 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 89(1): 59-61, jan./mar. 1994
Achilea Lisboa Bittencourt/+, Dilson J Fernandes, Carlos Sampaio Filho, Edson Duarte Moreira Jr*, Terezinha T Ribeiro*, William Harrington Jr** Departamentos de Patologia e de Medicina Interna, *Laboratorio de Retrovirus, Hospital Universitario Professor Edgard Santos, Universidade Federal da Bahia, Rua Joao das Botas s/no, 40110-160 Salvador, BA, Brasil **Department of Hematology and Oncology, University of Miami, Jackson Memorial Medical Center, P.O. Box 016960 (D8-4), Miami, FL 33101, USA + Corresponding author Received 23 March 1993, Accepted 19 November 1993
Code Number: OC94011
Sizes of Files:
Text: 13.7
Graphics: Photos (Jpg) - 13.6K / Halftones (Gif) - 50K
A case of a 20-years-old black man from Salvador, Bahia with
HTLV-I associated T cell lymphoma is presented. In spite of
the absence of splenomegaly and leukemia, the patient had a
marked cephalic tumoral infiltration associated with axillary
tumors in a pattern not yet described in adult T cell
lymphoma. Peripheral blood involvement was observed later on
in the course of the disease. The patient underwent
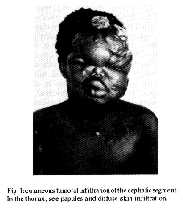
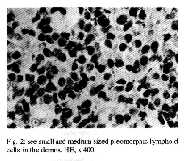
chemotherapy but died seven months after diagnosis.Key words: adult T cell lymphoma - HTLV-I - cutaneous T-cell lymphoma Acute adult T cell leukemia-lymphoma (ATLL) is a disease entity caused by human T cell leukemia virus type I (HTLV-I) (Lennert & Feller 1992). This lymphoma presents a rapid clinical course which often includes hepatosplenomegaly, lymphadenomegaly, hypercalcemia and the occurrence of peculiar leukemic cells with markedly pleomorphic and polylobulated nuclei. Interstitial pneumonitis may also be observed in ATLL (Can & Chen 1990). ATLL may also appear as a chronic-smoldering form in 30% of the cases. These forms are less agressive than the acute disease and characterized by skin lesions, low levels of circulating leukemic cells and absence of visceral involvement. The skin lesions appear as maculo-papular lesions, nodules or tumors, but less frequently erythrodermia may occur (Bunn et al. 1983). Higher numbers of circulating malignant cells occur in the chronic ATLL form than in the smoldering form. These cells have a highly lobulated nuclei. However, the chronic smoldering form of ATLL develops into the acute form of the disease within a period of several months (Can & Chen 1990). Peripheral blood involvement is seen in the majority of patients with ATLL, either initially or during the later course of the disease (Jaffe et al. 1984, Nagatani et al. 1990). ATLL has several histologic subtypes such as pleomorphic lymphoma with small cells, medium and/or large cells and immunoblastic lymphoma (Lennert & Feller 1992). The organs most frequently involved are lymph nodes, bone marrow, skin, liver, spleen and lungs. The skin in some series is involved in more than 60% of cases (Jaffe et al. 1984). Epidermotropism with Pautrier microabscesses imitating mycosis fungoides/Sezary syndrome is observed in two thirds of patients with cutaneous involvement. Sometimes circulating Sezary cells may also be observed (Jaffe et al. 1984). Thus the differential diagnosis between ATLL and mycosis fungoides/Sezary syndrome is sometimes impossible on histological grounds (Jaffe et al. 1984). However, the relationship between HTLV-I associated lymphoma and mycosis fungoides/Sezary syndrome is still the subject of contradictory reports (Bazaorbachi & Saal 1993, Hall 1993, Whittaker & Luzzatto 1993). The first cases of ATLL were described in areas of southern Japan. Since then many cases have been found in the Orient, Caribbean basin, northeastern South America and Central Africa (Can & Chen 1990). A few cases have also been observed from southeastern United States (Bunn et al. 1983). Recently, 14 cases of acute ATLL were described in Rio de Janeiro, Brazil, five of them being of African descent (Oliveira et al. 1990). The aim of this paper is to present the first case of HTLV-I associated ATLL observed in Bahia - Brazil, in a patient with marked skin infiltration. CASE REPORT A 20-years-old black man from Salvador, BA, was admitted with a one year history of weight loss and fever and rapidly growing cutaneous tumors in the last three months. The physical