon severe malaria, could not only contribute to the understanding
of the mechanisms of severity but also clarify the association between platelets
and severe disease.
Thrombocytopenia
in other infectious diseases - Many other acute and chronic infectious diseases
share similar thrombocytopenia as part of the clinical picture and these mechanisms
may be used by proxy to explain malarial disease.
Chronic thrombocytopenia
is found in approximately 10% of patients with human immunodeficiency virus
(HIV)-1 infection and in one-third of those with acquired immunodeficiency syndrome
(Scaradavou 2002). The first cases of homosexuals with profound thrombocytopenia
in New York were classified as ITP (Karpatkin 2002), involving the presence
of serum IgG anti-GPIIIa (Karpatkin et al. 1995). Later on, this IgG was found
to be directed against GPIIIa49-66 (Nardi et al. 1997). More recently,
molecular mimicry was proposed between nef HIV-1 protein and GPIIIa49-66
(Li et al. 2005). Other chronic infectious diseases known to cause
thrombocytopenia include chronic viral hepatitis, where CIC (Samuel et al. 1999)
and PAIgG (Doi et al. 2002) are also implicated. In the case of hepatitis C
virus infection, the blockage in the maturation of megakaryocytes is mediated
by the viral RNA itself (Almeida 2003). Despite an associated medullary compromise
in visceral leishmaniasis in the canine model of Leishmania infantum
infection, anti-platelet IgG and IgM were also observed (Terrazzano et al. 2006).
In acute infection with Trypanosoma cruzi, frequent thrombocytopenia
is related to the presence of parasite trans-sialidase (Tribulatti et al. 2005).
Furthermore, during infection with any of the four dengue viruses, thrombocytopenia
is frequent and is supposed to be a criterion of dengue hemorrhagic fever (Mourão
et al. 2007). Platelet phagocytosis ex vivo has already been shown as a potential
mechanism in this acute viral disease (Honda et al. 2009). Thrombocytopenia
is also observed in leptospirosis (Nicodemo 1993), typhoid fever (Huang &
DuPont 2005), hantavirus infection (Santos et al. 2006), yellow fever (Monath
2001) and sepsis (Becchi et al. 2006), whose mechanisms are poorly understood.
The high frequency of thrombocytopenia in other infectious diseases, as a rule,
changes the paradigm that platelets are essential only to haemostasis, supporting
their role as important contributors to modulate the immune response. In any
case, studies focusing on the pathogenesis of thrombocytopenia in malarial patients
should always rule out other concomitant infectious diseases, which is difficult
in socio-economically deprived study populations suffering large burdens of
multiple diseases.
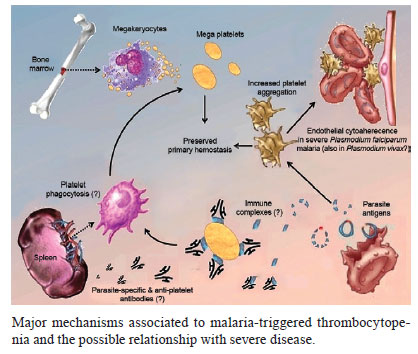
The frequency of
thrombocytopenia (i.e., platelet count below 150,000/mm3) in malarial
infection ranges from 24-94% in the literature, despite the low occurrence of
severe bleeding, even in the case of severe malaria. It is still unclear whether
this haematological complication is more frequent in P. vivax or P.
falciparum malaria. In Figure, the major mechanisms involved
in the pathogenesis are highlighted, but further studies are still needed to
clarify the impact of each mechanism and its clinical relevance. The clinical
management of malarial thrombocytopenia is expectant and the level of evidence
for platelet transfusion is insufficient to recommend this practice. It is not
clear whether platelets are diminished during acute malarial infection as a
consequence of the immune response to the parasite present or whether platelets
are actually involved in the generation of severe disease.
Acknowledgements
To Alex Kumar,
for critical and linguistic review of the manuscript, and to Mary Galinski,
for inspiring the title. This review is dedicated to Simon Karpatkin and Vanize
Oliveira Macêdo.
References
- Aggarwal A, Rath
S, Shashiraj 2005. Plasmodium vivax malaria presenting with severe thrombocytopenia.
J Trop Pediatr 51: 120-121.
- Alecrim MGC 2000. Clinical aspects, resistance and parasitary polymorphism of Plasmodium
vivax malaria in Manaus, PhD Thesis, Universidade de Brasília,
Brasília, 176 pp.
- Alexandre MA, Ferreira
CO, Siqueira AM, Magalhaes BL, Mourao MPG, Lacerda MVG, Alecrim MGC 2010. Severe Plasmodium vivax malaria, Brazilian Amazon. Emerg Infect Dis 16:
1611-1614.
- Almeida AJ 2003. Trombocitopenia associada ao HCV: aspectos clínico-laboratoriais e
virológicos, MD Thesis, Fundação Oswaldo Cruz, Rio
de Janeiro, 110 pp.
- Andrade BB, Reis-Filho
A, Souza-Neto SM, Clarencio J, Camargo LM, Barral A, Barral-Netto M 2010. Severe Plasmodium vivax malaria exhibits marked inflammatory imbalance. Malar
J 9: 13.
- Anstey NM, Currie
BJ, Dyer ME 1992. Profound thrombocytopenia due to Plasmodium vivax malaria. Aust N Z J Med 22: 169-170.
- Araujo CF, Lacerda
MV, Abdalla DS, Lima ES 2008. The role of platelet and plasma markers of antioxidant
status and oxidative stress in thrombocytopenia among patients with vivax malaria. Mem Inst Oswaldo Cruz 103: 517-521.
