 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 89(1): 1-4, jan./mar. 1994
A Salmonella Agona Outbreak in a Pediatric Hospital in the City of Rio de Janeiro, BrazilMarise Dutra Asensi/+, Claude Andre Solari*, Ernesto Hofer* Laboratorio de Bacteriologia, Instituto Fernandes Figueira - FIOCRUZ *Departamento de Bacteriologia, Instituto Oswaldo Cruz, Av. Brasil 4365, 21045-900, Rio de Janeiro, R J, Brasil +Corresponding author Received 5 May 1993, Accepted 8 November 1993
Code Number: OC94001
Sizes of Files:
Text: 16K
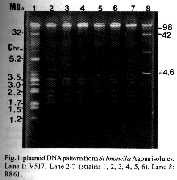
Graphics: Photos (Jpg)-9K / Halftones (Gif)-110K Six Salmonella Agona strains from an outbreak of 15 days duration which occurred in a public hospital in Rio de Janeiro, Brazil, were analyzed. The outbreak involved six infants (mean age, 24 days; mean body weight, 1612 g), all of them with severe clinical signs and symptoms. Two of them had surgical implications, two were preterm and two had respiratory distress at birth. The Salmonella strains were resistant to nine antimicrobial agents (ampicillin, cephalotin, ceftriaxone, gentamicin, amykacin, trimethoprim-sulfamethoxazole, chloramphenicol and tetracyclin). Analysis of the plasmid pattern of the wild strains and of the transconjugants confirmed that these were identical strains. Key words: Salmonella Agona - hospital infection - outbreak - antimicrobial resistance - plasmid pattern Hospital infections represent a serious medical problem, especially when they attack very young individuals such as newborns and infants up to six months of age (Erikson 1983, Jarvis 1987). Infants hospitalized in neonatal intensive care units or on surgical wards are the most vulnerable to infection because of a series of predisposing factors such as the intervention of broadspectrum antibiotics and the use of invasive procedures such as catheterization and intubation (Jarvis 1987). Among the Gram-negative bacteria most commonly involved in hospital infections in this age range are members of the family Enterobacteriaceae and of the genus Pseudomonas (Leonard et al. 1990). Since the participation of Salmonella is more rarely reported in the literature, in the present study we analyzed an outbreak of S. Agona infection of short duration which occurred in a public pediatric hospital in the city of Rio de Janeiro, RJ. MATERIALS AND METHODS Hospital and population description - The strains were isolated from six infants admitted to a public maternity-pediatric hospital (Fernandes Figueira Institute (IFF), FIOCRUZ, Brazilian Ministry of Health). Four of these infants were in the Neonatal Intensive Care Unit, one was on the Pediatric Surgery ward, and the other on the Pediatric Ward (Table I). Bacteriological methods - The strains were obtained from stools and blood cultures. The patbogen was isolated and identified by the method of Ewing (1972) and serological characterization followed the methods of Kauffmann (1954), and of Costa and Hofer,(1972). Serovar nomenclature is that of Le Minor (1988). Specimens were analyzed for susceptibihty to antimicrobials by disk diffusion on solid medium as recommended by National Committee for Clinical Laboratory Standards CNCCLS 1984). The discs (Cecon) were used at the following concentrations: ampicillin (Ap) - 10mcg; cephalotin (Cf) - 30 mcg; cefoxitin (Cx) - 30 mcg; cefriaxone (Cro) - 30 mcg; cefotaxime (Cft) - 30 mcg; pefloxacin (Pe) - 5 mcg; gentamicin (Ge) - 10 mcg; amykacin (Am) - 30 