examination revealed a diffuse and marked skin thickening, mainly in the face and neck, assuming in many areas a tumoral pattern (Fig. 1). In addition, tumors measuring 8 cm were observed in both axillary regions. Desquamative skin with macules and papules was present throughout the trunk and upper limbs of the patient. Cervical and axillary lymph node enlargement was also detected. The remainder of the physical examination was within normal limits. Results of the blood count, kidney function tests and blood calcium level were normal. Urinalysis revealed 5 erythrocytes/field and the presence of protein (++). Chest X-ray showed no abnormalities. An abdominal ultrasound revealed a mild hepatomegaly and renal litiasis at left. No malignant cells were found either in the peripheral blood or the bone marrow. Fig. 1: cutaneous tumoral infiltration of the cephalic segment. In the thorax, see papules and diffuse skin infiltration. Fig. 2: see small and medium sized pleomorphic lymphold cells in the dermis. HE, x 400. Pathology - Biopsy of a skin tumoral lesion revealed a diffuse and marked infiltration on the dermis by pleomorphic medium sized cells with few small cells, involving the reticular and pappilar dermis (Fig. 2). The cells had a moderate amount of pale cytoplasm and nuclei with coarse chromatin and one prominent nucleolus. The nuclei show indentations, polylobulations and sometimes a cerebriform aspect. Few mitotic figures were observed. Frequently nuclear karyorrhexis was seen. The epidermis was slightly acanthotic and showed no epidermotropism. Biopsy of a papular lesion revealed a slight and focal infiltration of the same cells and a normal epidermis. The diagnosis was pleomorphic T cell lymphoma of medium cells (high grade lymphoma). Immunohistochemistry - Formalin fixed, paraffin-embedded tissue sections were studied by the avidin-biotin complex immunoperoxidase method (Hsu et al. 1981) using the following antibodies: CD30 (BerH2) and CD45RO (UCHL1). The neoplastic cells showed diffuse cytoplasmic staining for CD45RO and did not react with the CD30 antibodies. Serological assays - Serum sample was tested for antibodies to HTLV-I/II, using commercially available diagnostic enzyme immune assays (EIA) kits for screening (Coulter Labs., Hialeath, FL). The EIA-positive serum was then tested for HTLV-I by a new dot blot immunoassay using highly purified HTLV-I viral and recombinant proteins. The criteria of positivity for HTLV-I was the presence of antibodies to products of both the gag (p24) and env (p21e) genes. The sample was also tested to distinguish between HTLV-I and HTLV-II infection using a series of synthetic peptide-coated polystyrene beads in a solid phase immunoassay (Abott, Chicago, IL). Each peptide represented an area of 20 to 30 aminoacids from HTLV core or envelope region (Moreira Jr et al. 1993). The serological evaluation was made according to American Heath Services recommendations for laboratory techniques (Public Health Service Working Group, 1988). Evolution - The patient underwent chemotherapy according to the CHOP-Bleo regimen (Seiden & Canellos 1992). A partial regression of the tumors was observed and this protocol was repeated three, seven and eleven weeks after the beginning of treatment. A complete remission of cutaneous lesions was then observed. Two months later he returned with skin infiltration but without tumors. At this time, neoplastic cells were seen in the peripheral blood and bone marrow. The leukemic cells had pleomorphic and polylobulated nuclei. No cerebriform cells were seen. Additional chemotherapy was given but was not carried beyond the second week, however, due to severe thrombocytopenia. He died seven months after diagnosis and no autopsy was performed. DISCUSSION In ATLL, skin lesions begin as papules, nodules or plaques that become generalized within several months. Less frequently, ATLL manifests itself as erythrodermia simulating Sezary syndrome and the pre-mycotic phase of mycosis fungoides (Bunn et al. 1983, Jaffe et al. 1984). In the present case, in spite of the initial absence of leukemia and splenomegaly, the patient's condition was poor because of the marked skin infiltration. The cutaneous involvement was more marked than is generally referred in the literature, with the presence of tumoral cutaneous lesions and facial