- Araújo Filho
JA, Bressan FR, Tourinho TM, Souza MVL, Pereira LI 2003. Plaquetopenia acentuada
associada à malária pelo P. vivax. Anais do XIII Congresso
Brasileiro de Infectologia, Goiânia. Braz J Infect Dis 7 (Suppl.
1): 25.
- Bashawri LA, Mandil
AA, Bahnassy AA, Ahmed MA 2002. Malaria: hematological aspects. Ann Saudi
Med 22: 372-376.
- Batista D 1946. O paludismo na Amazônia: contribuição à epidemiologia,
à protozoologia e à clínica; estudo sôbre a febre
biliosa-hemoglobinúrica; síntese, Imprensa Nacional, Rio de
Janeiro, 212 pp.
- Beale PJ, Cormack
JD, Oldrey TB 1972. Thrombocytopenia in malaria with immunoglobulin (IgM) changes. BMJ 1: 345-349.
- Becchi C, Al Malyan
M, Fabbri LP, Marsili M, Boddi V, Boncinelli S 2006. Mean platelet volume trend
in sepsis: is it a useful parameter? Minerva Anestesiol 72: 749-756.
- Bhatia V, Bhatia
J 2010. Severe thrombocytopenia with bleeding manifestations in two children
secondary to Plasmodium vivax. Platelets 21: 307-309.
- Blajchman MA 2003.
Substitutes and alternatives to platelet transfusions in thrombocytopenic patients. J Thromb Haemost 1: 1637-1641.
- Brown KM, Kreier
JP 1982. Plasmodium berghei malaria: blockage by immune complexes of
macrophage receptors for opsonized plasmodia. Infect Immun 37: 1227-1233.
- Campos FM, Franklin
BS, Teixeira-Carvalho A, Filho AL, de Paula SC, Fontes CJ, Brito CF, Carvalho
LH 2010. Augmented plasma microparticles during acute Plasmodium vivax infection. Malar J 9: 327.
- Carvalho BO, Lopes
SC, Nogueira PA, Orlandi PP, Bargieri DY, Blanco YC, Mamoni R, Leite JA, Rodrigues
MM, Soares IS, Oliveira
TR, Wunderlich G, Lacerda MV, Del Portillo HA, Araujo MO, Russell B, Suwanarusk
R, Snounou G, Renia L, Costa FT 2010. On the cytoadhesion of Plasmodium vivax-infected
erythrocytes. J Infect Dis 202: 638-647.
- Casals-Pascual
C, Kai O, Newton CR, Peshu N, Roberts DJ 2006. Thrombocytopenia in falciparum
malaria is associated with high concentrations of IL-10. Am J Trop Med Hyg
75: 434-436.
- Chagas C 1903. Hematological studies of impaludism, MD Thesis, Manguinhos Institute,
Rio de Janeiro, 143 pp.
- Chotivanich K,
Sritabal J, Udomsangpetch R, Newton P, Stepniewska KA, Ruangveerayuth R, Looareesuwan
S, Roberts DJ, White NJ 2004. Platelet-induced autoagglutination of Plasmodium
falciparum-infected red blood cells and disease severity in Thailand. J
Infect Dis 189: 1052-1055.
- Combes V, Coltel
N, Faille D, Wassmer SC, Grau GE 2006. Cerebral malaria: role of microparticles
and platelets in alterations of the blood-brain barrier. Int J Parasitol
36: 541-546.
- Conte R, Tassi
C, Belletti D, Ricci F, Tazzari PL 2003. Autoimmune thrombocytopenia in malaria. Vox Sang 85: 221.
- Cummins D, Faint
R, Yardumian DA, Dawling S, Mackie I, Machin SJ 1990. The in vitro and ex vivo effects of chloroquine sulphate on platelet function: implications
for malaria prophylaxis in patients with impaired haemostasis. J Trop Med
Hyg 93: 112-115.
- D'Acremont V, Landry
P, Mueller I, Pecoud A, Genton B 2002. Clinical and laboratory predictors of
imported malaria in an outpatient setting: an aid to medical decision making
in returning travelers with fever. Am J Trop Med Hyg 66: 481-486.
- Daniel-Ribeiro
CT 2000. Is there a role for autoimmunity in immune protection against malaria? Mem Inst Oswaldo Cruz 95: 199-207.
- Daniel-Ribeiro
CT, Zanini G 2000. Autoimmunity and malaria: what are they doing together? Acta
Trop 76: 205-221.
- Davidson RA 1985.
Immunology of parasitic infections. Med Clin North Am 69: 751-758.
- de Paula LV, Klafke
A, Bordin R, Pereira JPM, Job FM 1993. Avaliação da eficácia
das transfusões de concentrados de plaquetas nos Serviços de Hematologia
e Hemoterapia do Hospital de Clínicas de Porto Alegre. Bol Soc Bras
Hematol Hemoter 15: 9-13.
- del Portillo HA,
Lanzer M, Rodriguez-Malaga S, Zavala F, Fernandez-Becerra C 2004. Variant genes
and the spleen in Plasmodium vivax malaria. Int J Parasitol 34:
1547-1554.
- Dennis LH, Eichelberger
JW, Inman MM, Conrad ME 1967. Depletion of coagulation factors in drug-resistant Plasmodium falciparum malaria. Blood 29: 713-721.
