 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Memorias do Instituto Oswaldo Cruz Vol. 90(6), Nov./Dec. 1995 Prevalence of anti-Taenia solium Antibodies in Sera from Outpatients in an Andean Region of Ecuador Luis Escalante, Edwin C Rowland*, Malcolm R Powell*/+ Instituto Nacional de Higiene y Medicina Tropical, Quito, Ecuador *Department of Biological Sciences and the Tropical and Geographical Diseases Institute, Ohio University, Athens, Ohio, USA
Code Number: OC95146
Size of Files:
Text:
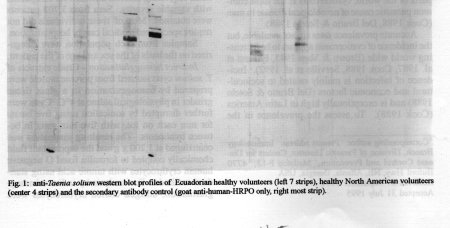
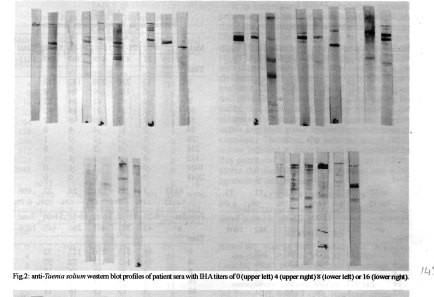
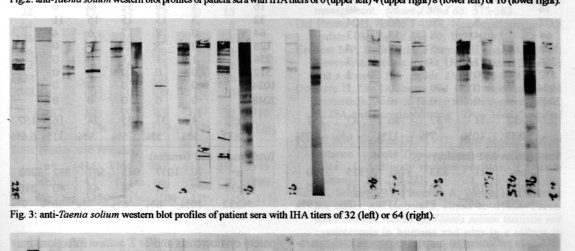
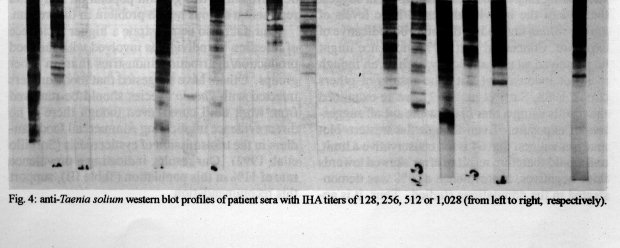
Graphics: Photos (jpg) - 103.3KSera from 9,254 individuals that presented at one of three outpatient clinics in Quito, Ecuador were assayed by indirect hemagglutination for the presence of antibodies reactive with antigens from Taenia solium cysts. Immunoblot analysis of 81 selected sera with IHA titers ranging from 0 to 1,028 showed that a titer of =/> 32 was suggestive of exposure to the parasite. Nine percent (9%) of the 9,254 patients had titers of 32 or greater. Of 3,503 sera from one clinic, which included sera from food handlers undergoing yearly physicals, 390 (11%) were positive. In addition, a correlation with age was seen in some, but not all, populations. In situations where age-related effects were noted, the highest incidence was seen in the youngest (0-20 years) and in the oldest (51-60 years) group. Thus, a resurgence of infection after a period of lower prevalence may be developing. Overall, this study shows that cysticercosis is relatively common and potentially a serious health problem in this region. Key words: Taenia solium - cysticercosis - serology - Ecuador Cysticercosis, caused by infection with the larval stage of Taenia solium has been described as both an ancient disease (Del Brutto & Sotelo 1988) and a modern day plague (Brown & Voge 1985). Humans are the definitive host for the adult tapeworm and eggs or proglottids are shed in the feces. Eggs can be ingested by swine where the metacestode stage (a cysticercus) encysts in the tissues, including but not limited to, muscle. Consumption by man of raw or undercooked pork containing cysts completes the life cycle. However, people can also be infected by the larval stage by egg consumption via the fecal-oral route. As in the porcine intermediate host, larval forms encyst in the muscle and also in the central nervous system which can lead to serious disease. In some parts of the world, cysticercosis is the most common parasitic cause of neurological disease in man (Cook 1988, Del Brutto & Sotelo 1988). Accurate prevalence rates are not available, but the incidence of cysticercosis appears to be increasing world wide (Brown & Voge 1985, Earnest et al. 1987, Cook 1988, Sorvillo et al. 1992). Incidence of infection is mainly related to sociocultural and economic factors (Del Brutto & Sotelo 1988) and is exceptionally high in Latin America (Cook 1988). To assess the prevalence in the Andean region of Ecuador, we performed a serological examination of 9,254 patients from three outpatient clinics in Quito, Ecuador. MATERIALS AND METHODS Patient populations - Sera were obtained from patients at three health care facilities in Quito, Ecuador. Samples (3,503) acquired from the Instituto de Higiene Municipal were from food handlers, grocery store owners and employees receiving required annual physicals. Patients (2,700) at the Instituto Nacional de Higiene y Medicina Tropical (INH) were also undergoing standard laboratory tests for general health screening and routine physicals. The IESS Social Security Institute is an outpatient clinical for ambulatory patients requesting medical attention for complaints with variable severity. Sera from 3,202 patients were obtained. Most of these individuals did not require specialized medical care or hospitalization. Samples from each population were categorized on the basis of the sex and age of the patient. Indirect hemagglutination - Crude extracts of T. solium cysts isolated from porcine muscle were prepared by homogenization in a glass tissue grinder in physiological saline at 4 C. Cysts were further disrupted by sonication using five bursts for min each on ice, with five min rests in between treatments. The resulting suspension was centrifuged at 1,200 x g and the supernatant fluid chemically coupled to formalin fixed O negative human erythrocytes with tannic acid using standard methods. For analysis by indirect hemagglutination, antigen coated erythrocytes were placed into the wells of microtiter plates (96 well) containing diluted patient serum and the anti-T. solium titer determined after 4 hr at 4 C. Western blot analysis - Western blot analysis was performed as previously described (Powell & Wassom 1993). Briefly, extracts of T. solium cysts were separated on 12% polyacrylamide gels and transferred electrophoretically to nitrocellulose. After blocking with 5% non-fat dry milk, strips of nitrocellulose were