mcg; trimethoprim/sulfametoxazole (TSx) - 1.25/ 23.75 mcg; chloramphenicol (Cl) -30 mcg; tetracyclin (Te) - 30 mcg; nalidixic acid (NA) 30 mcg. Determination of the presence of R factors Cultures of S. Agona and of the receptor strains Escherichia coli K12 F^-, Lac^+ and Nal^r (originally from the Biophysics Institute, Federal University of Rio de Janeiro) were incubated at the 1:10 inoculum proportion at 37 C for 18 hr. Transconjugants were plated onto Agar McConkey, with the antimicrobial drugs added individually at the following concentrations: ampicillin, 10 mcg/ml- gentamicin- 10 mcg/ml; ceftriaxone - 16 mcg/ml. All plates contained nalidixic acid at the concentration of 30 mcg/ml. The growth of lactose-positive colonies (transconjugants) indicated the transfer of resistance markers. This result was confirmed by an antibiogram of the transconjugants, considering the original pattern of the corresponding donor colony. Plasmid DNA characterization - Plasmid DNA was extracted from the wild strains by the method of Birnboim and Doly (1979), modified by Sambrook et al. (1989). Electrophoresis on 0.8% agarose was at 40 V for 2 hr and 30 min in a 7.5-cm long cuvette in Tris-borate buffer. The plasmid DNAs of the E. coli strains R861 and V517 were included as molecular weight standards (Macrina et al. 1978, Threlfall et al. 1986). DNA was also extracted from the transconjugants in order to determine the conjugant plasmids. These experiments were repeated three times, and for the determination of the plasmid molecular weight we considered the average of the three electrophoretic runs. RESULTS The outbreak of S. Agona in the hospital areas was first recognized from a coproculture of patient 1 (RPS) who had been admitted on the preceding day (13 October) with signs and symptoms of bronchiolitis and diarrhea. In the remaining patients, Salmonella was detected, on average, after three days of hospitalization by bacteriologic analysis (fecal or blood cultures). The last specimen was collected on 29 October. Table I lists the relevant characteristics observed in the hospitalized infants who later on acquired S. Agona infection. Patient age ranged from five to 50 days (mean, 24 days) and birth weight ranged from 920 to 2380 g (mean, 1612 g). The major cause of hospitalization was a severe clinical picture for all patients: two of them (patients 2 and 4) had immediate surgical implication, two (patients 3 and 5) were preterm, low body weight infants with perinatal respiratory distress who were submitted to early antimicrobial treatment. The sixth child had osteomyelitis and was submitted to invasive procedures associated with the use of antimicrobial agents. Four of the six infants developed septicemia due to S. Agona, and one of them (patient 2) died on the seventh day of life. Analysis of the isolated strains (Table II) for susceptibility to the twelve antimicrobial agents used showed that five strains were resistant to nine drugs, differing from the strains from patient 2 by the absence of resistance to tetracyclin. All strains transferred the resistance markers of ampicillin, gentamicin and ceftriaxone, with contransfer of cephalotin and tetracycline markers also occurring in strains nos. 1, 3, 4, 5 and 6 and of the cephalotin and chloramphenicol markers in strain no. 2. Analysis of plasmid pattern (Fig. 1, Table III) revealed plasmid bands with molecular weights of 65, 5.8, 5.0, 3.8, 3.5, 3.3, 3.1, 3.0, 2.2, 2.0, 1.9, 1.7 MDa.