- Doi T, Homma H,
Mezawa S, Kato J, Kogawa K, Sakamaki S, Niitsu Y 2002. Mechanisms for increment
of platelet associated IgG and platelet surface IgG and their implications in
immune thrombocytopenia associated with chronic viral liver disease. Hepatol
Res 24: 23.
- Echeverri M, Tobon
A, Alvarez G, Carmona J, Blair S 2003. Clinical and laboratory findings of Plasmodium
vivax malaria in Colombia 2001. Rev Inst Med Trop Sao Paulo 45: 29-34.
- Engwerda CR, Beattie
L, Amante FH 2005. The importance of the spleen in malaria. Trends Parasitol
21: 75-80.
- Erel O, Kocyigit
A, Bulut V, Avci S, Aktepe N 1998. Role of lipids, lipoproteins and lipid peroxidation
in thrombocytopenia in patients with vivax malaria. Haematologia (Budap)
29: 207-212.
- Erel O, Vural H,
Aksoy N, Aslan G, Ulukanligil M 2001. Oxidative stress of platelets and thrombocytopenia
in patients with vivax malaria. Clin Biochem 34: 341-344.
- Essien EM, Ebhota
MI 1981. Platelet hypersensitivity in acute malaria (Plasmodium falciparum)
infection in man. Thromb Haemost 46: 547-549.
- Fajardo LF, Tallent
C 1974. Malarial parasites within human platelets. J Am Med Assoc 229:
1205-1207.
- Franchini M 2005.
Pathophysiology, diagnosis and treatment of disseminated intravascular coagulation:
an update. Clin Lab 51: 633-639.
- George P, Alexander
LM 2010. A study on the clinical profile of complicated Plasmodium vivax mono-infections. Asian Pac J Trop Med 3: 560-562.
- Gerardin P, Rogier
C, Ka AS, Jouvencel P, Brousse V, Imbert P 2002. Prognostic value of thrombocytopenia
in African children with falciparum malaria. Am J Trop Med Hyg 66: 686-691.
- Gonzalez B, Rodulfo
H, De Donato M, Berrizbeitia M, Gomez C, Gonzalez L 2009. Hematologic variations
in patient with malaria caused by Plasmodium vivax before, during and
after treatment. Invest Clin 50: 187-201.
- Gonzalez LM, Guzman
M, Carmona J, Lopera T, Blair S 2000. Clinical and epidemiologic characteristics
of 291 hospitalized patients for malaria in Medellin (Colombia). Acta Med
Colomb 25: 163-170.
- Grau GE, Piguet
PF, Gretener D, Vesin C, Lambert PH 1988. Immunopathology of thrombocytopenia
in experimental malaria. Immunology 65: 501-506.
- Greenwood BM 1968.
Autoimmune disease and parasitic infections in Nigerians. Lancet 2: 380-382.
- Grynberg P, Fernandes
Fontes CJ, Braga EM 2007. Association between particular polymorphic residues
on apical membrane antigen 1 (AMA-1) and platelet levels in patients with vivax
malaria. Clin Microbiol Infect 13: 1089-1094.
- Harish R, Gupta
S 2009. Plasmodium vivax malaria presenting with severe thrombocytopenia,
cerebral complications and hydrocephalus. Indian J Pediatr 76: 551-552.
- Hill GJ, Knight
V, Jeffery GM 1964. Thrombocytopenia in vivax malaria. Lancet 39: 240-241.
- Hoffman SL, Rustama
D, Punjabi NH, Surampaet B, Sanjaya B, Dimpudus AJ, McKee KT, Jr., Paleologo
FP, Campbell JR, Marwoto H 1988. High-dose dexamethasone in quinine-treated
patients with cerebral malaria: a double-blind, placebo-controlled trial. J
Infect Dis 158: 325-331.
- Holland BH, Walker
AN, Collier L, Stephens JL 2004. Severe thrombocytopenia and epistaxis secondary
to Plasmodium vivax infection. Internet J Infect Dis 3. Available
from: ispub.com/ostia/index.php?xmlFilePath=journals/ijid/vol3n2/vivax.xml.
- Honda S, Saito
M, Dimaano EM, Morales PA, Alonzo MT, Suarez LA, Koike N, Inoue S, Kumatori
A, Matias RR, Natividad FF, Oishi K 2009. Increased phagocytosis of platelets
from patients with secondary dengue virus infection by human macrophages. Am
J Trop Med Hyg 80: 841-845.
- Huang DB, DuPont
HL 2005. Problem pathogens: extra-intestinal complications of Salmonella
enterica serotype typhi infection. Lancet Infect Dis 5: 341-348.
- Inyang AL, Sodeinde
O, Okpako DT, Essien EM 1987. Platelet reactions after interaction with cultured Plasmodium falciparum infected erythrocytes. Br J Haematol 66:
375-378.
- Jadhav UM, Patkar
VS, Kadam NN 2004. Thrombocytopenia in malaria - correlation with type and severity
of malaria. J Assoc Physicians India 52: 615-618.
- Jaff MS, McKenna
D, McCann SR 1985. Platelet phagocytosis: a probable mechanism of thrombocytopenia
in Plasmodium falciparum infection. J Clin Pathol 38: 1318-1319.
- Kakar A, Bhoi S,
Prakash V, Kakar S 1999. Profound thrombocytopenia in Plasmodium vivax malaria. Diagn Microbiol Infect Dis 35: 243-244.
- Karpatkin S 2002.
HIV-1 related thrombocytopenia. In AD Michelson, Platelets, Elsevier
Academic Press, California, p. 559-570.
