 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Human Papillomavirus Detection in Genital Lesions by in Situ Hybridization and Ultrastructural ObservationsLHS Oliveira (/ +), ICPP Frugulhetti, MRL Passos, SMB Cavalcanti, MEF Fonseca (*)
Code Number: OC94040
Size of Files:
Text: 25K
Graphics: Photographs (Jpg) - 194K / Halftones (Gif) - 158K
Departamento de Microbiologia e Parasitologia, Instituto Biomedico, Universidade Federal Fluminense, Rua Prof. Ernani Melo 101, 24210-030 Niteroi, RJ, Brasil * Setor de Microscopia Eletr& circ;nica, Instituto de Microbiologia, UFRJ, Ilha do Fundao, 21944-970 Rio de Janeiro, RJ, Brasil
Detection of papillomavirus DNA in situ hybridization technique was performed in 29 symptomatic patients (6 males and 23 females) during the period of 1989-1991 at the Clinic for Sexually Transmitted Diseases, Universidade Federal Fluminense, State of Rio de Janeiro. All the male patients had condyloma acuminata. Only HPV 6/11 were found in these lesions. Clinical features in the female patients included vulvar condyloma acuminata, bowenoid papulosis, flat cervical condyloma, cervical condyloma acuminatum and cervical intraepithelial neoplasia grade II (CIN II). We also found cases of condyloma acuminata associated to vulvar intraepithelial neoplasia grade III (VIN III), as well as to vaginal invasive carcinoma. HPV 6/11 and 16/18 were found in vulvar condyloma acuminata. Mixed infection by 6/11-16/18 HPV were also seen in these lesions as well as in the patient who had cervical condyloma acuminatum. HPV 16/18 were found in the condyloma acuminatum plus VIN III and in the CIN II lesions. We have found HPV 31/33/51 in the specimen of condyloma acuminatum plus invasive carcinoma.
In order to investigate the ultrastructural aspects of HPV infection in genital tissue, the biopsies of three female patients were observed under electron microscope. Mature virus particles were found in the cells of a condyloma acuminatum as well as in the condyloma acuminatum plus invasive carcinoma case. In another sample, chromosome breakages were found in the nuclei of the infected cells although no viral particles were observed.
Key words: papillomavirus - viral ultrastructure - in situ hybridization
Human papillomavirus (HPV) infections of the genital tract are common sexually transmitted diseases. HPV 6, 11, 16 and 18 are the most usual types associated with genital lesions based on their frequent detection in either benign condylomas or cervical intraepithelial neoplasia (CIN) and genital carcinomas. It has been shown that HPV types 16 and 18 are found strongly associated with malignant tumors (Durst et al. 1983, McCance et al. 1985) while HPV 6 and 11 are almost exclusively found in benign lesions (Gissmann et al. 1984).
Several authors suggested that cells harbouring HPV types 16 and 18 are submitted to a higher risk of becoming malignant than those containing HPV 6 and 11 (Crum et al. 1984, Schneider et al. 1985). These data are in contrast with those of Hallan et al. (1991) which found HPV 16 and 18 as the most common types in 131 asymptomatic women. HPV 31, 33 and 51 have been associated with anogenital carcinoma and mild dysplasia (Lorincz et al. 1986, Fuchs et al. 1988, Nuovo et al. 1988).
The condyloma lesions may be florid and exophytic (condyloma acuminatum) or flat condyloma. In males, condyloma acuminata occurs on the penis, around the anus, on the perineum, and, more rarely, on the scrotum. In the female, they involve the vaginal introitus, the vulva, the perineum, the anus and rarely the cervix. The exophytic condyloma can be found with moderate and severe dysplasia in the same tissue. In the cervical neoplasias, tissues showing lesions with high-grade severity frequently have contiguous areas with mild condilomatous lesions (Saito et al. 1987).
Typing HPV requires nucleic acid hybridization studies. In situ hybridization test can be used to detect the HPV type in topographic relation to the pathologic characteristics of the lesion.
HPV particles have been shown in approximately 50% of the cases of condyloma acuminatum in the external genital tract (Oriel & Almeida 1970). They are usually identified in the nuclei of koilocytic cells and also occasionally in non- koilocytic cells. No particle is found in CIN III (severe dysplasia) and in cervical invasive carcinoma. However, HPV particles can be de-monstrated in cervical epithelium without cyto-pathic effects due to HPV (Syrjanen et al. 1985).