exposed to 1:100 dilutions of patient sera. Antigen-antibody complexes were visualized using peroxidase linked goat anti-human IgG (Tago Immunochemicals, Burlingame, CA) followed by incubation with a substrate/chromophore solution of H2O2/4-chloro-1-napthol. RESULTS Anti-T. solium indirect hemagglutination titers (IHA) in the sera of 9,254 patients are presented in Tables I-IV. Western blot analysis of 81 selected sera are shown in Figs 1-4. Samples used in immunoblot studies were chosen to represent the spectrum of IHA titers ranging from 0-1028. Antibodies in sera from some healthy controls do bind to T. solium antigens in the western blot assay used, but the frequency and patterns are low and inconsistent (Fig. 1). Similarly, patients with IHA titers of 0, 4, 8 or 16 also showed inconsistency with respect to the antigen-antibody profiles, but the number of bands detected was, in general, higher than those detected from control sera (Fig. 2). Both the frequency and intensity of bands detected was higher using sera from patients with IHA titers of 32 or 64 (Fig. 3). This was true to an even greater extent using sera from individuals with titers =/> 128 (Fig. 4). Based on qualitative analysis of these data (Figs 1-4) a cut off titer of =/> 32 was used as suggestive of infection. Table I shows the anti-T. solium IHA titers in the sera of 892 males and 1,808 females that reported to the INH in 1985. Of these, a total of 8.5% had titers =/> 32. Of 3,202 patients that presented at the IESS, 210 (6.6%) had titers of =/> 32 (Table II). Sera obtained from the Higiene Municipal (Table III) had the highest percentage with titers suggestive of exposure. Of 3,503 patient sera tested, 390 (11.1%) had titers =/> 32. Table IV summarizes the data presented in Tables I-III and suggests an overall exposure rate of 9% to T. solium in the populations examined. DISCUSSION Prevalence data for particular diseases are important for the establishment of appropriate diagnostic, therapeutic and prophylactic efforts and in determining national, regional and global health policy. We examined a large number of samples from both the general public and those with a wide variety of medical complaints around Quito and suggest a high and fairly consistent incidence of exposure to T. solium in this population. Sera obtained from 9,254 individuals in 1985 had anti-T. solium IHA titers ranging from 0 to 2,048. In an a posteriori attempt to determine a titer indicative of infection, western blot analyses of sera from selected patients, as well as those from healthy Ecuadorian and North American volunteers, were performed. Others have shown western blot analysis to be useful in the serodiagnosis of cysticercosis (Gottstein et al. 1987, Wilson et al. 1991). Qualitative examination of our results (Figs 1-4) suggested a titer of 32 or higher in the IHA was sufficient to suspect exposure to the parasite. Using this value as a cutoff, our data suggest that 9% of the individuals tested have levels of anti-T. solium antibodies that may be indicative of exposure. Concerned that a 9% incidence might be perceived as unrealistically high, even though it is not inconsistent with the results of others (Cook 1988, Sarti et al. 1992), we re-examined the results using a titer of 64 as the cut off suggestive of exposure. Even though the western blot analyses suggest that 64 is too conservative a limit, and would therefore result in error skewed towards false negatives, a prevalence of 6% was demonstrated in the populations studied. Thus, it is apparent cysticercosis and/or T. solium infections may be prevalent in this general population and could represent a serious health problem in this region. Our data also demonstrate a higher incidence of infection in individuals involved with the food production/distribution industries than in other groups. Others have suggested that food handlers infected with Taenia species should be removed from work until cured, even though there is no direct evidence implicating commercial food handlers in the transmission of cysticercosis (Sorvillo et al. 1992). Our results, indicating a prevalence rate of 11% in this population (Table III), support this recommendation. It is interesting that ambulatory patients presenting with medical complaints to the IESS clinic showed an infection rate associated with age (Table II). Within this population, the youngest group (0-20 years) and the oldest group (51-60 years) had the higher percentages of individuals with titers indicative of infection compared to individuals aged 21-50 years (p<0.003 by Chi Square analysis). The same pattern of age distribution and infection was seen in males, but not in females, that presented at the INH. Moreover, the present study does suggest that a number of people in this area have anti-T. solium titers indicative of exposure. Therefore, the potential exists for T. solium infection to cause significant morbidity in this particular geographical region and underscores the need for further evaluation and management of this disease.