- Karpatkin S, Nardi
MA, Hymes KB 1995. Sequestration of anti-platelet GPIIIa antibody in rheumatoid
factor immune complexes of human immunodeficiency virus 1 thrombocytopenic patients. Proc Natl Acad Sci USA 92: 2263-2267.
- Katira B, Shah
I 2006. Thrombocytopenia in Plasmodium vivax infected children. J
Vector Borne Dis 43: 147-149.
- Kaur D, Wasir V,
Gulati S, Bagga A 2007. Unusual presentation of Plasmodium vivax malaria
with severe thrombocytopenia and acute renal failure. J Trop Pediatr 53:
210-212.
- Kelton JG, Keystone
J, Moore J, Denomme G, Tozman E, Glynn M, Neame PB, Gauldie J, Jensen J 1983.
Immune-mediated thrombocytopenia of malaria. J Clin Invest 71: 832-836.
- Khan FY, Lutof
AK, Yassin MA, Khattab MA, Saleh M, Rezeq HY, Almaslamani M 2009. Imported malaria
in Qatar: a one year hospital-based study in 2005. Travel Med Infect Dis
7: 111-117.
- Kochar DK, Das
A, Kochar A, Middha S, Acharya J, Tanwar GS, Gupta A, Pakalapati D, Garg S,
Saxena V, Subudhi AK, Boopathi PA, Sirohi P, Kochar SK 2010. Thrombocytopenia
in Plasmodium falciparum, Plasmodium vivax and mixed infection
malaria: a study from Bikaner (Northwestern India). Platelets 21: 623-627.
- Kochar DK, Saxena
V, Singh N, Kochar SK, Kumar SV, Das A 2005. Plasmodium vivax malaria. Emerg Infect Dis 11: 132-134.
- Koltas IS, Demirhindi
H, Hazar S, Ozcan K 2007. Supportive presumptive diagnosis of Plasmodium
vivax malaria. Thrombocytopenia and red cell distribution width. Saudi
Med J 28: 535-539.
- Komoda M, Fujimoto
T, Kawaguchi Y, Tsushima H, Fukushima T, Hata T, Miyazaki Y, Tsukasaki K, Tomonaga
M 2006. Plasmodium vivax malaria with clinical presentation mimicking
acute type idiopathic thrombocytopenic purpura (abstract). Rinsho Ketsueki
47: 1453-1456.
- Kortepeter M, Brown
JD 1998. A review of 79 patients with malaria seen at a military hospital in
Hawaii from 1979 to 1995. Mil Med 163: 84-89.
- Kreil A, Wenisch
C, Brittenham G, Looareesuwan S, Peck-Radosavljevic M 2000. Thrombopoietin in Plasmodium falciparum malaria. Br J Haematol 109: 534-536.
- Kumar A, Shashirekha
2006. Thrombocytopenia: an indicator of acute vivax malaria. Indian J Pathol
Microbiol 49: 505-508.
- Lacerda MV, Alexandre
MA, Santos PD, Arcanjo AR, Alecrim WD, Alecrim MGC 2004. Idiopathic thrombocytopenic
purpura due to vivax malaria in the Brazilian Amazon. Acta Trop 90: 187-190.
- Lacerda MV, Hipolito
JR, Passos LN 2008. Chronic Plasmodium vivax infection in a patient with
splenomegaly and severe thrombocytopenia. Rev Soc Bras Med Trop 41: 522-523.
- Lacerda MVG 2007. Manifestações clínicas e patogênese da plaquetopenia
na malária, PhD Thesis, Universidade de Brasília, 439 pp.
- Lacerda MVG, Cavalcante
TB, Silva AC, Macêdo VO 2006. Avaliação das indicações
de transfusão de concentrado de plaquetas. Anais do XLII Congresso da
Sociedade Brasileira de Medicina Tropical, Teresina. Rev Soc Bras Med Trop
39 (Suppl. I): 104.
- Lacerda MVG, Mourão
MPG, Alecrim WD, Alecrim MGC 2001. Clinical study of patients with falciparum
malaria admitted to the Tropical Medicine Foundation of Amazonas - Brazil. Annals
of the 50th Annual Meeting of the American Society of Tropical Medicine and
Hygiene, Atlanta (USA). Am J Trop Med Hyg 65: 336.
- Lacerda MVG, Oliveira
SL, Alecrim MGC 2007. Splenic hematoma in a patient with Plasmodium vivax malaria. Rev Soc Bras Med Trop 40: 96-97.
- Ladhani S, Lowe
B, Cole AO, Kowuondo K, Newton CR 2002. Changes in white blood cells and platelets
in children with falciparum malaria: relationship to disease outcome. Br
J Haematol 119: 839-847.
- Lathia TB, Joshi
R 2004. Can hematological parameters discriminate malaria from nonmalarious
acute febrile illness in the tropics? Indian J Med Sci 58: 239-244.
- Lee SH, Looareesuwan
S, Chan J, Wilairatana P, Vanijanonta S, Chong SM, Chong BH 1997. Plasma macrophage
colony-stimulating factor and P-selectin levels in malaria-associated thrombocytopenia. Thromb Haemost 77: 289-293.
- Li Z, Nardi MA,
Karpatkin S 2005. Role of molecular mimicry to HIV-1 peptides in HIV-1-related
immunologic thrombocytopenia. Blood 106: 572-576.
- Llanos C, Quintero
G, Castellanos A, Arévalo-Herrera M, Herrera S 2006. Surgical bone marrow
aspiration in Aotus lemurinus griseimembra. J Med Primatol 35:
131-135.
