 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memorias Instituto Oswaldo Cruz, Vol. 90(2):161-164 mar./apr. 1995 Treatment of Schistosomiasis: Gathering Stones Together JR Lambertucci, Departamento de Clinica Medica, Faculdade de Medicina da UFMG, Av. Alfredo Balena 190, 30130-100 Belo Horizonte, MG, Brasil
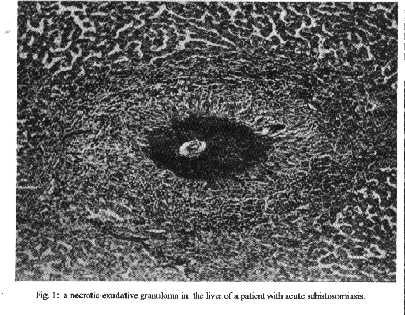
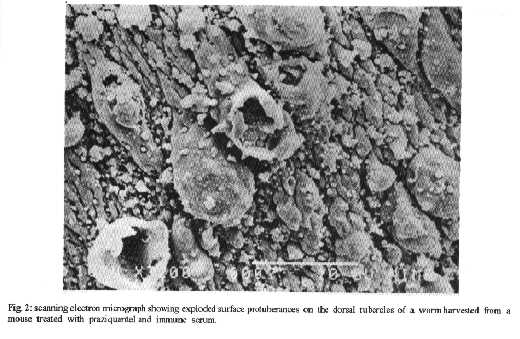
In this paper the treatment of schistosomiasis is examined under the following headings: cercarial dermatitis, Katayama fever, schistosomiasis in the immunosuppressed host and treatment of therapeutic failures. Key words: schistosomiasis - praziquantel - oxamniquine - corticosteroids CERCARIAL DERMATITIS Cercarial dermatitis results from incomplete infection by small mammal or avian schistosomes and occurs in immune populations from endemic areas following heavy reexposure to Schistosoma mansoni (Amer 1982). Schistosome dermatitis is difficult to distinguish from other forms of dermatitis. The lesions are commonly confused with those of contact dermatitis, poison ivy, scabies, impetigo, and insect bites. This stage also includes migration and development of the schistosomes and symptoms may start as early as two or three days after infection with fever, pulmonary symptoms (cough) and infiltrates, myalgia, abdominal pain, eosinophilia and moderate splenomegaly (Pedroso et al. 1984). The diagnosis of schistosomiasis at this stage is quite difficult. Treatment is usually not needed. Palliative topical agents, e.g., corticosteroids creams can be applied, and in severe cases, oral or parenteral antihistamines can be administered. There have been no clinical reports on the efficacy of schistosomicides at this stage but experimental work in mice supports the viewpoint that praziquantel, oxamniquine or steroids when given during the first week of infection, in the usual doses, are efficient in aborting the development of the worms (Coker 1957, Harrison & Doenhoff 1983, Sabah et al. 1986). TREATMENT OF ACUTE SCHISTOSOMIASIS (KATAYAMA FEVER) Four main approaches have been proposed for the treatment of acute schistosomiasis (Fig. 1): (1) Wait for the chronic stage - Due to the low efficacy of all schistosomicides in the toxaemic phase of schistosomiasis, it has been suggested that specific treatment should be postponed until the disease has entered its chronic stage (Lambertucci 1993); (2) Use of schistosomicides alone - Oxamniquine and praziquantel are potent schistosomicidal agents against mature Schistosoma mansoni (Lambertucci et al. 1982). They have also been used for the treatment of acute schistosomiasis. A reduced efficacy of these drugs against immature worms in experimentally infected mice has been demonstrated (Sabah et al. 1986). In at least two reports it has been shown that treatment with praziquantel alone aggravates the clinical picture of acute schistosomiasis (Harries & Cook 1987, Chapman et al. 1988). Schistosomicides alone should be given only to asymptomatic or pauci- symptomatic patients (Lambertucci et al. 1980); (3) Steroids alone - Mice experimentally infected with Schistosoma mansoni and treated with corticosteroids alone form incomplete granulomas around S. mansoni eggs and develop diffuse and severe hepatitis, and mortality is high in the infected group. Steroids should not be used alone in the treatment of acute schistosomiasis (Neves & Raso 1963); (4) Association of steroids and schisto- somicides - The association of steroids and schistosomicides in the treatment of acute toxaemic schistosomiasis augment cure rates, speed the recovery time (reducing the demand for inhospital treatment) and improve the quality of medical care (Lambertucci et al. 1989). THE IMMUNE DEPENDENCE OF CHEMOTHERAPY The number of people immunosuppressed by drugs (cytotoxic chemotherapy, other imunosuppressive agents including steroids and irradiation) or