This research was undertaken to verify the presence of HPV in different lesions associated with these virus from patients who attended a Clinic of Sexually Transmitted Diseases (STD). Ultrastructural features about the development of papillomavirus particles in the infected cells are also reported.
MATERIALS AND METHODS
Study population - The study group comprised 29 patients (6 males and 23 females) attending the STD Clinic at the Universidade Federal Fluminense during the period of 1989-1991. The average age of the group was 25 years, with a standard deviation of three years. All the males had penile exophytic condyloma. The females showed vulvar condyloma (15), bowenoid papulosis (2), flat cervical condyloma (2), cervical condyloma acuminatum (1), CIN II (1), condyloma acuminatum plus vaginal invasive carcinoma (1), and condyloma acumi-natum plus VIN III (1). Biopsy specimens were taken from female lesions during colposcopy and from males during clinical analysis.
Histological diagnosis - The biopsies were fixed in 10% buffered neutral formalin, embedded in paraffin wax and stained with haematoxylin and eosin (HE) for histological evaluation. Histological grading of the intraepithelial lesions into mild (grade I), moderate (grade II), and severe dysplasia or carcinoma in situ (grade III) was performed according to the following criteria: (a) loss of organization of the epithelium in three layers, (b) disorderly arrangement of cells, (c) presence of koilocytosis, (d) binucleation or multinucleation, (e) nuclear atypia, (f) disturbed nuclear/cytoplasm ratio, (g) abnormal mitosis.
Tissue processing for hybridization - Paraffin embedded sections (5 um) of all biopsies were placed on slides previously treated with aminopropyltriethoxysilane (Sigma, St. Louis, MD, USA) and fixed for 60 min at 60 oC, deparaffinized and hydrated by sequential immersion in xylene, ethanol and deionized water. The unmasking of the target DNA was performed with proteinase K (250 ug/ml) for 15 min at 37 oC. In order to avoid any peroxidade activity in the tissue sections, the slides were treated with 3% hydrogen peroxide in 10mM phosphate buffer (PBS) containing 5mM EDTA. The slides were then dehydrated by sequential immersion in deionized water and ethanol, and dried for 30 min at 37 oC.
Hybridization procedure - The assay was performed using the Pathogene DNA Probe Assay (Enzo Diagnostics, New York, NY, USA) for identification of HPV types 6/11, 16/18 and 31/33/51 throughout biotinylated probes. Briefly, one drop of each probe was added to the test slides and to the controls. Then, the sections were covered with coverslips. The denaturation of DNA (probes and target) was performed on a heating block at 92 oC for 10 min. Hybridization was carried out at 37 oC for 30 min. Following hybridization, the coverslips were removed and the sections were washed with 40% formamide in PBS for 10 min at 37 oC. The slides were then incubated with streptavidin biotinylated horseradish peroxidase complex for 15 min at 37 oC, rinsed and incubated at 37 oC for 15 min with developing reagent containing 2% 3-amino-ethilcarbazole in solvent and hydrogen peroxide. Following the counterstaining with hematoxilin-eosin, the slides were mounted in water and observed under light microscopy with 40 X to 400 X magnification.
Electron microscopy studies - Specimens of genital lesions were taken from two patients who had condyloma acuminata and from one patient with condyloma acuminatum plus vaginal invasive carcinoma. The specimens were fixed in 2.5% glutaraldehyde (Merck) for 2 hr at room temperature. The material was then washed with cacodylate (Vetec, Sao Paulo, SP, Brasil) buffer, held 24 hr at 4 oC, dehydrated through a series of alcohols and embedded in Polylite Resin. The ultra- thin sections were stained with uranyl acetate and lead citrate, and then observed with a Philips 301 electron microscope.
RESULTS
The clinical and molecular data from the study group (29 cases) are summarized in Table. Of all cases, 21 (72%) were condyloma acuminata and 17 (58%) were positive for HPV DNA.
