 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Analysis of Mycobacterium avium complex serovars isolated from AIDS patients from southeast Brazil Maria Helena Feres Saad/^+, Veronique Vincent*, David J Dawson**, Laboratorio de Hanseniase, Instituto Oswaldo Cruz, Av. Brasil 4365,
21045-900 Rio de Janeiro, RJ, Brasil Received 4 December 1996
Code Number: OC97083
File Sizes:
Text: 20.6K
Graphics: Tables (jpg) - 84K
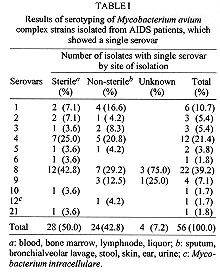
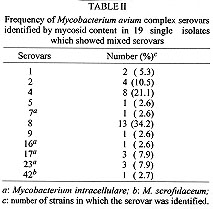
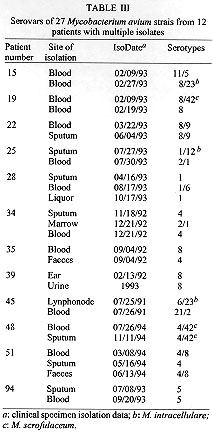
The purpose of this study was to assess the distribution of Mycobacterium avium serovars isolated from AIDS patients in Sao Paulo and Rio de Janeiro. Ninety single site or multiple site isolates from 75 patients were examined. The most frequent serovars found were 8 (39.2%), 4 (21.4%) and 1 (10.7%). The frequency of mixed infections with serovar 8 or 4 was 37.8%. Among the 90 strains examined, M. intracellulare serovars (7 strains) and M. scrofulaceum (4 strains) were found in 11 isolates (12%) indicating that M. avium (88%) was the major opportunistic species in the M. avium complex isolates in Brazilian AIDS patients. Key words: seroagglutination - serovars - mycoside C - glicopeptidolipids - Mycobacterium avium Non tuberculous mycobacteria belonging to the Mycobacterium avium complex (MAC) have been increasingly recognized as an important group of organisms causing severe opportunistic infection in patients with acquired immunodeficiency syndrome (AIDS) in the United States (Kiehn et al. 1985, Young et al. 1986, Horsburgh & Selik 1989, Nassos et al. 1991, Havlik et al. 1992), Europe (Yates et al. 1986, Wickman 1986, Peters et al. 1989, Grange et al. 1990) and Australia (Dawson 1990). In Brazil an increase in the frequency of M. avium complex infections has also been found associated with AIDS patients (Barreto et al. 1993, Landgraf et al. 1994). Recognition of the importance of MAC infection in AIDS has stimulated epidemiological studies concerning it. Most of the studies have been done in the USA, some in Europe; however none in Brazil. MAC may be typed by using a seroagglutina-tion assay described by Schaefer (1965). Currently the serovars 1 through 6, 8 through 11 and 21 are recognized as M. avium, 7, 12 through 28 as M. intracellulare while serotypes 41 through 43 are designated M. scrofulaceum. Serotyping is based on the presence of specific oligosaccharide haptens (Brennan & Goren 1979, Brennan et al. 1981, McNeil et al. 1987) that form the sugar moiety of glycopeptidolipids (GPL), located on the cell surface of smooth-colony-forming strains. Rough colony variants are not amenable for serotyping because they agglutinate spontaneously. However, their GPL can be extracted and analyzed by thin layer chromatography (TLC) procedures (Brennan & Goren 1979). Significant geographic differences have been reported in the major serotypes infecting AIDS patients (Kiehn et al. 1985, Horsburgh et al 1986). Furthermore, these serotypes infecting AIDS patients also differ from those predominantly infecting non-AIDS patients (Yakrus & Good 1990, Tsang et al. 1992). In order to examine the predominant serotypes infecting patients, we analyzed MAC strains isolated from AIDS patients combining both agglutination according to Schaefer (1980) and the nature of the GPLs identified by TLC. The MAC strains were isolated from Sao Paulo and Rio de Janeiro, where the rate of AIDS infection is the highest in Brazil (Ministerio da Saude 1996). MATERIALS AND METHODS Selected isolates - A total of 90 strains, isolated from clinical specimens from 75 AIDS patients, between 1991 and 1994, in the cities of Sao Paulo and Rio de Janeiro were studied. The strains were from the Instituto Adolfo Lutz in Sao Paulo (SP) (n=67), and from three different microbiology laboratories in Rio de Janeiro: Hospital Evandro Chagas (FIOCRUZ) (n = 7), Hospital Universitario Clementino Fraga Filho (UFRJ) (n = 4) and Centro de Referencia Professor Helio Fraga (Health Ministry) (n = 12), most of them being from Rio de Janeiro (RJ). Forty-seven strains were isolated from sterile sites (41 blood, 2 lymph nodes, 1 cerebrospinal fluid and 3 bone marrow), and 40 from non-sterile sites (29 sputum, 4 bronchialveolar