TABLE I
General clinico-pathological data on six patients with
salmonellosis (Salmonella Agona)
Patient Age Sex BW Cause of Ward Septiceaemia
(days) (g) admission
1 - RPS 50 M Diarrhea, PW -
bronchiolitis
2 - DSV 7 M 1900 Pulmonary and PSW +
renal agenesis,
cardiopathy
3 - NLS 5 F 1130 Prematurity, NICU +
respiratory distress
4 - PFS 40 M 2360 Pulmonary NICU/PSW -
adenomatoid lesion
5 - MBS 19 F 920 Perinatal NICU +
anoxia
6 - CBM 24 M 1730 Osteomyelitis NICU +
BW: birth weight; PW: pediatric ward; PSW: pediatric surgery
ward; NICU: neonatal intensive care unit
TABLE II
Antimicrobial resistance patterns and R factor of
Salmonella Agona strains isolated from hospitalized children
Markers
No. of strain Resistance patterns Transferred Cotransferred
1, 3, 4, 5, 6 Ap,Cf,Cft,Cro,Ge,Am, Ap,Ge,Cro Cf,Te
CI,TSx,Te
2 Ap,Cf,Cft,Cro,Ge,Am,
CI,TSx Ap,Ge,Cro Cf, CI
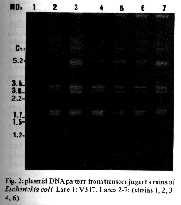
TABLE 111
Plasmid DNA patterns of Salmonella Agona isolates and
respective transconjugants
No. of Plasmid DNA patterns
strains (MDa)
1,3,4,5,6 65 5.8 5.0 3.8 3.5 3.3 3.1 3,0 2.2 2.0 1.9 1.7
2 65 5.8 5.0 3.8 3.5 3.3 3.1 3.0 - 2.0 1.9 1.7
Transconjugants 65 5.8 5.0 - - - 3.1 3.0 - - 1.9 1.7
(1,2,3,4,5,6)
Fig. 1:plasmid DNA pattern from Salmonella Agona isolates. Lane 1: V517. Lane 2-7 (strains 1, 2, 3, 4, 5, 6). Lane 8: R861. Fig. 2:plasmid DNA pattern from transconjugant strains of Escherichia coli. Lane 1:V517. Lanes 2-7: (strains 1, 2, 3 4, 6). The plasmid pattern of the transconjugants (Fig. 2) revealed the transfer of seven plasmids including one of high molecular weight (65 MDa). DISCUSSION The IFF is a public maternity-pediatric hospital with 120 beds, of which half are destined to the care of children with severe infectious or noninfectious conditions. In routine surveys carried out at the hospital for the control and prevention of hospital infection, the following microorganisms are usually detected: Klebsiella pneumoniae, Staphylococcus aureus, and Pseudomonas aeruginosa. These data fully agree with those obtained in other investigations (Jarvis 1987, Abrahamsen et al. 1989, Leonard et al. 1990, Hambreus et al. 1991). The outbreak discussed here is the first report of an infection provoked by S. Agona in this hospital. Indeed, this serovar occupies an outstanding position in Brazil in the enteric and/ or systemic processes affecting hospitalized children and children treated at outpatient clinics (Pessoa et al. 1978, 1980, Schwantes et al. 1983, Solari et al. 1986, Leal et al. 1988). This S. Agona outbreak probably resulted from the high vulnerability of the infants due to their exceptionally severe primary processes which favored dissemination of the bacterium. Highs, among the risk factors (Table I), are age and low body weight which are intimately associated with immunologic immaturity and with pathologic alterations in fundamental structures such as the pulmonary parenchyma. Consequently, invasive clinical and surgical procedures are used in the treatment of these basic diseases (nasogastric and endotracheal tubes, intravascular catheters and broad-spectrum antibiotics). These procedures and manoeuvres are predisposing factors favouring the implantation and propagation of a microorganism (Erikson 1883, Jarvis 1987, Leonard et al. 1990). From a bacteriological viewpoint, one of the basic properties enabling a bacterium to become an infectious agent in a hospital is clearly its pattern of antibiotic resistance. In the present case, the data listed in Table II show that almost all the S. Agona strains were multiresistant. Supporting this statement, R plasmids, which code for resistance and have the ability to transfer it, were detected in all strains. An unusual feature was the absence of resistance to tetracyclin in strain no. 2, perhaps as the result of loss of the plasmid coding for this marker, or indicating that this bacterial strain