TABLE
Correlation of HPV type and histological analysis
============================================================
In situ hybridization
Legions No. of Positive HPV types
cases for HPV 6/11 16/18 6/11 31/33/
16/18a 51
Male patients
Penile condyloma acuminata 6 4 4 - - -
--------------------------------------------------------------------
Female patients
Vulvar condyloma acuminata 15 9 4 1 4 -
Bowenoid papulosia 2 - - - - -
Flat cervical condyloma 2 - - - - -
Cervical condyloma acuminatum 1 1 - - 1 -
CIN II 1 1 - 1 - -
Vulvar condyloma acuminatum
plus VIN III 1 1 - 1 - -
Vaginal condyloma acuminatum
plus invasive carcinoma 1 1 - - - 1
Total 23 13 4 3 5 1
-------------------------------------------------------------------
Total 29 17 8 3 5 1
===================================================================
Among men, condyloma was the only clinical manifestation detected. The only HPV types found among them were 6/11 (66%). Histopathological findings of these patients biopsies clearly showed koilocytic atypia in intermediate and upper epithelial layer. The two specimens found negative for HPV probes had clinical penile condyloma acuminata, but cytological changes (hyperplasia, hyperkeratosis and papillomatosis) were confined to a few areas of the tissue. In these biopsies, parakeratosis and koilocytosis were not found. Following therapy all male patients had remission of their warts and they have had no recurrence. Of the 32 women with HPV related lesions, a total of 15 (65%) had vulvar condyloma acuminata. Within these 15 cases, nine displayed HPV DNA. Out of them, four (44.4%) were positive for 6/11 type, four (44%) had presented mixed infection with both 6/11 and 16/18 types, and one (11%) was positive for 16/18 only. The six remaining specimens were negative for HPV and showed weak changes in the epithelial tissue, by histopathological analysis.
There were two cases of bowenoid papulosis and two of flat cervical condyloma. All of them were negative for the in situ hybridization technique.
Among the remaining cases, one biopsy of cervical condyloma acuminatum showed mixed infection with both HPV 6/11 and 16/18 types. One CIN II specimen was positive for HPV 16/18 as well as the case presenting vulvar condyloma acuminatum plus VIN III. The case of condyloma acuminatum plus invasive vaginal carcinoma was positive for HPV 31/33/51.
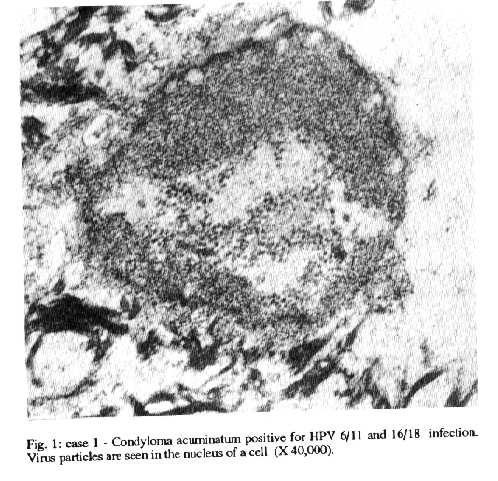
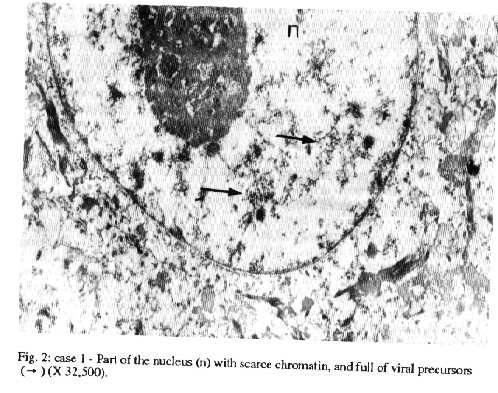
Electron microscopy - The first specimen studied was from a case of condyloma acuminatum positive for both HPV 6/11 and 16/18, by in situ hybridization (case 1). The cytological examination showed an extensive area with koilocytic atypia in intermediate and upper epithelial cell layers. Under the electron microscope, virus particles with 40 to 50 nm in diameter were found in the nuclei of the infected cells. These cells contained large clumps of chromatin which were mainly attached to the nuclear edges. Small aggregates of virus particles occurred in pseudocrystalline arrays or were scattered throughout the nucleoplasm, associated to or independent from the chromatin (Fig. 1). Mature and incomplete virus particles (35-50 nm) were detected in the nucleus of a cell presenting classical hallmarks of HPV infection. The nucleolus of this cell was strongly compact and the nucleus almost completely depleted of chromatin (Fig. 2). Some cells showed scanty nuclear chromatin and cytoplasmic degeneration.
