 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memorias Instituto Oswaldo Cruz, Vol. 90(2):257- 260 mar./apr. 1995 Control of Schistosomiasis in Brazil: Perspectives and Proposals Jose Rodrigues Coura Departamento de Medicina Tropical, Instituto Oswaldo Cruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil
Code Number: OC95051
Size of Files:
Text: 25K
Graphics: Line Drawing (gif) - 11K
Photo (jpg) -23K / Halftone (gif) - 42K
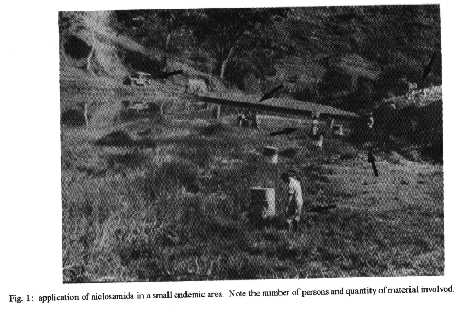
[TABLE AT END OF TEXT] Attemps to control schistosomiasis have hitherto involved the use of one or more of the following methods, either in isolation or in combination: (1) control of the intermediate host using molluscicides or biological methods; (2) basic sanitation and clean water supply; (3) health education; (4) individual or mass treatment; (5) protection of individuals in such a way as to prevent cercariae from penetrating the skin; (6) vaccine-based strategies against schistosomiasis. None of these methods is capable, on its own, of bringing about effective control of schistosomiasis, except in populations of a very limited size or under very special conditions. Molluscicides, besides expensive and toxic, have only a temporary effect. As for biological control, there is no effective method yet. Basic sanitation and clean water supply combined with health education potentially constitute the most effective approach, but only in the mid-to-long term. Mass treatment reduces morbidity, but does not control transmission. Protection of individuals has proved to be impraticable on a large scale. Vaccine-based strategies against schistosomiasis are still in the experimental stage. Experiments carried out in Brazil in the last 20 years have shown that mass treatment with single doses of oxamniquine or praziquantel can rapidly reduce levels of Shistosoma mansoni infection and morbidity in endemic areas. They have also shown that subsequent transmission and reinfection frequently occur in defined foci or "clusters", due to human contact with water, and in inverse proportion to the number and frequency of treatments carried out. On the basis of these experiments, the author suggests a multidisciplinary strategy for schistosomiasis control. Key words: schistosomiasis control - multidisciplinary strategy The control of schistomiasis is one of the most difficult tasks facing public health services in affected countries, owing to the world-wide spread of the intermediate host, its escape mechanisms in relation to existing control methods, the frequency of human contact with water, the dynamics of schistosomes transmission, the lack of sanitation and clean water supply for human populations and the limitations of individual and mass treatment/protection. Furthermore, the control of schistosomiasis using combined measures is very expensive and, to be effective, has to be maintained over the mid-to-long term. Protection of individuals in such way as to prevent cercariae from penetrating the skin will not be discussed in this paper, nor will vaccine-based strategies, because these methods are still in the very early experimental stages. Control of the intermediate host The observations made by Paraense et al. (1954) and Paraense (1955) 40 years ago concerning both re-invasion of breeding places by snails and the processes of self-and cross- fertilization in Biomphalaria glabrata led the identification of an important escape mechanism for these snails. The authors reported that many snails routinely buried themselves in the mud of their breeding sites up to a depth of 40 cm, and concluded that such snails remained unaffected by molluscicide treatment. Buried snails were found alive, and few days later were observed depositing self-fertilized eggs. It was discovered that within 90 days a single specimen of B. glabrata, under favorable conditions in terms of food and temperature, could produce 10 million individuals over three generations (Paraense 1987). In addition, Sullivan et al. (1984) demonstrated tolerance of some strains of B. glabrata to niclosamida and copper sulfate. Thus, these snails have shown to have at least two escape mechanisms against molluscicides. Fig.1 shows how many people and material are needed for a single molluscide campaign in a very restricted area. As well as being very expensive, a major desvantage of this method is that molluscicides require repeated application and have a number of environmental side-effects. The biological control of schistosoma vectors with microbial agents, parasites, predators and competitors has sometimes given satisfactory results in the laboratory, but has failed to deliver decisive gains in the field. The most effective biological agent against Schistosoma mansoni is Ribeiroia marini, described by Marin (1928) as Cercaria IV and redescribed by Faust and Hoffman (1934) under the name of Cercaria marini. It destroys the ovotestis of parasitized biomphalarias (Harry 1965), causing castration. Golvan et al. (1974) and Golvan (1978) observed natural R. marini infection