- Lou J, Donati YR,
Juillard P, Giroud C, Vesin C, Mili N, Grau GE 1997. Platelets play an important
role in TNF-induced microvascular endothelial cell pathology. Am J Pathol
151: 1397-1405.
- Maina RN, Walsh
D, Gaddy C, Hongo G, Waitumbi J, Otieno L, Jones D, Ogutu BR 2010. Impact of Plasmodium falciparum infection on haematological parameters in children
living in Western Kenya. Malar J 9 (Suppl. 3): S4.
- Makkar RP, Mukhopadhyay
S, Monga A, Gupta AK 2002. Plasmodium vivax malaria presenting with severe
thrombocytopenia. Braz J Infect Dis 6: 263-265.
- Marques HO 2004. Alterações da hemostasia em pacientes com malária,
MSc Thesis, Universidade Federal de São Paulo, São Paulo, 140
pp.
- Marques HO, Alexandre
MAA, Oliveira VM, Marreira L, Lacerda MVG, Alecrim MGC, Morelli VM, Lourenço
DM 2005. Hemostatic changes in patients with malaria. Annals of the XX Congress
of the International Society on Thrombosis and Hemostasis, Sydney (Australia). J Thromb Haemost 3 (Suppl. I): 1452.
- Martin-Jaular L,
Ferrer M, Calvo M, Rosanas-Urgell A, Kalko S, Graewe S, Soria G, Cortadellas
N, Ordi J, Planas A, Burns J, Heussler V, Del Portillo HA 2011. Strain-specific
spleen remodelling in Plasmodium yoelii infections in Balb/c mice facilitates
adherence and spleen macrophage-clearance escape. Cell Microbiol 13:
109-122.
- Mast Q, de Groot
PG, van Heerde WL, Roestenberg M, van Velzen JF, Verbruggen B, Roest M, McCall
M, Nieman AE, Westendorp J, Syafruddin D, Fijnheer R, van Dongen-Lases EC, Sauerwein
RW, van der Ven AJ 2010. Thrombocytopenia in early malaria is associated with
GP1b shedding in absence of systemic platelet activation and consumptive coagulopathy. Br J Haematol 151: 495-503.
- Mast Q, Groot E,
Lenting PJ, de Groot PG, McCall M, Sauerwein RW, Fijnheer R, van der Ven A 2007.
Thrombocytopenia and release of activated von Willebrand Factor during early Plasmodium falciparum malaria. J Infect Dis 196: 622-628.
- Menendez C, Fleming
AF, Alonso PL 2000. Malaria-related anaemia. Parasitol Today 16: 469-476.
- Mohanty D, Ghosh
K, Nandwani SK, Shetty S, Phillips C, Rizvi S, Parmar BD 1997. Fibrinolysis,
inhibitors of blood coagulation, and monocyte derived coagulant activity in
acute malaria. Am J Hematol 54: 23-29.
- Mohanty D, Marwaha
N, Ghosh K, Sharma S, Garewal G, Shah S, Devi S, Das KC 1988. Functional and
ultrastructural changes of platelets in malarial infection. Trans R Soc Trop
Med Hyg 82: 369-375.
- Mohanty S, Patel
DK, Pati SS, Mishra SK 2006. Adjuvant therapy in cerebral malaria. Indian
J Med Res 124: 245-260.
- Mohapatra MK, Padhiary
KN, Mishra DP, Sethy G 2002. Atypical manifestations of Plasmodium vivax malaria. Indian J Malariol 39: 18-25.
- Monath TP 2001.
Yellow fever: an update. Lancet Infect Dis 1: 11-20.
- Moulin F, Lesage
F, Legros AH, Maroga C, Moussavou A, Guyon P, Marc E, Gendrel D 2003. Thrombocytopenia
and Plasmodium falciparum malaria in children with different exposures. Arch Dis Child 88: 540-541.
- Mourão MP,
Lacerda MV, Macedo VO, Santos JB 2007. Thrombocytopenia in patients with dengue
virus infection in the Brazilian Amazon. Platelets 18: 605-612.
- Mourão MPG,
Lacerda MVG, Magalhães L, Alecrim WD, Alecrim MGC 2001. Estudo clínico
em crianças internadas com malária (P. falciparum) na FMT-AM.
Anais do XXXVII Congresso da Sociedade Brasileira de Medicina Tropical, Salvador. Rev Soc Bras Med Trop 34 (Suppl. 1): 71.
- Muniz-Junqueira
MI 2007. Immunomodulatory therapy associated to anti-parasite drugs as a way
to prevent severe forms of malaria. Curr Clin Pharmacol 2: 59-73.
- Muniz-Junqueira
MI, Silva FO, de Paula Júnior MR, Tosta CE 2005. Thalidomide influences
the function of macrophages and increases the survival of Plasmodium berghei-infected
CBA mice. Acta Trop 94: 128-138.
- Murthy GL, Sahay
RK, Srinivasan VR, Upadhaya AC, Shantaram V, Gayatri K 2000. Clinical profile
of falciparum malaria in a tertiary care hospital. J Indian Med Assoc 98:
160-162.
- Nardi MA, Liu LX,
Karpatkin S 1997. GPIIIa(49-66) is a major pathophysiologically relevant antigenic
determinant for anti-platelet GPIIIa of HIV-1-related immunologic thrombocytopenia. Proc Natl Acad Sci USA 94: 7589-7594.
- Naveira JB 1970. Malária - aspectos hematológicos, Associate professorship
Thesis, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 104 pp.
