 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Diagnosis of dengue by using Reverse Transcriptase- Polymerase Chain Reaction Marize Pereira Miagostovich/^+, Flavia Barreto dos Santos, Eliane Saraiva M de Araujo, Juarez Dias*, Hermann G Schatzmayr, Rita Maria Ribeiro Nogueira Laboratorio de Flavivirus, Departamento de Virologia, Instituto Oswaldo
Cruz, Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil ^+Corresponding author. Fax: + 55-21-270.6397. E-mail: marizepm@gene.dbbm.fiocruz.br Received 10 March 1997; Accepted 16 June 1997
Code Number:OC97111
Sizes of Files:
Text: 19.4K
Graphics: Tables (jpg) - 88.1K
Line drawings and photographs (jpg) - 6.5K
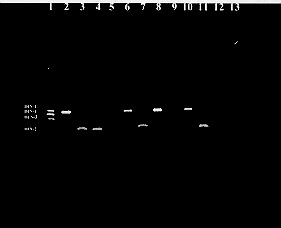
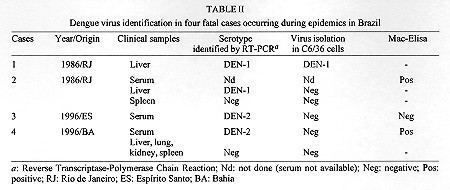
A rapid identification of dengue viruses from clinical samples by using a nested reverse transcriptase-polymerase chain reaction (RT-PCR) procedure was carried out for diagnostic and epidemiological purposes. RT-PCR identified DEN-1 and DEN-2 viruses in 41% (41/100) of previously confirmed cases and provided an accurate confirmation of DHF in four fatal cases. RT-PCR was also useful for detecting and typing dengue viruses in suspected cases, allowing a rapid identification of new serotypes in endemic areas. Key words: dengue - diagnosis - virological surveillance - polymerase chain reaction Dengue virus activity increased significantly in Brazil after the introduction of dengue virus type 1 (DEN-1) into the State of Rio de Janeiro in 1986 (Schatzmayr et al. 1986). DEN-1 was the only serotype circulating in the country until 1990, when dengue virus type 2 (DEN-2) was also introduced (Nogueira et al. 1990). During the last decade, dengue epidemics have been recorded annually in the country and the number of reported cases has shown dengue infection to be an increasing public health problem (Figueiredo 1996) The circulation of dengue viruses in the Americas, including dengue virus type 3 (DEN-3) which reappeared in the region (Nicaragua and Panama) in 1994 (CDC 1995) after an absence of 16 years, represents a real threat of new dengue epidemics in the country. Since a dengue vaccine is still being developed, an active surveillance system is the key to early detection and prevention of large epidemics. The availability of a rapid, sensitive and specific method to detect dengue virus infection is one of the most important factors necessary for that purpose. The laboratory diagnosis of dengue virus is based primarily on virus isolation and serology. However the increasing number of reported cases of dengue fever/dengue haemorrhagic fever (DF/DHF) in Brazil (Nogueira et al. 1993, Zagne et al. 1994, Souza et al. 1995, Vasconcelos et al. 1995) showed the need for new approaches to diagnosis. Various protocols of polymerase chain reaction (PCR) have offered obvious advantages for the detection of dengue virus (Deubel et al. 1990, Morita et al. 1991, Pao et al. 1992, Seah et al. 1995). The reverse transcriptase-polymerase chain reaction (RT-PCR) protocol developed by Lanciotti et al. (1992) could detect and identify all four serotypes of dengue viruses simultaneously in a nested procedure. In the present study we employed this protocol for diagnostic and epidemiological purposes. Virological investigation of clinical samples established RT-PCR as an useful tool in the laboratory diagnosis of dengue infections. MATERIALS AND METHODS Clinical samples Group 1: acute sera from 100 dengue cases previously confirmed by paired serology. All cases were negative for dengue virus isolation. Serum samples were obtained during the dengue epidemic which occurred in the State of Rio de Janeiro in 1995-1996. Group 2: sera and necropsy tissues from 31 fatal cases suspect of DHF. All clinical samples were obtained from the collection at the Laboratory of Flavivirus, Instituto Oswaldo Cruz, FIOCRUZ Group 3: acute sera collected by the epidemiological surveillance system in dengue endemic areas during outbreaks occurred in 1996 in the states of Bahia (BA), Rio de Janeiro (RJ) and Espirito Santo (ES). Virology and serology Virus isolation was attempted by inoculation into clone C6/36 Aedes albopictus cells (Igarashi 1978) and virus isolates were typed by the