affected by diseases that cause immunodepression (AIDS, neoplasia, malnutrition, chronic renal failure) is growing fast. In the immunocompromised host there have been changes in the approach to most associated infectious diseases. Data on the behaviour of schistosomiasis mansoni in the immunosuppressed host are rather few (Hillyer & Cangiano 1979, Doenhoff et al. 1986, 1991, Hillyer & Climent 1988). Immunosuppressed individuals tend to have disseminated infection with S. mansoni (eggs) involving lung, liver, spleen, intestine, pancreas, and testis (Hillyer & Climent 1988, Lambertucci & Neves 1993). The migration of worms to different organs in the human body may explain the finding of a great number of eggs in unusual places. This hypothesis implies that the immune system is important in keeping the adult worms of S. mansoni confined to the mesenteric vessels. The efficacy of schistosomicides, in mice infected with S. mansoni and immunosuppressed by thymectomy and administration of rabbit anti-mouse thymocyte serum, is decreased. The schistosomicidal power of antimony, oxamniquine, and praziquantel is enhanced by passive transfer of immune serum simultaneously with drug administration to S. mansoni-infected mice, thus indicating a role for humoral immune effector mechanisms in this phenomenon (Brindley & Sher 1987, Lambertucci et al. 1989). Modha et al. (1990), using scanning and transmission electron microscopy, examined the immunodependence of praziquantel for the treatment of schistosomiasis mansoni in mice. The damage seen in male parasites harvested from mice that had been treated with praziquantel plus rabbit immune serum was more dramatic than that observed in worms from mice given either treatment alone (Fig. 2). Failure to respond to oxamniquine or praziquantel, in the usual doses, is to be expected in the immunocompromised host infected with S. mansoni. Most infections in patients with AIDS, for example, have been treated with higher doses of chemotherapeutic agents and they have also been given for longer periods of time. If it can be proven that the immune status of human patients influences the outcome of chemotherapy in the manner described for rodent models of schistosomiasis, there would be a strong case for the development of a vaccine that would enhance the efficacy of schistosomicidal drugs (Doenhoff et al. 1991). TREATMENT OF THERAPEUTIC FAILURES The approach to patients infected with S. mansoni who did not respond to previous treatment for schistosomiasis is still unsettled. In order to minimize the risk of the development of drug resistance, Katz and colleagues (1991) have suggested that infected patients should be treated with one drug, and therapeutic failures with another. Although isolated cases of oxamniquine resistance have been reported (Dias et al. 1982), a community with a serious problem of resistance has not yet been described. There are no similar reports for tolerance or resistance in S. mansoni infected individuals to praziquantel. Lambertucci and Carvalho (unpublished data) treated 220 children (ages 7 to 14), infected with S. mansoni in Brazil, with oxamniquine (20 mg/kg/body weight, single dose). Those children still passing eggs 1-3 months after therapy received oxamniquine again. Therapeutic failures were retreated three times during the following 9 months. Two successive quantitative stool examinations were performed after each treatment. Eight children presented viable eggs of the worm in their stools after the fourth treatment with oxamniquine. The percentage reduction in egg counts in children not cured was above 80%. Our data suggest that repeat treatment with oxamniquine is curative in most children infected with S. mansoni in Brazil. Other well-designed prospective studies are needed to define the best approach to therapeutic failures in patients with schistosomiasis mansoni. REFERENCES