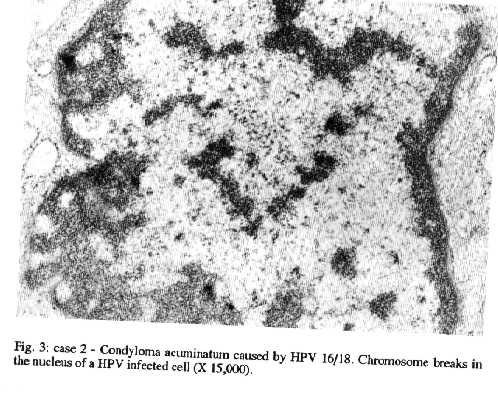
The second specimen was from a case of condyloma acuminatum caused by HPV 16/18 (case 2), as detected by in situ hybridization. Histological features showed koilocytic atypia followed by nuclear changes. Ultrastuctural studies revealed complete dearrangement of the cytoplasm and cytoplasmic organelles. Although mature viral particles were not found in this case, some cells exhibited chromosomes breakages in their nuclei (Fig. 3).
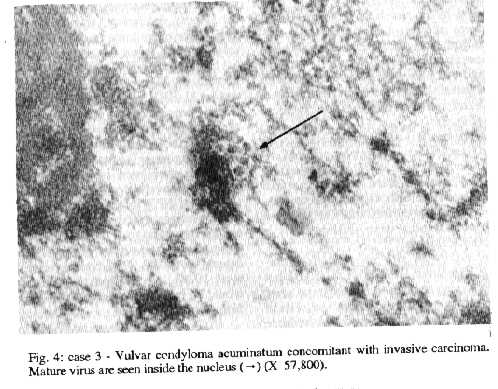
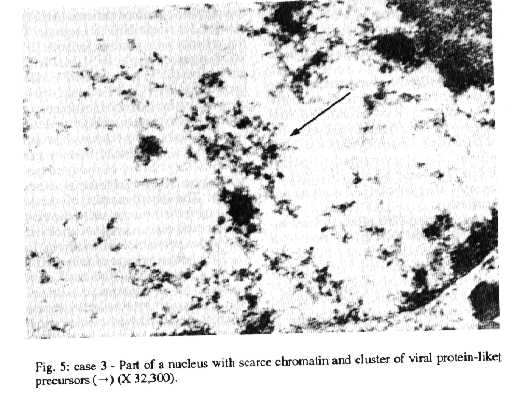
The last specimen was from a patient with vulvar condyloma acuminatum plus vaginal invasive carcinoma (case 3). The histological analysis of the warts revealed koilocytic atypia and binucleation in the cells of the upper and intermediate layer of the epithelium. The adjacent areas of the condyloma were infiltrated by a squamous cell carcinoma.
As detected by in situ hybridization, carcinoma cells harboured HPV DNA 31/33/51 but no HPV DNA was seen in the condyloma area. However, by ultrastuctural studies, a few cells of the condylomatous lesions showed mature viruses (Fig. 4). In one cell, cluster of virus protein-like precursors with 55nm in diameter was detected (Fig. 5). No viral particle was seen in the carcinoma cells.
DISCUSSION
This paper holds the first step of a survey concerning HPV infection carried out in the State of Rio de Janeiro.
In the last years, there has been an increasing detection of people showing lesions due to HPV infection not only in Rio de Janeiro, but worldwide. In order to diagnose and treat the clinical manifestations caused by this virus, the STD Clinic of the Universidade Federal Fluminense had introduced an attending that include colposcopy, histopathological analysis and HPV typing detection.
We had verified that 12% of all patients attending the STD Clinic during the period of 1989-1991 had HPV infection. During this period the number of female patients with clinical lesions by HPV was aproximately four times higher than the male patients, suggesting that these lesions are more frequent in women than in men. The latter, in general, only go to a STD Clinic when a visible and painful lesion occurs at the body, while women, besides this reason, visit the STD Clinic because they had been diagnosed or suspected of HPV-related conditions after the Papanicolau smear. Moreover, several authors have reported the difficulty in detecting subtle HPV infections in men (Rosemberg 1985, Sedlacek et al. 1986, Krebs & Schneider 1987). The detection of such lesions of the genital tract in women is easier because of the anatomical structure of the female genital tract.