in 90% of B. glabrata during the dry season in the island of Guadeloup, with a complete disapearance of the snails in some parts of the island. Combes et al. (1975) showed that the common rats Rattus rattus and Rattus norvergicus are the definitive host of C. marini in Guadeloupe, a finding confirmed by Nassi (1978). The latter carried out a field control study of B. glabrata involving dayly applications of laboratory rats faeces in specific foci (Nassi et al. 1979). Despite a significant decline in population, however, the snails reappeared in the following rainy season. Several competitors and predators, such as Pomacea lineata, Marisa cornuarietis, Helisoma duryi, Tilapia, etc., have been used in pilot snail control studies, sometimes leading to an inicially drastic reduction of population, but with disappointing final results (Paraense 1987). Basic sanitation and clean water supply in combination with health education
Basic sanitation and clean water supply combined with health education potentially constitute the most effective approach to schistosomiasis control, but only in the mid-to-long-term. The classic solution involving only basic sanitation and clean water supply would, in theory, be the most effective method, but it is very difficult and expensive to achieve such a solution in large endemic area, like in Brazil, that covers 1,000.000 km^2. This is a dream to come true in the next century. More simple methods of water supply and sanitation can reduce the prevalence and morbidity of schistosomiasis, but only in the long term and if associated with permanent health education programs. According to Pitchford (1958, 1972), in some parts of Africa where water was supplied for domestic purposes and other simple and relatively cheap measures were encouraged in order to reduce human contact with water, schistosomiasis infection rates were also declining progressively. In northeasthern Brazil, Barbosa et al. (1971, 1992) showed that schistosomiasis could be effectively controled with relatively limited intervention involving community-organized sanitation programs. The case of Saint Lucia, reported by Jordan et al. (1975), is very impressive because it shows that, with simple introduction of household water, a significant reduction in human contact with water can be achieved leading to reduce schistosomiasis prevalence and incidence. Finally, effective and permanent control of schistosomiasis will only be possible with changes in human behavior through health education, with the improvement of the basic social and economic standards of the involved communities and with enforcement by public health services, as occured in Japan, Puerto Rico and Venezuela. Individual and mass treatment Studies carried out in some endemic areas in Brazil have shown that specific chemotherapy for schistosomiasis, delivered either to individuals or in mass treatment campaigns, reduces the severity of the disease's clinical forms, and also that mass treatment can temporarily reduce the prevalence of infection (Kloetzel 1963, Bina 1977, Santos 1978, Katz et al. 1978, 1980). However, because of frequent re-infections in endemic areas, mass treatment, even when repeated several times, cannot completely control schistosomiasis (Katz et al. 1978, 1980, Coura et al. 1980, 1987, Prata et al. 1980, Santos & Coura 1986, Cutrim 1987, Cutrim & Coura 1992, Coura et al. 1992). As we can see in Figs 2, 3 from Coura et al. (1980, 1987), after the first mass treatment with oxamniquine there is a sudden drop in the prevalence of infection and in the egg load, but this is followed by rapid re-infection and egg load reconstitution, and even after five mass treatment an important residual infection remains. This problem occurred on a large scale in the Brazilian Special Program for the Control of Schistosomiasis, financed by the Ministry of health from 1976 onwards. Multidisciplinary strategy for schistosomiasis control: a proposal
On the basis of our field experience of schistosomiasis control in Brazil in the last 20 years, we propose the following tentative schedule for the short, mid and long term (Table). The Table can be summarized as follows: (1) in the short-to- mid term: mass treatment when prevalence is > 30% of the population, and selective treatment when 30%, together with use of molluscicides in transmission foci, during the dry season, in the 1st, 2nd, 3rd, 5th and 10th years; (2) in the mid-to-long term: water supply, sanitation and health education; (3) evaluation at the end of the 1st, 2nd, 3rd, 5th and 10th years; (4) follow-up for two more decades.