Amer 1982. Cutaneous schistosomiasis. Int J Dermatol 21: 44-46. Brindley PJ, Sher A 1987. The chemotherapeutic effect of praziquantel against Schistosoma mansoni is dependent on the host immune response. J Immunol 139: 215-219. Chapman PJC, Wilkinson PR, Davidson RN 1988. Acute schistosomiasis among British air crew. Brit Med J 297: 1101. Coker CM 1957. Effects of cortisone on immunity to Schistosoma mansoni in mice. Proc Soc Exp Biol 96: 1-3. Dias LCS, Pedro RJ, Deberaldini ER 1982. Use of praziquantel in patients with schistosomiasis mansoni previously treated with oxamniquine and hycanthone: resistance of Schistosoma mansoni to schistosomicidal agents. Trans R Soc Trop Med Hyg 76: 652-659. Doenhoff MJ, Hassounah O, Murare H, Bain J, Lucas S 1986. The schistosome egg granuloma: immunopathology in the cause of host protection or parasite survival? Trans R Soc Trop Med Hyg 80: 503-514. Doenhoff MJ, Modha J, Lambertucci JR, McLaren DJ 1991. The immune dependence of chemotherapy. Parasitol Today 7: 16-18. Harries AD, Cook GC 1987. Acute schistosomiasis (Katayama fever): clinical deterioration after chemotherapy. J Infect 14: 159-161. Harrison RA, Doenhoff MJ 1983. Retarded development of Schistosoma mansoni in immunosuppressed mice. Parasitol 86: 429-438. Hillyer GV, Cangiano JL 1979. Schistosoma mansoni granuloma in immunosuppressed man. Report of a case. Trans R Soc Trop Med Hyg 73: 331-333. Hillyer GV, Climent C 1988. Acquired Immunodeficiency Syndrome (AIDS) and parasitic diseases in Puerto Rico. Bol Asoc Med P Rico 80: 312-319. Katz N, Rocha RS, Souza CP, Coura Filho P, Bruce JI, Coles GL, Kinot GK 1991. Efficacy of alternating therapy with oxamniquine and praziquantel to treat Schistosoma mansoni in children following failure of first treatment. Am J Trop Med Hyg 44: 509-512. Lambertucci JR 1993. Acute schistosomiasis: clinical, diagnostic, and therapeutic features. Rev Inst Med Trop S o Paulo 35: 399-404. Lambertucci JR, Neves J 1993. Associac o Salmonella- Schistosoma-Mycobacterium: relato de um caso. Arq Bras Med 67: 53-54. Lambertucci JR, Greco DB, Pedroso ERP, Rocha MOC, Salazar HM, Lima DP 1982. A double blind trial with oxamniquine in chronic schistosomiasis mansoni. Trans R Soc Trop Med Hyg 76: 751-755. Lambertucci JR, Modha J, Curtis R, Doenhoff MJ 1989. The association of steroids and schistosomicides in the treatment of experimental schistosomiasis. Trans R Soc Trop Med Hyg 83: 354-357. Lambertucci JR, Modha J, Doenhoff MJ 1989. Schistosoma mansoni: the therapeutic efficacy of oxamniquine is enhanced by immune serum. Trans R Soc Trop Med Hyg 83: 362-363. Lambertucci JR, Pedroso ERP, Souza DWC, Lima DP, Neves J, Salazar HM, Marinho RP, Rocha MOC, Coelho PMZ, Costa MFFL, Greco DB 1980. The therapeutic efficacy of oral oxamniquine in the toxemic form of schistosomiasis: treatment of eleven individuals from two families and experimental study. Amer J Trop Med Hyg 29: 50-53. Modha J, Lambertucci JR, Doenhoff MJ, McLaren DJ 1990. Immune dependence of schistosomicidal chemotherapy: an ultrastructural study of Schistosoma mansoni adult worms exposed to praziquantel and immune serum in vivo. Parasite Immunol 12: 321-334. Neves J, Raso P 1963. Estudo critico do tratamento da forma toxemica da esquistossomose mansoni. Hospital 64: 167- 212. Pedroso ERP, Lambertucci JR, Rocha MOC, Greco DB, Ferreira CS, Lima DP, Raso P 1984. Pulmonary schistosomiasis: broncho- pneumonitis probably due to schistosomulae. Rev Soc Bras Med Trop 17: 213-215. Sabah AA, Fletcher C, Webbe G, Doenhoff MJ, 1986. Schistosoma mansoni: chemotherapy of infection of different ages. Exp Parasitol 61: 294-303.
Copyright 1995 Fundacao Oswaldo Cruz (Fiocruz)
The following images related to this document are available:Halftone images[oc95034a.gif]Photo images[oc95034b.jpg] [oc95034a.jpg]Line drawing images[oc95034b.gif] |
| |||||||||

{kind=link}
{kind=link}