 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memorias do Instituto Oswaldo Cruz, Vol. 106, No. 7, November 2011 Schistosomal glomerulopathy and changes in the distribution of histological patterns of glomerular diseases in Bahia, Brazil Washington Luis Conrado dos-SantosI, II*; Glória Maria Maranhão SweetI; Marília Bahiense-OliveiraII; Paulo Novis RochaIII ICentro
de Pesquisas Gonçalo Moniz-Fiocruz, Rua Waldemar Falcão 121, 40296-710
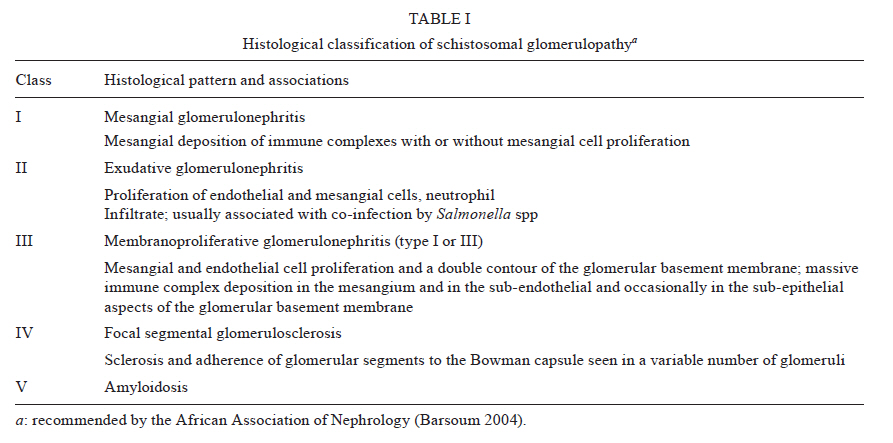
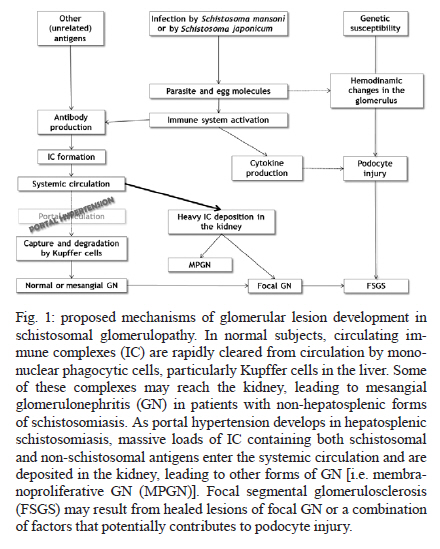
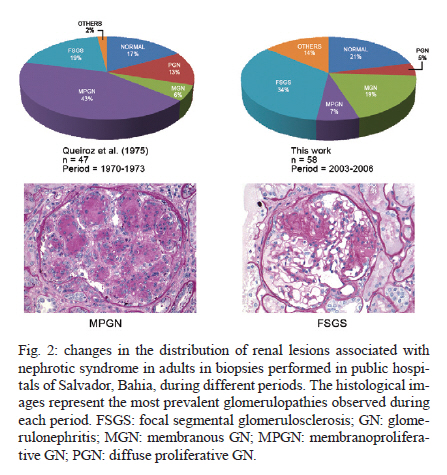
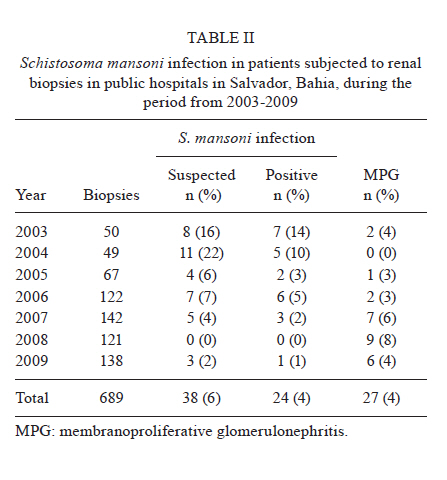
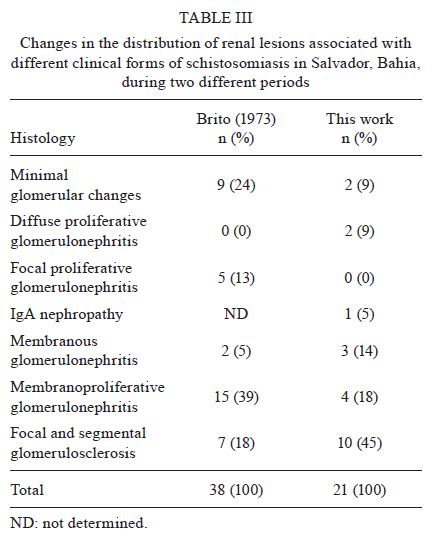
Salvador, BA, Brasil Code Number: oc11179 ABSTRACT Distinct patterns of glomerular lesions, including membranoproliferative glomerulonephritis and focal segmental glomerulosclerosis, are associated with infection by Schistosoma mansoni or Schistosoma japonicum. Evidence suggests that immune complex deposition is the main mechanism underlying the different forms of schistosomal glomerulonephritis and that immune complex deposition may be intensified by portal hypertension. The relationship between focal segmental glomerulosclerosis and schistosomiasis remains poorly understood. A clinicopathologic classification of schistosomal glomerulopathies was proposed in 1992 by the African Association of Nephrology. In Brazil, mass treatment with oral medications has led to a decrease in the occurrence of schistosomal glomerulopathy. In a survey of renal biopsies performed in Salvador, Brazil, from 2003-2009, only 24 (4%) patients were identified as positive for S. mansoni infection. Among these patients, only one had the hepatosplenic form of the disease. Focal segmental glomerulosclerosis was found in seven patients and membranoproliferative glomerulonephritis was found in four patients. Although retrospective studies on the prevalence of renal diseases based on kidney biopsies may be influenced by many patient selection biases, a change in the distribution of glomerulopathies associated with nephrotic syndrome was observed along with a decline in the occurrence of severe forms of schistosomiasis. Key words: schistosomiasis - Schistosoma mansoni - Schistosoma japonicum - mesangiocapillary glomerulonephritis - kidney diseases - focal segmental glomerulosclerosis Schistosomal glomerulopathy was classified as a clinicopathological entity following the publication of a series of studies published mainly by Brazilian researchers in the 1960s and 1970s. The evidence supporting the classification of schistosomal glomerulopathy as a distinct disease comes from the following observations: (i) clinical and laboratory signs of renal disease are more prevalent in patients with hepatosplenic schistosomiasis than in patients with other clinical forms of Schistosoma mansoni infection or in non-infected controls (reviewed by Andrade & de Queiroz 1968), (ii) the frequency of severe glomerular lesions is higher in patients with hepatosplenic schistosomiasis than in patients with hepatic cirrhosis or other unrelated diseases (Andrade & de Queiroz 1968), (iii) schistosomal glomerulopathy has been experimentally reproduced in different animal species infected with S. mansoni or Schistosoma japonicum (De Brito et al. 1971, Andrade & Susin 1974, Cavallo et al. 1974), (iv) schistosomal antigen-containing immune complexes (IC) have been identified in the kidneys of S. mansoni or S. japonicum-infected patients and experimental animals, even in non-hepatosplenic forms of the disease (Hoshino-Shimizu et al. 1975, van Marck et al. 1981) and (v) a sequential temporal relationship between Schistosoma infection and the appearance of renal lesions has been observed in experimental studies and is suggested by follow-up studies of transplant patients (Falcao & Gould 1975). The overall frequency of glomerulopathy was 