Different lesions caused by HPV infection were detected, althoug the commonest one was condyloma acuminata, found in approximately 50% of the cases (nine females and six males). In male patients, condyloma were caused by HPV 6/11. In agreement, Rock et al. (1992) verified that 20 of 23 men with venereal warts had 6 and/or 11 HPV type. Since these types are considered non-oncogenic HPV, we suggest that, in accordance with the world literature (Pfister 1987, Fuchs et al. 1988), male patients had low risk of progression to malignancy.
In the two men negative for HPV DNA probes we have observed poor histopathological features of HPV infection. It is possible that the tissue sections tested did not present viral DNA or that it was in such a small copy number that was under the sensitivity of the method that only detects up to 200 DNA copies per cell (Syrjanen et al. 1988). It is also possible that these lesions would be infected by another HPV type different from the probes tested.
Unlike male patients, women had diverse clinical features of HPV infection, although condyloma acuminata has been prevalent. HPV DNA was detected in nine (60%) of these cases. Among the positive HPV DNA it was interesting to note that only four patients (44%) were found positive for single HPV 6/11 probe. The remaining patients were positive for both HPV 6/11 and 16/18 types or single HPV 16/18. Thus, in this group, five (55%) presented HPV 16/18. It is well known that HPV 16/18 are high risk types, that means, they are correlated with evolution of condyloma acuminata to malignant lesions. In this way, our study group has a high proportion of patients with a high risk to develop genital cancer and thus, they have to be followed periodically to verify possible progression of these lesions to cancer. The disappearance of the warts either resulting from the response to the treatment or by spontaneous regression has correlation neither to HPV types nor to mixed infections.
The high prevalence of mixed HPV infections was also observed by Villa and Franco (1989) in a survey in asymptomatic women in Brazil. Sexual promiscuity should favor reinfections by different types. Environmental and economical factors can also take place in the establishment of mixed infections. It is possible that some geographic areas are endemic to different types. Besides, the most part of the patients attended at STD Clinic live under poverty conditions. Poor higyene habits and the absense of medical care would be among causes of these observations.
We have reported a case of CIN II that was possibly a progression of a condyloma acuminatum acquired by the patient five years before. The patient was found positive for HPV 16/18 probes. This data is in agreement with the available literature (Syrjanen et al. 1985, 1988) and supports the idea of a higher relative risk to develop malignant lesions by the tissue cells infected with HPV 16 and 18. It is worth noting that during the period of progression, these patient showed many recurrences. The case of vulvar condyloma acuminatum and VIN III, a severe dysplasia, was also found positive for the 16/18 probes.
The case of vaginal condyloma acuminatum plus invasive carcinoma was the only found positive for 31/33/51 probe. It is remarkable that we did not find HPV DNA in the condylomatous tissue, but only in transformed cells. On the other hand, viral particles were found in these cells by electron microscope studies. It is possible that a HPV type other than HPV 31/33/51 has caused the condyloma. Further epidemiological studies have to be carried out in order to verify the relationship between HPV types and severity of the disease, as well as its clinical course.
Ultrastructure studies confirmed the difficulty in detecting HPV particles on genital tissue. In the first specimen analyzed, viral particles were detected only in a small amount of abnormal cells. In spite of Casas-Cordero et al. (1981) report that koilocytic atypia are not closely associated to the presence of the virus particles, we only found viral material in koilocytic cells. As seen in case 1, the compact nucleolus found indicates RNA synthesis. In accordance, viral precursors were found in this cell.
Viral particles are not found in the specimen of condyloma acuminatum caused by HPV 16/18. Besides, weak hybridization signals of HPV infection were observed in this case. It is reasonable to correlate this finding to sensitivity of the technique employed.
Chromosomes breakages were an interesting finding in this study. Although other viral infections may promote this pattern of cythopatic change, the available literature about HPV infection does not describe this feature for HPV infected tissues. These data suggest that besides altering the infected cell by inducing characteristic nuclear effects (enlargement, hyperchromasia, degeneration and pyknosis) HPV can cause cell damage in a particular way. These alterations were demonstrated in cells without virus particles, indicating that they are not directly associated to its presence inside the cell nucleus. Further studies will be required in order to get detailed information about this occurrence.
ACKNOWLEDGEMENTS
To Paulo Roberto Andrade Rios for technical assistance.