indirect fluorescent antibody test using serotype-specific monoclonal antibodies (Gubler et al. 1984). IgM capture enzyme-linked immunosorbent assay (MAC-ELISA) was performed using a mixture of DEN-1 and DEN-2 antigens according to Nogueira et al. (1992). RNA extraction and RT-PCR Viral RNA was extracted from clinical samples using a silica protocol described previously by Boom et al. (1990). RT-PCR for detecting and typing dengue viruses was carried out according to Lanciotti et al. (1992). Briefly, cDNA copies of a portion of the viral genome (capsid/prM) were produced and amplified using two consensus primers designed to anneal to any of the four dengue virus types. Second-round amplification with type-specific primers results in different bands of DNA, characteristic for each dengue virus type, that could be observed directly in 1% agarose gel stained with ethidium bromide. All primers were kindly provided to Dr Vance Vorndam (CDC, Puerto Rico). Positive and negative controls were included in all steps. RESULTS Group 1: fig. shows up the characterization of DEN-1 and DEN-2 viruses by the agarose gel analysis of the amplified products. RT-PCR identified dengue serotypes in 41% (41/100) of cases studied. Eleven DEN-1 and 30 DEN-2 strains were demonstrated in acute sera. Table I shows the RT-PCR results according to IgM antibody detection. Figure : Characterization of DEN-1 and DEN-2 viruses by Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR). Ethidium bromide stained agarose gel showing RT-PCR products: lane 1, molecular weight marker of DEN-1, DEN-4, DEN-3 and DEN-2 RT-PCR products corresponding to 482 bp, 392 bp, 290 bp, 119 bp, respectively (Lanciotti et al. 1992); lanes 2, 6 and 8, DEN-1 from serum samples; lanes 3, 4 and 7, DEN-2 from serum samples; lanes 5 and 9, negative sera; lane 10 and 11, positive controls of DEN-1 and DEN-2 isolated from Aedes albopictus C6/36 cell line; lane 12, uninfected cell culture; lane 13, water. Group 2: DHF was confirmed by dengue RNA identification in four cases, two from liver specimens and two from sera (Table II). The remaining cases (27) were negative for virus isolation and RT-PCR on available samples, although eight of them had anti-dengue IgM antibodies. Group 3: RT-PCR identified the aetiological agent responsible for three dengue epidemics studied in the states of BA, ES and RJ (Table III). In Bahia this method detected the introduction of DEN-1 into the area. In all opportunities the clinical diagnosis was also confirmed by virus isolation and serology. DISCUSSION The anti-dengue IgM response and virus isolation using the Ae. albopictus C6/36 cell line have been routinely used for dengue diagnosis in Brazil (Schatzmayr et al. 1986, Figueiredo et al. 1992, Miagostovich et al. 1993, Nogueira et al. 1993, Vasconcelos et al. 1993). However, due to its speed and sensitivity, PCR has been adopted as an alternative method in dengue diagnosis (Laille et al. 1991, Chungue et al. 1993, Morita et al. 1994). The whole RT-PCR procedure, including RNA extraction, is expensive and requires adequate care in handling the specimens safely, avoiding contamination at all stages. Thus, it should be used mostly on clinical samples from severe forms of infection and in sera obtained from areas recently affected by dengue viruses. In relation to RNA extraction, we used the silica protocol described by Boom et al. (1990) instead of the method described originally in the RT-PCR procedure (Lanciotti et al. 1992). The elimination of phenol/chloroform extraction and ethanol precipitation has obvious advantages. Enzyme-linked immunosorbent assay (Elisa) has proven to be a sensitive method for detecting anti-dengue IgM (Nogueira et al. 1992), however a monotypic response is rarely observed because of the extensive cross-reactivity among dengue viruses. In our study, RT-PCR identified dengue virus RNA in 32.4% and 59.4% of cases respectively in relation to the presence or absence of anti-dengue IgM antibodies. Different studies have shown a range from 12% to 100% of virus detection in serologically confirmed cases (Chungue et al. 1993, Chan et al. 1994). The inverse correlation between virus isolation and anti-dengue antibodies has been