12% in patients with hepatosplenic schistosomiasis compared with 5.6% in the global population of patients autopsied in a general hospital (Andrade et al. 1971). A similar frequency (12.7%) of renal disease was reported in a recent study involving 63 patients with hepatosplenic schistosomiasis from Minas Gerais, Brazil (Rodrigues et al. 2010). A variety of anatomopathological patterns of glomerular lesions have been associated with schistosomal glomerulopathy, due mainly to the intensity of infection, the emergence of portal hypertension and the association with infections by other pathogens (van Marck et al. 1977, Ramos & Andrade 1987, Zeid et al. 1994, Chisty et al. 2002, Barsoum 2004). The diversity observed among the lesions associated with schistosomiasis motivated a clinicopathologic classification of schistosomal glomerulopathies, endorsed in 1992 by the African Association of Nephrology (AFRAN) (Barsoum 2004), that recognized the five categories of glomerular diseases shown in Table I. Class I (mesangioproliferative glomerulonephritis) may be the most prevalent form of schistosomal glomerulopathy seen in patients with hepato-intestinal or hepatosplenic schistosomiasis (Sobh et al. 1990). Patients with this form of the disease are clinically normal or they may present mild proteinuria or nephrotic syndrome. Mesangial and paramesangial deposits with mesangial cell proliferation are observed in the glomeruli. Class II (exudative glomerulonephritis) occurs in the presence of concomitant infection by Schistosoma and Salmonella species. Patients may have nephrotic or nephritic syndrome and a proliferative glomerulonephritis with neutrophil infiltration of the glomeruli (Bassily et al. 1976, Rocha et al. 1976, Martinelli et al. 1992). Class III (membranoproliferative glomerulonephritis) and Class IV (focal segmental glomerulosclerosis) represent the patterns of glomerular lesion that are most consistently associated with the hepatosplenic form of schistosomiasis in Brazil. Both are associated with nephrotic syndrome and with progression to chronic kidney disease. Class V (renal amyloidosis) has been reported in Africa, but its association with S. mansoni infection in Brazil remains controversial (Sadigursky & Andrade 1976, Strausbaugh et al. 1978). Recently, another class (Class VI) has been proposed as an addition to the AFRAN classification of schistosomal glomerulopathy. This lesion consists of mesangial proliferation associated with apoptotic transient cellular infiltrations, amyloidosis and cryoglobulin deposition, which are attributed to the combined effect of infection by Schistosoma spp and hepatitis C virus (Barsoum 2004). The suggested mechanism underlying schistosomal glomerulonephritis is immune complex deposition in the mesangial, sub-endothelial and sub-epithelial regions of the glomerulus. IC of IgG, IgM and complement, together with parasite antigens and IgA aggregates, have been identified in the glomeruli of both human and experimental animals with mesangioproliferative and membranoproliferative glomerulonephritis. Immune complex deposition may be intensified by the portosystemic shunt secondary to portal hypertension [Fig. 1] (van Marck et al. 1979). Co-infection by Salmonella or hepatitis B and C viruses, other co-morbidities and genetic background may add complexity to the pattern of glomerular lesions (Jones 1977, Zeid et al. 1994, Abdul-Fattah et al. 1995, Barsoum 2004). Although immune complex deposition has been consistently demonstrated in schistosomal glomerulonephritis, the relationship between focal segmental glomerulosclerosis and schistosomiasis remains unclear [Fig. 1]. The genetic background of a predominantly Afro-descendant population infected by the parasite has been proposed as a possible explanation (Lopes et al. 2002). Schistosomal glomerulopathy is more frequently associated