represents another clone. Analysis of plasmid pattern (Figs 1, 2, Table III) confirmed the identify of the strains, except for the strain from patient 2 which did not have the 2.2 MDa band. We emphasize the absence of the plasmid of 2.2 MDa molecular weight in strain 2 (Fig. 1). Later studies will be undertaken to confirm whether this may be the plasmid coding for resistance to tetracyclin. The present study indicates S. Agona to be an important nosocomial pathogen in children with severe primary disease: microbiological identification and characterization remain an important epidemiological tool. ACKNOWLEDGEMENTS To Prof. Dr Luiz Carlos de Souza Ferreira and to Dr Jose Cavalcanti de Albuquerque Ribeiro Dias for genetic consultation and to Dr Frits Sutmoller for reviewing the paper. REFERENCES Abrahansen TG, Finne PH & Lingas E 1989. Flavobacterium meningosepticum infections in a neonatal intensive care unit. Acta Pediatr Scand 78: 51-55. Birnboim HC, Doly J 1979. A rapid alkaline extraction procedure for screening recombinant plasmid DNA. Nucl Acid Res 7: 1513-1523. Costa GA, Hofer E 1972. Isolamento e identificafao de enterobacterias. Instituto Oswaldo Cruz, Rio de janeiro, 120p. Erikson M 1983. Neonatal septicaemia. Acta Pediatr Scand 72: 1-8. Ewing WH 1972. Edwards and Ewing's identification of Enterobacteriaceae. 4a. ed. Elsevier. Hambreus A, Lagerqvist-Widh A, Zettersten U, Engberg S, Sedin G, Sjoberg L 1991. Spread of Klebsiella in a neonatal ward. Scand J Infect Dis 23: 189-194. Jarvis WR 1987. Epidemiology of nosocomial infections in pediatric patients. Pediatr Infect Dis 6: 344-351. Kauffmann F 1954. Enterobacteriaceae. 2a. ed. E. Munksgard, Conpenhagen, 382 p. Leal MC, Cavalcanti TIR, Silva MJB, Reis EMF, Solari CA, Hofer E 1988. Frequencia de enterobacterias patogenicas em processos diarreicos infantis na cidade do Recife, Pernambuco, Brasil. Mem Inst Oswaldo Cruz 83: 475-479. Le Minor L 1988. Typing of Salmonella species. Eur J Clin Microbiol Direct Dis 7: 214-218. Leonard EM, Van Saene HF, Shears P, Walker J, Tam PKH 1990. Pathogenesis of colonization and infection in a neonatal surgical unit. Crit Care Med 18: 264-269. Anacrina FL, Kopecko D J, Jones KR, Mayers D J, McCowan SM 1978. A multiple plasmid-containing Escherichia coli strain: convenient source of size reference plasmid molecules. Plasmid 1: 417-420. (NCCLS) - National Committee For Clinical Laboratory Standards 1984. Performance Standards For Antimicrobial Disk Susceptibility Tests. Approved Standard. NCCLS Publication M2-A3. Pessoa GVA, Irino K, Melles CEA, Calzada CT, Raskin M, Kano E 1978. Ocorrencia de bacterias enteropatogenicas em Sao Paulo. No septenio 1970-1976 I - 0 surto epidemico de Salmonella typhimurium em Sao Paulo. Rev Inst Adolfo Lutz 38: 107-227. Pessoa GVA, Suguimori RT, Irino K, Raskin M, Calzada CT 1980. Isolamento de enterobacterias patogenicas em bercarios do municipio de Sao Paulo. Rev lnst Adolfo Lutz 40: 107-127, 1980. Sambrook J, Fritsch EF, Maniatis T 1989. Molecular cloning: a laboratory manual, 2nd ed. p. 1.25-1.28. Cold Spring Harbor Laboratory, Cold Spring Harbor, N.Y. Schwantes I, Esteves JS, Hofer E 1983. Frequencia de sorotipos de Salmonella em dois hospitais pediatricos. Bol Saude (Porto Alegre) 16: 12. Solari CA, Reis EMF, Dias JCAR, Hofer E 1986. Resistencia antimicrobiana de Salmonella agona ofiundas de varias regioes do Brasil. Memn Inst Oswaldo Cruz 81: 7-14. Threlfall EJ, Rowe B, Fergunson JL, Ward LR 1986. Characterization of plasmids conferring resistance to gentamicin and apramycin in strains of Salmonella typhimurium phage type 204C isolated in Britain. J Hyg 97: 419-426. Copyright 1994 Memorias do Instituto Oswaldo Cruz. The following images related to this document are available:Halftone images[oc94001b.gif]Photo images[oc94001a.jpg] [oc94001b.jpg]Line drawing images[oc94001a.gif] |
| |||||||||

{kind=link}
{kind=link}