- Nicodemo AC 1993. Análise de aspectos microscópicos, imuno-histoquímicos
e ultra-estruturais do pulmão na leptospirose para a compreensão
da patogenia da plaquetopenia, PhD Thesis, Universidade de São Paulo,
São Paulo, 153 pp.
- Noronha EF 1998. Estudo clínico-epidemiológico da malária falciparum
em crianças de 0 a 14 anos, atendidas no Instituto de Medicina Tropical
do Amazonas em Manaus - AM - Brasil, MSc Thesis, Universidade de Brasília,
Brasília, 126 pp.
- Oh MD, Shin H,
Shin D, Kim U, Lee S, Kim N, Choi MH, Chai JY, Choe K 2001. Clinical features
of vivax malaria. Am J Trop Med Hyg 65: 143-146.
- Ohtaka M, Ohyashiki
K, Iwabuchi H, Iwabuchi A, Lin KY, Toyama K 1993. A case of vivax malaria with
thrombocytopenia suggesting immunological mechanisms. Rinsho Ketsueki 34:
490-492.
- Pain A, Ferguson
DJ, Kai O, Urban BC, Lowe B, Marsh K, Roberts DJ 2001. Platelet-mediated clumping
of Plasmodium falciparum-infected erythrocytes is a common adhesive phenotype
and is associated with severe malaria. Proc Natl Acad Sci USA 98: 1805-1810.
- Panasiuk A 2001.
Autoimmune thrombocytopenia in recurrent polietiological malaria (Plasmodium
falciparum, Plasmodium vivax). Wiad Parazytol 47: 85-89.
- Pankoui Mfonkeu
JB, Gouado I, Fotso Kuate H, Zambou O, Amvam Zollo PH, Grau GE, Combes V 2010.
Elevated cell-specific microparticles are a biological marker for cerebral dysfunctions
in human severe malaria. PLoS ONE 5: e13415.
- Parakh A, Agarwal
N, Aggarwal A, Aneja A 2009. Plasmodium vivax malaria in children: uncommon
manifestations. Ann Trop Paediatr 29: 253-256.
- Park CHL, Ferreira
CB, Bianchi CP, Fazio FS, Costa JC, Padilha A, Fonseca MO, Boulos M 2002. Plaquetopenia
em pacientes com malária por Plasmodium vivax. Anais do XXXVIII
Congresso da Sociedade Brasileira de Medicina Tropical, Foz do Iguaçu. Rev Soc Bras Med Trop 35 (Suppl. 1): 370.
- Park JW, Park SH,
Yeom JS, Huh AJ, Cho YK, Ahn JY, Min GS, Song GY, Kim YA, Ahn SY, Woo SY, Lee
BE, Ha EH, Han HS, Yoo K, Seoh JY 2003. Serum cytokine profiles in patients
with Plasmodium vivax malaria: a comparison between those who presented
with and without thrombocytopenia. Ann Trop Med Parasitol 97: 339-344.
- Patel U, Gandhi
G, Friedman S, Niranjan S 2004. Thrombocytopenia in malaria. J Natl Med Assoc
96: 1212-1214.
- Peck-Radosavljevic
M 2001. Hypersplenism. Eur J Gastroenterol Hepatol 13: 317-323.
- Piguet PF, Da Laperrousaz
C, Vesin C, Tacchini-Cottier F, Senaldi G, Grau GE 2000. Delayed mortality and
attenuated thrombocytopenia associated with severe malaria in urokinase- and
urokinase receptor-deficient mice. Infect Immun 68: 3822-3829.
- Poespoprodjo JR,
Fobia W, Kenangalem E, Lampah DA, Hasanuddin A, Warikar N, Sugiarto P, Tjitra
E, Anstey NM, Price RN 2009. Vivax malaria: a major cause of morbidity in early
infancy. Clin Infect Dis 48: 1704-1712.
- Prasad R, Das BK,
Pengoria R, Mishra OP, Shukla J, Singh TB 2009. Coagulation status and platelet
functions in children with severe falciparum malaria and their correlation of
outcome. J Trop Pediatr 55: 374-378.
- Rasheed A, Saeed
S, Khan SA 2009. Clinical and laboratory findings in acute malaria caused by
various plasmodium species. J Pak Med Assoc 59: 220-223.
- Rebulla P 2000.
Trigger for platelet transfusion. Vox Sang 78 (Suppl. 2): 179-182.
- Rebulla P 2001.
Revisitation of the clinical indications for the transfusion of platelet concentrates. Rev Clin Exp Hematol 5: 288-310.
- Rifakis PM, Hernandez
O, Fernandez CT, Rodriguez-Morales AJ, Von A, Franco-Paredes C 2008. Atypical Plasmodium vivax malaria in a traveler: bilateral hydronephrosis, severe
thrombocytopenia, and hypotension. J Travel Med 15: 119-121.
- Rios-Orrego A,
Alvarez-Castillo T, Carmona-Fonseca J, Blair-Trujillo S 2005. Temporal evolution
of platelets and anti-platelet antibodies in patients of endemic area with non
complicated malaria. An Med Interna 22: 561-568.
- Robinson P, Jenney
AW, Tachado M, Yung A, Manitta J, Taylor K, Biggs BA 2001. Imported malaria
treated in Melbourne, Australia: epidemiology and clinical features in 246 patients. J Travel Med 8: 76-81.
- Rodriguez-Morales
AJ, Sanchez E, Vargas M, Piccolo C, Colina R, Arria M 2006. Anemia and thrombocytopenia
in children with Plasmodium vivax malaria. J Trop Pediatr 52:
49-51.
- Rodriguez-Morales
AJ, Sanchez E, Vargas M, Piccolo C, Colina R, Arria M, Franco-Paredes C 2005.