lavage, 3 faeces, 3 urine and 1 ear), while three were from unknown sites. The isolates were identified by conventional biochemical tests. Twelve patients had multiples isolates (n = 27) from different body sites or from the same body site at different times. Specimen source and patient information were obtained from microbiology laboratory records. Serotyping - The smooth colonies were serotyped by direct agglutination following modified Schaefer's procedure (Schaefer 1980), using rabbit antisera raised against each member of the MAC (serovars 1-28) and M. scrofulaceum (serovars 41-43). The strain suspensions for serotyping were prepared as follows: the organisms were cultured on Lowenstein-Jensen medium incubated at 37 C for two weeks, or until heavy growth was obtained. The growth was harvested by scraping gently with loop and flooding into 1 ml of 0.5% phenol phosphate buffered saline (P-PBS). The suspensions were killed by heating at 80 C for 1 hr. After shaking, the suspensions were let stand for 1 hr to allow clumps to sediment and the heavily turbid supernatant was then used for serotyping. The serotyping procedure was performed in the Microbiology and Pathology Laboratory, Queensland Health, Brisbane, Australia. Thin layer chromatography - The extraction and preparation of the alkali-stable glyco-peptidolipid antigen from fresh growth were performed as described previously (Tsang at al. 1983), with minor modifications: the organisms were cultured as described above. The growth was heavily harvested by scraping gently with loop and mixed into 1.5 ml of chloroform-methanol 2:1, v/v (C:M) and the suspension was then heated overnight at 56 C. One hundred ul of the clear crude lipid extracts were then mixed with the same volume of methanol containing 0.2 M NaOH. The reaction was incubated at 37 C for 20 min, to saponify other complex lipids, then the reaction was acidified with 2.5 ul of acetic acid and dried. To the extract 500 ul of C:M and 100 ul of water were added. After 10 min of centrifugation, the aqueous phase was discarded and the extract was dried. The dried extract was solubilized in 30 ul of C:M, applied to silica gel TLC plates (HP-K, Merck, Germany) and then chromatographed using C:M:H2O (65:25:4) and C:M (80:20). The C-mycoside GPL antigens were revealed using the 0.2% solution of anthron in sulfuric acid spray reagent. Reference cultures of M. avium were used as the internal standard for each of the M. avium complex mycosides. RESULTS This is the first time that Brazilian MAC clinical isolates have been examined with respect to serotyping and mycoside content. Both procedures were applied to 39 strains; 8 (20.5%) were non-typeble (or autoagglutinated) by seroagglutination, but all strains could be typed by their characteristic GPL mycosides. Among 31 strains that were typed by both methods, there were 3 (9.67%) in disagreement. Although, there was good agreement between the two methods (90.4%) a large proportion of the strains were untypeble or autoaggluti-nated using seroagglutination, despite the presence of characteristic GPLs in all strains tested. Consequently, only the mycoside content was used in the following analysis of the data. Seventy-five patients yielded 90 isolates; 56 (62.2%) showed a single serovar (group I) while in 34 (37.8%) more than one serovar was identified (group II). The serovars identified from the first group of isolates are depicted in Table I. The predominant serovars were 8, 4 and 1 (39.2%, 21.4% and 10.7% of the isolates, respectively). No significant difference was found between isolates from sterile and non-sterile sites (X^2 =1.12; p=0.29). From group II distinct serovars were seen, the mixed serovars were identified in 19 isolates from a single site (55.9%) (Table II) and in 15 (44.1%) distinct serovars were isolated from different sites or from the same site but at different times (Table III). As shown in Table II, the most common serovars in mixed infections from single sites were 8 and 4 (34.2% and 21.1%, respectively). Among the 12 patients with multiple isolates, 27 strains were typed (Table III). Also, serovars 8 and 4 were more frequent (10/27, 37% and 7/27, 25.9%, respectively). Considering all isolates, they were arranged to