TABLE I
Patients from Instituto Nacional de Higiene y Medicina
Tropical
Age groups
Males 0-10 11-20 21-30 31-40 Total
-------------------------------------------------------
n^= 98 327 334 133 892
Titer
-------------------------------------------------------
0 68 188 163 59
4 16 67 66 37
8 5 38 38 12
16 5 13 30 13
32 1 12 19 4
64 2 7 8 2
128 1 0 4 1
256 0 1 3 2
512 0 1 3 1
1024 0 0 0 0
2048 0 0 0 1
n=/> 32 4 21 37 12 73
%=/> 32 3% 6% 11% 9% 6.6%
---------------------------------------------------------
Females 0-10 11-20 21-30 31-40 Total
---------------------------------------------------------
n^= 113 506 807 382 1808
Titer
---------------------------------------------------------
ACKNOWLEDGEMENTS To Mrs Margarita Vela, MT, of the INH, Quito for expert technical assistance. REFERENCES Brown WJ, Voge M 1985. Cysticercosis. A modern day plague. Ped Clin N Am 32: 953-969. Cook GC 1988. Neurocysticercosis: parasitology, clinical presentation, diagnosis, and recent advances in management. Quart J Med 68: 575-583. Del Brutto OH, Sotelo J 1988. Neurocysticercosis: An update. Rev Infect Dis 10: 1075-1087. Earnest MP, Reller LB, Filley CM, Grek AJ 1987. Neurocysticercosis in the United States: 35 cases and a review. Rev Infect Dis 9: 961-979. Gottstein B, Zini D, Shantz PM 1987. Species-specific immunodiagnosis of Taenia solium cysticercosis by ELISA and immunoblotting. Trop Med Parasitol 38: 299-303. Powell MR, Wassom DL 1993. Host genetics and resistance to acute Trypanosoma cruzi infection in mice. I. Antibody isotype profiles. Parasite Immunol 15: 215-221. Sarti E, Schantz PM, Plancarte A, Wilson M, Gutierrez IO, Lopez AS, Roberts J, Flisser A 1992. Prevalence and risk factors for Taenia solium taeniasis and cysticercosis in humans and pigs in a village in Morelos, Mexico. Am J Trop Med Hyg 46: 677-685. Sorvillo FJ, Waterman SH, Richards FO, Shantz PM 1992. Cysticercosis surveillance: locally acquired and travel-related infections and detection of intestinal tapeworm carriers in Los Angeles county. Am J Trop Med Hyg 47: 365-371. Wilson M, Bryan RT, Fried JA, Ware DA, Schantz PM, Pilcher JB, Tsang VWC 1991. Clinical evaluation of the cysticercosis enzyme-linked immunoelectrotransfer blot in patients with neurocysticercosis. J Infect Dis 164: 1007-1009. +Corresponding author. Present address: Immunology Branch, Division of Parasitic Diseases, Centers for Disease Control and Prevention, Mailstop F-13, 4770 Buford Hwy, NE, Atlanta, Georgia, USA Received 27 September 1994 Accepted 31 July 1995 Copyright 1995 Fundacao Oswaldo Cruz, FIOCRUZ
The following images related to this document are available:Photo images[oc95146d.jpg] [oc95146c.jpg] [oc95146b.jpg] [oc95146a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}