deformation simulating the tumoral phase of mycosis fungoides. The histological diagnosis was pleomorphic, medium sized T-cell lymphoma (high-grade malignant lymphoma) but no giant cells of the Sternberg-Reed and cerebriform types so often seen in ATLL (Lennert & Feller 1992) were observed in the present case. A differential diagnosis with the tumoral phase of mycosis fungoides was made on a histopathological basis because no epidermotropism and inflammatory cells were observed. Typical circulating pleomorphic and polylobulated cells different from the cerebriform cells of the Sezary syndrome were seen later on in the peripheral blood. It might be possible that other cases of malignant T cell lymphoma in Bahia are associated with HTLV-I. Epidemiological surveys carried out in this state have demonstrated a high prevalence of this infection either in the general population (1.1-2.3%) or in cases of tuberculosis in a general hospital that attends to lower income groups in Salvador - BA (11.1-28.6%) (Moreira et al. 1993). Tropical spastic paraparesis have also been described in Salvador - BA (Meireles et al. 1992). A large epidemiological study is warranted to define the extent of HTLV-I infection in Bahia. ACKNOWLEDGEMENTS To Gary Toedter from Coulter Immunology, Miami FL, for providing diagnostic EIA kits for screening HTLV-I/II antibodies; to Priscilla Swanson from Abbott Laboratories, Chicago, IL, to Prof. Fernando Schmitt from Fac. Med. Botucatu, UNESP - Sao Paulo, for performing the immunohistochemistry studies and to Miss Irani Abreu for her secretarial assistance. REFERENCES Bazarbachi A, Saal F 1993. HTLV-I Provirus and mycosis fungoides. Science 259: 1470-1471. Bunn PA, Schechter GP, Jaffe E, Blayney D, Young RC, Mattews MI, Blattner W, Broder S, Robert-Guroff M, Gallo RC 1983. Clinical course of retrovirus-associated adult T-cell lymphoma in the United States. New Engl J Med 309: 257-264. Cann AJ, Chen ISY 1990. Human T cell leukemia virus types I and II, p 1501-1527. In B.N. Fields, D.M. Knipe Virology. Raven Press Ltd, New York. Hall WW 1993. HTLV-1 Provirus and mycosis fungoides. Science 259: 1471. Hsu SM, Raine L, Fanger H 1981. Use of avidin-biotin peroxidase complex (ABC) in immunoperoxidase techniques: a comparison of ABC and unlabelled antibody (PAP) procedures. J Histochem Cytochem 29: 477-580. Jaffe ES, Blattner WA, Blayney DW, Bunn JR. PA, Cossman J, Robert-Guroff M, Gallo RC 1984. The pathologic spectrum of adult T-cell leukemia/lymphoma in the United States. Am J Surg Pathol 8: 263-275. Lennert K, Feller AC 1992. Non Hodgkin's lymphomas. Springer-Verlag, Berlin, p 223. Meireles A, Moreira Jr ED, Moreno-Carvalho OA, Badaro R, Melo A 1992. HTLV-I associated myelopathy in Salvador (Northeastern Brazil). Arq Neuropsiquiat 50: 189-190. Moreira Jr ED, Harrington JR W, Ribeiro TT, Melo A, Brites C, Badaro R, Swanson P, Lee H 1992. HTLV-II and a new endemic area for HTLV-I in Brazil. Rev Soc Bras Med trop 25: 141-143. Moreira Jr ED, Ribeiro TT, Swanson P, Sampaio Filho C, Melo A, Brites C, Badaro R, Toedter G, Lee H, Harrington Jr WJ 1993. Seroepidemiology of human T-cell lymphotropic virus type I/II in Northeastern, Brazil. J AIDS 6: 959-963. Nagatani T, Matsuzaki T, Temoto G, Kim S, Baga N, Miyamoto H, Nakajima H 1990. Comparative study of cutaneous T-cell lymphoma and adult T-cell leukemia/lymphoma. Clinical, histopathologic and immunohistochemical analyses. Cancer 66: 2380-2386. Oliveira MSP, Matutes E, Famadas LC, Schulz TF, Calabro ML, Nucci M, Andrada-Serpa MJ Tedder RS, Weiss RA, Catovsky D 1990. Adult T-cell leukemia/lymphoma in Brazil and its relation to HTLV-I. Lancet 336: 987-989. Public Health Service Working Group (FDA/CDC/NIH) 1988. Licensure of screening tests for antibody human T lymphotropic virus type I. Morbid Mortal Weekly Rep 37: 736-747. Seiden MV, Canellos GP 1992. Non Hodgkin's lymphoma infavorable disease chemotherapy, p 339-345. In MC Brain, PP Carbonne, Current Therapy in Hematology Oncology. BC Decker, Philadelphia. Whittaker SJ, Luzzato L 1993. HTLV-I Provirus and Mycosis Fungoides. Science 259: 1470. Copyright 1994 Memorias do Instituto Oswaldo Cruz.
The following images related to this document are available:Halftone images[oc94011b.gif] [oc94011a.gif]Photo images[oc94011a.jpg] [oc94011b.jpg] |
| |||||||||

{kind=link}
{kind=link}