with S. mansoni and S. japonicum infection. In Brazil, mass treatment with oral medications has led to a decrease in the occurrence of the hepatosplenic form of schistosomiasis and a similar impact has been seen on the occurrence of schistosomal glomerulopathy (Correia et al. 1997). This change in the frequency of schistosomal glomerulopathy may be reflected in the change in the distribution of glomerular lesions associated with nephrotic syndrome in adults (over 15 years old) that was reported by Queiroz et al. (1973) between 1970-1973 and that we noted in a study conducted between 2003-2006 [Fig. 2]. Membranoproliferative glomerulonephritis was the most prevalent renal lesion observed in adult patients with nephrotic syndrome in the study by Queiroz et al. (1973). In our study, focal segmental glomerulosclerosis was the predominant pattern of disease in this group of patients. Furthermore, a survey carried out by the Renal Pathology Services at the Gonçalo Moniz Research Centre-Fiocruz (Salvador, Brazil) revealed a decline in the occurrence of the report of S. mansoni infection in biopsy request forms from 2-16% between 2003-2009 [Table II]. Positive results for S. mansoni infection were reported for 24/689 (4%) patients and hepatosplenomegaly was reported in only one of these patients. Among the whole group of patients who tested positive for S. mansoni infection, 7/24 had focal segmental glomerulosclerosis and 4/24 had membranoproliferative type I glomerulonephritis (including the patient with reported hepatosplenomegaly). This prevalence of focal segmental glomerulosclerosis is quite different from that reported in a study performed in 1973 (Brito 1973) using biopsies of patients with different clinical forms of schistosomiasis [Table III]. Membranoproliferative glomerulonephritis was the predominant pattern of renal lesion found by Brito (1973) in a group of patients with different clinical forms of schistosomiasis. Although these changes in the distribution of glomerular lesions may be the result of various biases related to the selection of subjects for biopsy, they may reflect actual changes in the pattern of distribution of glomerulopathies in the state of Bahia (BA), Brazil. The studies compared here all represent patients from the public general hospitals. Changes in the distribution of glomerular diseases have been associated with socioeconomic development in many studies (Ben Maiz et al. 2006, Gusbeth-Tatomir et al. 2006, Woo et al. 2010). A biopsy-based study from Romania found a higher prevalence of membranoproliferative glomerulonephritis in the most socioeconomically deprived areas of the country than in more socioeconomically developed areas (Gusbeth-Tatomir et al. 2006). It is interesting to note that, as shown in Table II, the average frequency of membranoproliferative glomerulonephritis remained stable, comprising 4% of the biopsies in the period between 2003-2009. However, the disease most commonly associated with this pattern of glomerulonephritis during that period was systemic lupus erythematosus. None of the 13 patients for whom serological tests for hepatitis B and C viruses were available had positive results for infection. Taken together, the data presented herein support the idea that the reduction in the occurrence of schistosomal glomerulopathy represents a change in the distribution of nephropathies in BA, toward a pattern similar to that observed in socioeconomically developed regions of the world (Korbet et al. 1996). ACKNOWLEDGEMENTS To Dr Zilton Andrade, for the suggestions to the manuscript. REFERENCES
Received 18 April
2011 Copyright 2011 - Memorias do Instituto Oswaldo Cruz The following images related to this document are available:Photo images[oc11179t2.jpg] [oc11179t3.jpg] [oc11179f1.jpg] [oc11179f2.jpg] [oc11179t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}