Occurrence of thrombocytopenia in Plasmodium vivax malaria. Clin Infect
Dis 41: 130-131.
- Rogier C, Gerardin
P, Imbert P 2004. Thrombocytopenia is predictive of lethality in severe childhood
falciparum malaria. Arch Dis Child 89: 795-796.
- Samuel H, Nardi
M, Karpatkin M, Hart D, Belmont M, Karpatkin S 1999. Differentiation of autoimmune
thrombocytopenia from thrombocytopenia associated with immune complex disease:
systemic lupus erythematosus, hepatitis-cirrhosis, and HIV-1 infection by platelet
and serum immunological measurements. Br J Haematol 105: 1086-1091.
- Santana Filho FS,
Arcanjo AR, Chehuan YM, Costa MR, Martinez-Espinosa FE, Vieira JL, Barbosa MG,
Alecrim WD, Alecrim MG 2007. Chloroquine-resistant Plasmodium vivax,
Brazilian Amazon. Emerg Infect Dis 13: 1125-1126.
- Santos MC, Lacerda
MVG, Benedetti SM, Albuquerque BC, Aguiar Filho AA, Elkhoury MR, Rosa ES, Vasconcelos
PF, Medeiros DB, Mourao MPG 2006. Human hantavirus infection, Brazilian Amazon. Emerg Infect Dis 12: 1165-1167.
- Santos PD 2000. Correlação entre níveis séricos de Intermediários
Reativos de Nitrogênio (IRN) e malária em pacientes da Fundação
de Medicina Tropical do Amazonas (FMT/IMT-AM), MSc Thesis, Universidade
Federal do Amazonas, Manaus, 133 pp.
- Scaradavou A 2002.
HIV-related thrombocytopenia. Blood Rev 16: 73-76.
- Schlossberg HR,
Herman JH 2003. Platelet dosing. Transfus Apher Sci 28: 221-226.
- Shaikh QH, Ahmad
SM, Abbasi A, Malik SA, Sahito AA, Munir SM 2009. Thrombocytopenia in malaria. J Coll Physicians Surg Pak 19: 708-710.
- Shear HL 1984.
Murine malaria: immune complexes inhibit Fc receptor-mediated phagocytosis. Infect Immun 44: 130-136.
- Silva IBA 2004. Malária vivax: manifestações clínicas e laboratoriais
relacionadas com o fator de necrose tumoral alfa, PhD Thesis, Universidade
Federal do Pará, Belém, 128 pp.
- Silva SBR 2009. Avaliação da frequência e dos fatores associados à
plaquetopenia causada pelo Plasmodium vivax, MSc Thesis, Universidade Federal
do Mato Grosso, 64 pp.
- Silva SL, Santana
Filho FS, Arcanjo ARL, Alecrim WD, Alecrim MGC 2000. Perfil clínico e
hematológico dos pacientes internados com malária por Plasmodium
vivax e plaquetopenia, na Fundação de Medicina Tropical do
Amazonas, no período de janeiro de 1997 a setembro de 1999. Anais do
XXXVI Congresso da Sociedade Brasileira de Medicina Tropical, São Luís
do Maranhão , Rev Soc Bras Med Trop 33 (Suppl. 1): 348.
- Skudowitz RB, Katz
J, Lurie A, Levin J, Metz J 1973. Mechanisms of thrombocytopenia in malignant
tertian malaria. BMJ 2: 515-518.
- Song JY, Park CW,
Jo YM, Kim JY, Kim JH, Yoon HJ, Kim CH, Lim CS, Cheong HJ, Kim WJ 2007. Two
cases of Plasmodium vivax malaria with the clinical picture resembling
toxic shock. Am J Trop Med Hyg 77: 609-611.
- Srichaikul T, Pulket
C, Sirisatepisarn T, Prayoonwiwat W 1988. Platelet dysfunction in malaria. Southeast
Asian J Trop Med Public Health 19: 225-233.
- Srichaikul T, Puwasatien
P, Karnjanajetanee J, Bokisch VA, Pawasatien P 1975. Complement changes and
disseminated intravascular coagulation in Plasmodium falciparum malaria. Lancet 1: 770-772.
- Srivastava S, Ahmad
S, Shirazi N, Kumar Verma S, Puri P 2011. Retrospective analysis of vivax malaria
patients presenting to tertiary referral centre of Uttarakhand. Acta Trop
117: 82-85.
- Suarez-Mutis MC,
Cuervo P, Leoratti FM, Moraes-Avila SL, Ferreira AW, Fernandes O, Coura JR 2007.
Cross sectional study reveals a high percentage of asymptomatic Plasmodium
vivax infection in the Amazon Rio Negro area, Brazil. Rev Inst Med Trop
Sao Paulo 49: 159-164.
- Sun G, Chang WL,
Li J, Berney SM, Kimpel D, van der Heyde HC 2003. Inhibition of platelet adherence
to brain microvasculature protects against severe Plasmodium berghei malaria. Infect Immun 71: 6553-6561.
- Takaki K, Aoki
T, Akeda H, Kajiwara T, Honda S, Maeda Y, Okada K, Sawae Y 1991. A case of Plasmodium
vivax malaria with findings of DIC. Kansenshogaku Zasshi 65: 488-492.
- Tan SO, McGready
R, Zwang J, Pimanpanarak M, Sriprawat K, Thwai KL, Moo Y, Ashley EA, Edwards
B, Singhasivanon P, White NJ, Nosten F 2008. Thrombocytopaenia in pregnant women
with malaria on the Thai-Burmese border. Malar J 7: 209.
