 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
RESEARCH NOTE Evaluation of popular stains for the diagnosis of American cutaneous leishmaniasis Carmen Manuela Castillo^+, Carlos Rojas Corporacion CIDEIM, Avda 1N No 3-03, Cali, Colombia
Received 17 September 1996
Code Number: OC97095
File Sizes:
Text: 8.9K
Graphics: Tables (jpg) - 19.8K
Line drawings and photographs (jpg) - 15.1K
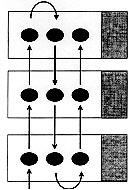
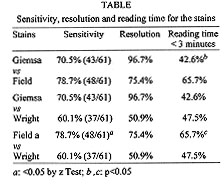
Key words: American cutaneous leishmaniasis - diagnosis - Giemsa - Wright - Field The diagnosis of American cutaneous leishmaniasis (ACL) is usually suspected on examination of compatible lesions on an individual living in, or having traveled to, a known endemic area of transmission. Definitive diagnosis of the disease is usually made in the clinical laboratory and needs visualization of amastigotes or the isolation of the parasite in culture. Indirect diagnostic methods such as serologic tests or the Montenegro intradermal test are available, but are rarely confirmatory of the disease (GI Palma & Y Gutierrez 1991 Clin Lab Med 11: 909-922). In Colombia, confirmation of the etiology is a requirement for treatment with meglumine antimoniate-glucantime. Diagnostic methods range from very simple and economic techniques like the dermal scraping to more complex and expensive ones, such as the polymerase chain reaction (PCR). However, most of the new and more complex methods are not available to the health services in developing countries because of their elevated costs, infrastructural requirements and lack of trained personnel in the endemic areas. Dermal scraping has been recommended by the Colombian Ministry of Health as the standard diagnostic technique for the endemic areas in Colombia (Guia Integral de Manejo de las Enfermedades Transmitidas por Vectores 1996, 75 pp.). Although dermal scraping has advantages over other available methods, this method still has some constraints that prevent its massive use by the health services in all the Colombian states in which cutaneous leishmaniasis is endemic. One of these constraints is the histology stain (Giemsa stain) that has been standardized and recommended for staining the material obtained from the dermal scraping. Health posts in endemic areas do not have Giemsa stain, mainly because it is expensive compared to other available stains, and because within the public health system of Colombia it is not used in other diagnostic procedures. For these reasons, health workers have been using Wright instead of Giemsa, with apparently good results (personal communication). However, to our knowledge there are no reports in which this or other alternative stains are compared with Giemsa in the diagnosis of cutaneous leishmaniasis. In this report, we present the results of a study comparing Giemsa with two low cost, Wright and Field stains, in 61 Colombian patients with parasitologically confirmed diagnosis of ACL. Patients were evaluated by the Centro Internacional de Entrenamiento e Investigaciones Medicas (CIDEIM) in Tumaco (n=45) and Cali (n=16), between July 1994 and June 1995. Parasitologic diagnosis was confirmed using diagnostic methods as described by KA Weigle et al. (1987 Am J Trop Med Hyg 36: 489). These methods are used by CIDEIM in the routine evaluation of patients with skin lesions compatible with leishmaniasis. Samples for dermal scraping were obtained from the margins of the most recent lesion. From the same outer border of the skin lesion an incision of 5 mm in length, 3 mm in depth was made, with a number 15 surgical blade, then dermal tissue scraped with a steril stainless steel spatula and smeared onto a glass slide (MA Escobar 1992 Tropical Doctor 22 Suppl. 1: 69-78). A total of three slides were obtained for each patient and three smears per glass slide. In order to guarantee that the three slides had a comparable amount and quality of dermal tissue, the tissue samples were distributed sequentially on the three slides as indicated in Figure. Figure: Distribution of tissue samples obtained from lesion borders. Arrows indicate sequence of samples placement on slides examined by each of three histological stains: Giemsa, Field and Wright.The stain for each slide was assigned at random. Slides were identified only with a three digit number obtained from a list of random numbers previously defined for the study. Slides were stained and examined for the presence of amastigotes by an experienced medical technologist. Stained smears were scanned under the 10X objective for amastigotes in areas where granulomas and mononuclear leukocytes were seen. The 100X oil immersion objective was used to confirm the identification of the parasite. This process was carried out until the identification of the first amastigote, or until 100 fields were scanned with the 100X oil immersion objective in each of the three samples per slide. The comparison was based upon a) sensitivity: defined as the proportion of stained slides that were positive for amastigotes; b) resolution: based on the definition of cytological characteristics of the amastigote: nucleus, kinetoplast and cell membrane; and c) time required to identify the first parasite: < 3 min, 3 to 10 min, and > 10 min. The z test was used for comparison of proportions obtained for the different stains (Table). Although Field was more sensitive than Giemsa (78.7% vs 70.5%), and Wright less sensitive (60.1% vs 70.5%), these differences were not statistically significant. The results obtained in these 61 patients suggest that both alternative stains are adequate for diagnosis using dermal scrapings. However, Field demonstrated significantly greater sensitivity than Wright, 78.7% vs 60.1%. Giemsa yielded a better resolution of all the cytological characteristics of the amastigote (96.7% vs 75.4% for Field and 50.9% for Wright), but this advantage did not affect the sensitivity or the time required to confirm the diagnosis with this particular stain. A larger proportion of slides (65.7%) were confirmed for parasites with Field stain in less than 3 min compared with the proportion obtained with Giemsa and Wright, 42.6% and 47.5%, respectively. This difference was probably due to the elimination of red blood cells by the Field staining procedure, which facilitates the identification of white blood cells and parasites. Giemsa and Wright are derivatives of the Romanowsky stain but Wright contain less Azur B, which results in a somewhat pale bluish-violet coloration of the nuclei and kinetoplast (ME Boon & JS Drijver 1986. Routine cytological staining techniques, p. 94-101, Macmillan Education LTD. London). Therefore the resolution of Giemsa stain, is generally superior than Wright (96.7% vs 50.9%). These results suggest that in circumstances where Giemsa stain is not available, such as in the cutaneous leishmaniasis endemic areas of Colombia, Field stain is a good alternative for direct dermal scraping. Field offers two other advantages: it requires one tenth of the time needed to stain a single slide with Giemsa (6 vs 60 min); and the cost of the stain required for one slide is 35 times less expensive than Giemsa (0.001 vs 0.035 US$). An important outcome of using the Field stain for the evaluation of dermal scraping is the facilitation of incorporating the diagnosis of dermal leishmaniasis into malaria surveillance and diagnosis programs, which in Colombia utilize Field stain. Although Giemsa will probably continue to be the gold standard for the diagnosis of dermal leishmaniasis in places where this reagent is available, the use of a single stain for two vector borne diseases in areas with limited diagnostic facilities would provide cost effectiveness to this diagnosis at the primary level of health care. Field stain provides a sustainable alternative where resources are limited. Acknowledgements: to Dr Nancy G Saravia for insighful review of the manuscript. This work was supported by the United States National Institutes of Health, Tropical Medicine Research Center, contract TMRC 5 p50 AI30603-50 and COLCIENCIAS contract 2229-04-001-92. Copyright 1997 Fundacao Oswaldo Cruz The following images related to this document are available:Photo images[oc97095b.jpg] [oc97095a.jpg] |
| |||||||||

{kind=link}
{kind=link}