well documented (Nogueira et al. 1992). In agreement with Chan et al. (1994), our results also showed that RT-PCR was most useful when anti-dengue antibodies were undetectable. RT-PCR provided an accurate identification of dengue virus in four fatal cases. Cases 1 and 2 occurred during a DEN-1 epidemic in Rio de Janeiro in 1986. Case 1 was a 17 year-old male who died seven days after the onset of disease. Liver was the only specimen available 12 hr after death. At that time we isolated DEN-1 virus from the specimen. Dengue virus isolation 40 hr after death was described by Rosen et al. (1989). Case 2 was a 51 year-old man presenting with the following signs and symptoms: fever, myalgia, diarrhea, hemoptysis, hematemesis, disorientation and progression to shock seven days after the onset of disease. At that time demonstration of anti-dengue IgM antibody was a good marker to confirm the clinical and epidemiological diagnosis. RT-PCR was successful in detecting DEN-1 virus in the liver from this patient. Dengue antigen was also demonstrated in liver and lung by using the immunoperoxidase technique (data not shown). The detection of dengue virus in two liver specimens frozen for ten years suggests that RT-PCR is applicable to retrospective studies. Attempts at RT-PCR on formalin-fixed and paraffin-embedded tissues gave unsuccessful results that could be explained by crosslinkage of viral nucleic acid to host proteins caused by formalin fixation (Pearse 1980). Case 3 was a 52 year-old female presenting fever, cephalgia, arthralgia, rash, petechiae, hematocrit < 45% and a platelet count of 21,000 mm^3 progressing to shock six days after onset of disease. This death occurred during an extensive dengue epidemic in Espirito Santo, where we isolated 25 strains of DEN-2 (data not shown). RT-PCR detected DEN-2 RNA in serum and was conclusive when other methods were unsuccessful. Case 4 was a 29 year-old male who died when arriving at the hospital. The death occurred in Bahia (Feira de Santana) during an extensive epidemic where 64,435 cases were reported in that state (Secretary of Health, Bahia). DEN-1 (14) and DEN-2 (8) strains were isolated during 1996. Unfortunately clinical data were not available to the laboratory. Severe forms of dengue infection after DEN-2 virus introduction into Espirito Santo and Bahia was also observed in the states of Rio de Janeiro and Ceara (Nogueira et al. 1993, Zagne et al. 1994, Vasconcelos et al. 1995) showing the hemorrhagic potential of the Jamaican topotype. RT-PCR was especially useful for monitoring dengue virus activity in endemic areas in Brazil, allowing a rapid identification of dengue viruses in Rio de Janeiro and Espirito Santo. In Bahia we detected the introduction of DEN-1 virus during a DEN-2 epidemic when the local epidemiological surveillance service observed that many individuals were experiencing a second dengue virus infection. Circulation of those serotypes was later confirmed by virus isolation in Ae. albopictus C6/36 cells. The whole procedure for isolating and typing dengue viruses in culture cells is time consuming but it is still the definitive system for characterizing dengue viruses. Taken together our results emphasize the importance of different approaches in dengue diagnosis. RT-PCR data obtained here, confirm this methodology as an important tool for clinical diagnosis and virological surveillance. Efforts are being made to establish this RT-PCR protocol in the National Network of Dengue Laboratories, as an attempt to improve the Dengue Epidemiological Surveillance System, contributing consequently to the current Program of Aedes aegypti Eradication, established by the Brazilian Government. ACKNOWLEDGMENTS To Alice Paiva and Maria Helena Venturini for serum samples from Espirito Santo. To Jose de Carvalho Filho, Jose da Costa Farias Filho, Patricia Aila da Costa and Jose Mariano da Silva for technical assistance. Supported by CNPq, Fundacao Banco do Brasil and COLAB, Ministry of Health. REFERENCES
Copyright 1997 Fundacao Oswaldo Cruz The following images related to this document are available:Photo images[oc97111d.jpg] [oc97111c.jpg] [oc97111b.jpg] [oc97111a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}