- Taylor WR, Widjaja
H, Basri H, Ohrt C, Taufik T, Tjitra E, Baso S, Fryauff D, Hoffman SL, Richie
TL 2008. Changes in the total leukocyte and platelet counts in Papuan and non
Papuan adults from northeast Papua infected with acute Plasmodium vivax or uncomplicated Plasmodium falciparum malaria. Malar J 7: 259.
- Terrazzano G, Cortese
L, Piantedosi D, Zappacosta S, Di Loria A, Santoro D, Ruggiero G, Ciaramella
P 2006. Presence of anti-platelet IgM and IgG antibodies in dogs naturally infected
by Leishmania infantum. Vet Immunol Immunopathol 110: 331-337.
- Thapa R, Biswas
B, Mallick D, Sardar S, Modak S 2009. Childhood Plasmodium vivax malaria
with severe thrombocytopenia and bleeding manifestations. J Pediatr Hematol
Oncol 31: 758-759.
- Tjitra E, Anstey
NM, Sugiarto P, Warikar N, Kenangalem E, Karyana M, Lampah DA, Price RN 2008.
Multidrug-resistant Plasmodium vivax associated with severe and fatal
malaria: a prospective study in Papua, Indonesia. PLoS Med 5: e128.
- Touze JE, Mercier
P, Rogier C, Hovette P, Schmoor P, Dabanian C, Campiadgi S, Laroche R 1990.
Platelet antibody activity in malaria thrombocytopenia. Pathol Biol (Paris)
38: 678-681.
- Tribulatti MV,
Mucci J, Van Rooijen N, Leguizamon MS, Campetella O 2005. The trans-sialidase
from Trypanosoma cruzi induces thrombocytopenia during acute Chagas'
disease by reducing the platelet sialic acid contents. Infect Immun 73:
201-207.
- Tyagi P, Biswas
S 1999. Naturally occurring plasmodia-specific circulating immune complexes
in individuals of malaria endemic areas in India. Indian J Malariol 36:
12-18.
- Urban BC, Hien
TT, Day NP, Phu NH, Roberts R, Pongponratn E, Jones M, Mai NTH, Bethell D, Turner
GDH, Ferguson D, White NJ, Roberts DJ 2005. Fatal Plasmodium falciparum malaria causes specific patterns of splenic architectural disorganization. Infect
Immun 73: 1986-1994.
- van der Heyde HC,
Gramaglia I, Sun G, Woods C 2005. Platelet depletion by anti-CD41 (alphaIIb)
mAb injection early but not late in the course of disease protects against Plasmodium
berghei pathogenesis by altering the levels of pathogenic cytokines. Blood
105: 1956-1963.
- Victoria MB, Victoria
F, Coelho AHV, Santos LO, Alecrim MGC 1998. Púrpura trombocitopênica
em paciente com malária por Plasmodium vivax: relato de caso.
Anais do XXXIV Congresso da Sociedade Brasileira de Medicina Tropical, Manaus. Rev Soc Bras Med Trop 31 (Suppl. 1): 55.
- Vij AS, Dandona
PK, Aggarwal A 2008. Malaria with marked thrombocytopenia: report of 2 cases. J Indian Med Assoc 106: 123-125.
- Warrell DA, Looareesuwan
S, Warrell MJ, Kasemsarn P, Intaraprasert R, Bunnag D, Harinasuta T 1982. Dexamethasone
proves deleterious in cerebral malaria. A double-blind trial in 100 comatose
patients. N Engl J Med 306: 313-319.
- Wassmer SC, Combes
V, Candal FJ, Juhan-Vague I, Grau GE 2006a. Platelets potentiate brain endothelial
alterations induced by Plasmodium falciparum. Infect Immun 74:
645-653.
- Wassmer SC, Lepolard
C, Traore B, Pouvelle B, Gysin J, Grau GE 2004. Platelets reorient Plasmodium
falciparum-infected erythrocyte cytoadhesion to activated endothelial cells. J Infect Dis 189: 180-189.
- Wassmer SC, Souza
JB, Frere C, Candal FJ, Juhan-Vague I, Grau GE 2006b. TGF-beta1 released from
activated platelets can induce TNF-stimulated human brain endothelium apoptosis:
a new mechanism for microvascular lesion during cerebral malaria. J Immunol
176: 1180-1184.
- Watier H, Verwaerde
C, Landau I, Werner E, Fontaine J, Capron A, Auriault C 1992. T-cell-dependent
immunity and thrombocytopenia in rats infected with Plasmodium chabaudi. Infect Immun 60: 136-142.
- WHO - World Health
Organization 2010. Guidelines for the treatment of malaria [homepage on
the Internet]: 2010. Available from: whqlibdoc.who.int/publications/2010/9789241547925_eng.pdf.
- Wickramasinghe
SN, Abdalla SH 2000. Blood and bone marrow changes in malaria. Baillieres
Best Pract Res Clin Haematol 13: 277-299.
- Yamaguchi S, Kubota
T, Yamagishi T, Okamoto K, Izumi T, Takada M, Kanou S, Suzuki M, Tsuchiya J,
Naruse T 1997. Severe thrombocytopenia suggesting immunological mechanisms in
two cases of vivax malaria. Am J Hematol 56: 183-186.
Copyright © 2011 - Instituto Oswaldo Cruz - Fiocruz
The following images related to this document are available:
Photo images
[oc11140f1.jpg]
[oc11140t2.jpg]
[oc11140t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}