TABLE Schedule for schistosoxniasis control in short, mid and long term Measures Time (years) Ist 2nd 3rd 4th 5th 6th 7th 8th 9th 10th 20th 30th Nth Short/mid term Prevalence > 30% . Mass treatment x x x x x . Mollucicides x x x x x (Dry season) .Surveillance x x x x x Prevalence REFERENCES Barbosa FS, Coimbra Jr CEA 1992. Alternative approaches in the schistosomiasis control. Mem Inst Oswaldo Cruz 87 (Suppl. IV): 215-220. Barbosa FS, Pinto R, Souza O 1971. Control of schistosomiasis in a small northeast Brazilian community. Trans R Soc Trop Med Hyg 65: 206-213. Bina JC 1977. Influencia da terapeutica especifica na evoluc o da esquistossomose mansonni. Thesis. Univ. Fed. Bahia, 97 pp. Combes C, Eleger N, Golvan YJ 1975. Rats et bilharziose en Guadeloupe. Acta Tropica 32: 304-308. Coura JR, Argento CA, Conceic o MJ, Lewis WM, Santos ML, Magalh es P 1980. Experiencias de campo com oxamniquine oral no tratamento da esquistossomose mansoni. Rev Inst Med Trop S Paulo 22 (Suppl. 4): 77-84. Coura JR, Conceic o MJ, Santos ML, Mendonca MZG, Cutrim RNM 1992. Cross-sectional and evolutive studies of schistosomiasis mansoni in untreated and mass treated endemic areas in the southeast and northeast of Brazil. Mem Inst Oswaldo Cruz 87 (Suppl.IV): 175-182. Coura JR, Mendonca MZG, Madruga JP 1987. Tentativa de Avaliac o do Programa Especial de Controle da Esquistossomose (PECE) no Estado da Paraiba, Brasil. Rev Soc Bras Med Trop 20: 67-76. Cutrim RNM 1987. Aspectos clinicos-epidemiologicos da esquistossomose mansoni em tres localidades da Baixada Ocidental Maranhense. Thesis. Instituto Oswaldo Cruz 107 pp. Cutrim RNM, Coura JR 1992. Schistosomiasis in three localities of western lowlands of State of Maranh o before and after mass treatments. Mem Inst Oswaldo Cruz 87: 555- 558. Faust EC, Hoffman WA 1934. Studies on schistosomiasis mansoni in Puerto Rico. III. Biological studies. 1.The extra mammalian phases of the life cycle. Puerto Rico J Pulb Hlth Trop Med 10: 1-47. Golvan YJ 1978. Lutte biologique contre la bilharziose. Recherche 9: 486-489. Golvan YJ, Combes C, Bayssade-Dufour C, Nassi H 1974. Les cercaires de Ribeiroia marini (Faust et Hoffman, 1934), Trematode antagonist de Schistosoma mansoni et provoquant la castration du Mollusque-h“te, vecteur de la bilharziose humaine. C R Acad Sci Serie D 279: 405- 408. Harry HW 1965. Evidence of a gonodal hormone controlling the development of the accessory reproductive organs in Taphius glabratus (Say) (Gastropoda, Basommatophora), Abstr. Trans Am Microscop Soc 84: 157. Jordan P, Woodstock L, Unrau GO, Cook JA 1975. Control of Schistosoma mansoni transmission by provision of domestic water supplies. Bull WHO 52: 9-20. Katz N, Rocha RS, Pereira JP 1980. Schistosomiasis control in Peri-Peri (Minas Gerais, Brazil) by repeated clinical treatment and molluscicide application. Rev Inst Med trop S Paulo 22 (Suppl. 4): 84-93. Katz Z, Zicker R, Rocha RS, Oliveira VB 1978. Reinfection of patients in a schistosomiasis endemic area after specific treatment. I. Influence of age and worm burden. Rev Inst Med trop S Paulo 20: 273-278. Kloeztel K 1963. Sobre a conveniencia da quimioterapia da esquistossomose em populac es em continuo contato com focos (Nota previa). Rev Inst Med trop S Paulo 5: 106-110. Marin RA 1928. Studies on schistosomiasis (S. mansoni) in Puerto Rico. III. Cercariae from Planorbis guadeloupensis. Puerto Rico J Public Hlth Trop Med 3: 397-415. Nassi H 1978. Donees sur le cycle biologique de Ribeiroia marini guadeloupensis n.sp., Trematode sterilisant Biomphalaria glabrata en Guadeloupe. Entretien du cycle en vue d un controle eventuel des populations de Mollusques. Acta Tropica 35: 41-56. Nassi H, Pontier JP, Golvan YJ 1979. Bilan d'un essai de contr“le de Biomphalaria glabrata en Guadeloupe a l'aide d'un Trematode sterilisant. Ann Parasitol Hum Comp 54: 185-192. Paraense WL 1955. Self and cross-fertilization in Australorbis glabratus. Mem Inst Oswaldo Cruz 53: 285- 291. Paraense WL, Pereira O, Pinto DB 1954. Re-infection of breeding places by snails. Trans Roy Med Hyg 48: 540. Paraense WL 1987. Control of schistosomiasis mansoni: an outlook from current expectation. Mem Inst Oswaldo Cruz 82 (Suppl. IV): 1-12. Pitchford RJ 1958. Influences of living conditions of bilharziasis infection rates in Africans in the Transval. Bull WHO 18: 1088-1091. Pitchdord EJ 1972. Control of schistosomiasis in South Africa and Malagasy, p. 26-128. In MJ Miller Proceedings of the Symposium on the Future of Schistosomiasis Control. New Orleans, Tulane University. Prata A, Bina JC, Barreto AC, Alecrim MG 1980. Attempt to control the schistosomiasis transmission by oxamniquine in an hyper-endemic locality. Rev Inst Med trop S Paulo 22 (Suppl. 4): 65-72. Santos ML 1978. Esquistossomose mansoni. Estudo da morbidade e interferencia da terapeutica especifica em uma area endemica. Thesis. Univ. Fed. Rio de Janeiro, 97p. Santos ML, Coura JR 1986. Morbidade da esquistossomose mansoni no Brasil. IV. Evoluc o em pacientes tratados e seus controles. Mem Inst Oswaldo Cruz 81: 53-60. Sullivan JT, Cheng TC, Chen CC 1984. Genetic selection for tolerance to niclosamide and copper in Biomphalaria glabrata (Mollusca: Pulmonata). Tropenmed Parasitol 35: 189-192. Copyright 1995 Fundacao Oswaldo Cruz (Fiocruz)
The following images related to this document are available:Halftone images[oc95051a.gif]Photo images[oc95051a.jpg]Line drawing images[oc95051b.gif] [oc95051c.gif] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}