the species M. avium (88%), M. intracellulare (7.8%), and M. scrofulaceum (4.2%). Consequently M. avium was the main specie of the MAC infecting the patients. DISCUSSION The purpose of this study was to assess the distribution of M. avium serovars from patients with AIDS in Brazilian centers that show the highest rate of AIDS infection. Since MAC infection is the second most important mycobacteriosis associated with AIDS, this study was performed with MAC isolated from AIDS patients from Sao Paulo and Rio de Janeiro. The serovars were established accordingly to the GPL (mycoside C) content of the isolates. A majority of the isolates (88%) were assigned to the M. avium serovars. When the serovars were ranked according to the isolated strains the results were: serovar 8, 39.2%; serovar 4, 21.4%; serovar 1, 10.7%; mixed serovars 8 and 4, 37.8%. In this report, the predominant serovars in our study were similar to those in the USA, Canada and Australia (Horn et al. 1989, Yakrus & Good 1990, Dawson 1990, Tsang et al. 1992) and distinct from those in Germany, Sweden and the United Kingdom (Ruf et al. 1989, Hoffner et al. 1990, De Smet et al. 1996). Geographic differences may be related to a combination of factors such as: prevalence of determinate serovars in the environment, differences in bacterial virulence factors and host immunoresponse status, since AIDS patients are particularly susceptible to determinate serovars of MAC. Like others (Yakrus & Good 1990, Tsang et al. 1992) we did not find significant differences between the isolates from sterile and non-sterile sites. The frequency of mixed serovars in our patients was higher than reported by others. For instance, in a large-scale study Tsang et al. (1992) observed 6% mixed serovars while in this study we observed 37.8%. In another study, Dawson (1990) found multiple serovars among isolates from multiple sites in 38% of 45 patients examined, and Hoffner et al. (1990) found 24.9% of multiple serovars from distinct body sites of isolation. Whether these difference are attributed to the size of the populations sampled (6,264 cultures in the Tsang et al. 1992 study as compared to only 90 isolates in the present study) or to environmental factors requires further investigations. The occurrence of mixed infections raises important questions regarding the management of M. avium infections, particularly in the event that serovars from distinct sites have distinct drug resistance patterns (von Reyn et al. 1995). Mixed infections (polyclonal infections) have also been demonstrated using RFLP assays (Von Reyn et al. 1996). The frequency of mixed infections reported varied widely (Arbeit & Slutsky 1993, Slutsky & Arbeit 1994) leading to the suggestion that most studies indeed underestimate the rate of polyclonal infection in AIDS patients. The mixed serovar infection finding is not easy to evaluate. Our first thought was that this could be a consequence of immunecompromised patients exposed to multiple environmental sources of MAC, since this organism is ubiquitous in nature. This is corroborated by von Reyn et al. (1996), which suggests that mixed infection may represent a synergic infection between two different MAC. The importance of epidemiological and clinical implications of mixed (polyclonal) infections in AIDS patients indicate that further investigation is necessary. Consequently, we are proceeding to a study of Brazilian isolates by DNA fingerprint using the IS1245 insertion sequence in order to establish the genetic identity of the strains. ACKNOWLEDGEMENTS To Dr Angela W Barreto and Dr Fatima Martins from Centro de Referencia Prof. Helio Fraga, and Dr Fatima Fandinho and Cristina L Almeida from Fundacao Oswaldo Cruz, for supplying several of the clinical Mycobacterium avium complex isolates for analysis. To Dr Hugo David from Instituto de Higiene e Medicina, Universidade de Lisboa, Portugal for reviewing the manuscript. To Anne Varnerot from Institute Pasteur for technical advice. This work was supported by CNPq and FINEP (Brasil). REFERENCES
Copyright 1997 Fundacao Oswaldo Cruz The following images related to this document are available:Photo images[oc97083a.jpg] [oc97083c.jpg] [oc97083b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}