REFERENCES
Casas-Cordero M, Morin C, Roy M, Fortier M, Meisels A 1981. Origin of the koilocyte in study of condyloma of the human cervix. Ultrastructural study. Acta Cytol 25: 383-392.
Crum CP, Ikemberg H, Richart GM, Gissman L 1984. Human papillomavirus type 16 in early cervical neoplasia. New Engl J Med 310: 880- 883.
Durst ML, Gissman H, Ikemberg H, zur Hausen H 1983. A papillomavirus DNA from a cervical carcinoma and its prevalence in cancer biopsy samples from different geographic regions. Proc Natl Acad Sci 80: 3812-3815.
Fuchs PG, Girardi F, Pfister H 1988. Human papillomavirus in the normal, metaplastic, preneoplastic and neoplastic epithelia of the cervix uteri. Int J Cancer 41: 41-45.
Gissman L, Boshart M, Durst M, Ikemberg H, Wagner D, zur Hausen H, 1984. Presence of human papillomavirus in genital tumors. J Invest Dermatol 83: 26-28.
Hallan N, Green J, Gibson P, Powis J, Bibby J 1991. Prevalence of HPV cervical in a family planning clinic determined by polimerase chain reaction and dot-blot hybridization. J Med Virol 34: 154-158.
Krebs H, Schneider V 1987. Human papillomavirus-associated lesions of the penis colposcopy, cytology, and histology. Obstet Gynecol 70: 299-304.
Lorincz AT, Lancaster D, Temple GF 1986. Cloning and characterizaion of the DNA of a new human papillomavirus from a women with dysplasia of the uterine cervix. J Virol 58: 225-229.
McCance DJ, Campion MJ, Clarkkson PK, Chesters PM, Jenkins D, Singer A 1985. Prevalence of human papillomavirus type 16 DNA sequences in cervical neoplasia and invasive carcinoma of the cervix. Br J Obstet Gynecol 92: 1101-1105.
Nuovo GJ, Crum CP, de Villiers EM, Levine RV, Silverstein SJ 1988. Isolation of a novel human papillomavirus (type 51) from a cervical condyloma. J Virol 62: 1452-1455.
Oriel JD, Almeida JD 1970. Demonstration of virus particles in human genital warts. Br Ven Dis 46: 37-42.
Pfister H 1987. Human papillomavirus and genital cancer. Adv Cancer Research 48: 113-147.
Rock B, Keert VS, Farmer ER 1992. A morphologic, pathologic, and virologic study of anogenital warts in men. Arch Dermatolol 127: 495-500.
Rosemberg SK 1985. Subclinical papilloma viral infection of male genitalia. Virology 20: 554-557.
Saito K, Saito A, Fu YS, Smotkin D, Gupta J, Shah KV 1987. Topographic study of cervical condyloma and intraepithelial neoplasia. Cancer 59: 2064-2070.
Schneider A, Kraus H, Schuman R, Gissman L 1985. Papillomavirus infection of the lower tract: detection of viral DNA in gynaecological swabs. Int J Cancer 35: 443-448.
Sedlacek TV, Cunnane M, Carpiniello V 1986. Colposcopy in the diagnosis of penile condyloma. Am J Obstet Gynecol 1: 494-496.
Syrjanen K, Varynen M, Hippelainen M, Castren O, Sarikoski S, Mantiarvi R 1985. Electron microscope assessment of cervical neoplasia punch biopsies in women followed-up for human papillomavirus (HPV) lesions. Arch Geschwulsforsch 55: 131-138.
Syrjanen S, Partanen P, Mantyjarvi R, Syrjanen K 1988. Sensitivity of in situ hybridization techniques using biotin and 35S- labeled human papillomavirus (HPV) DNA probes. J Virol Methods 19: 225-228.
Villa LL, Franco ELF 1989. Epidemiologic correlates of cervical neoplasia and risk of human papillomavirus infection in asymptomatic women in Brazil. JNCI 81: 332-340.
Copyright 1994 Fundacao Oswaldo Cruz - FIOCRUZ The following images related to this document are available:Halftone images[oc94040e.gif] [oc94040c.gif] [oc94040a.gif] [oc94040d.gif] [oc94040b.gif]Photo images[oc94040e.jpg] [oc94040d.jpg] [oc94040b.jpg] [oc94040c.jpg] [oc94040a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}