 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
RESEARCH NOTE Urban Visceral Leishmaniasis in Venezuela CM Aguilar/^+, E Fernandez, R Fernandez, DC Cannova, E Ferrer*, Z Cabrera*, WJS Souza**, SG Coutinho**
Laboratorio de Entomologia/Leishmaniasis, Departamento de Parasitologia,
Facultad de Ciencias de la Salud (FCS), Universidad de Carabobo, Valencia,
Apdo. Postal 5100, Naguanagua, Estado Carabobo, Venezuela Received 7 February 1997: Accepted August 1997
Code Number:OC98003
Sizes of Files:
Text: 8K
Graphics: Line drawings and photographs (jpg) - 21.7K
RESEARCH NOTE
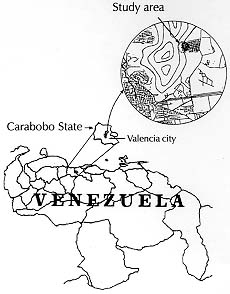
Key words: leishmaniasis epidemiology - urban visceral leishmaniasis - new focus - Venezuela American visceral leishmaniasis is a protozoosis caused by Leishmania (L.) chagasi, Cunha and Chagas 1937 (R Lainson & JJ Shaw 1987, p.1-104. In W Peters, R Killick Kendrick (eds) The Leishmaniasis in Biology and Medicine, Biology and Epidemiology, Vol I, Academic Press, London). The infection is trasmitted to the mammalian host by the bite of female phlebotomin sandflies Lutzomyia longipalpis (G Grimaldi et al. 1989 Am J Trop Med Hyg 4: 687-725, OMS 1990 SIT No 793, Geneva). The disease is mainly prevalent in Brazil, Venezuela, Argentina (Chaco), with discrete endemic foci in Paraguay, Bolivia, Peru, Colombia, El Salvador, Honduras, Guatemala and Mexico (L Rey 1992, Parasitologia, 2nd ed., Rio de Janeiro, 222 pp.). Although rural areas are the most affected, infection has been reported from urban and suburban regions of Brazil, such as the cities of Sobral and Russas (State of Ceara), Teresina (State of Piaui), Jacobina (State of Bahia), Rio de Janeiro (State of Rio de Janeiro) and Natal (State of Rio Grande do Norte), representing to the country the appearence and spreading of the disease in suburban areas of big cities one of the emerging public health problems of the last few years (L Deane & G Grimaldi 1985, p. 247-281. In KP Chang & RS Bray (eds) Leishmaniasis Vol I, Elsevier Amsterdam, S Jeronimo et al. 1994 Trans R Soc Trop Med Hyg 88: 385-388, RB Tesh 1995 Am J Trop Med Hyg 52: 287-292). Since the report of the first human case in Venezuela (NA Martinez Niochet & RS Pons 1941 Gac Med Caracas 48: 329-332), several more foci of the disease have been reported, the most important endemic areas being in the central-western, eastern and southern rural regions of the country (F Pifano 1954 Arch Venez Pat Trop Parasit Med 2: 213-219, JW Torrealba 1970 Observaciones sobre diagnostico terapeutica y evolucion de la leishmaniasis visceral humana y canina. Thesis, Universidad de Carabobo, Valencia, Venezuela 367 pp., L Garcia-Rivas 1993 Dermatol Venez 31: 39-46). Up to 200 cases had been reported by 1985, in foci where human cases were sporadic and the endemicity was low (JV Scorza et al. 1985, p. 289. In KP Chang & RS Bray loc. cit.). So far, no suburban leishmaniasis visceral focus have been refered in Venezuela. In the central focus where Carabobo is located, cases of visceral leishmaniasis have been reported from rural areas and cases in hospitals originated in these areas (ADF Amaral et al. 1961 Rev Inst Med Trop São Paulo 3: 91-98, O Guinand & LA Rodriguez 1967 Acta Med Venez 17: 244-249). In 1989 we detected a 2.5 years old child with kalazar, born and resident of a locality called Los Magallanes (CM Aguilar et al. 1992 Acta Cientif Venez 43: 191), where transmission of the disease had not been reported before. In order to determine the autoctonous suburban character of the disease in the metropolitan area of Valencia (State of Carabobo, central focus) we initiated a clinical, parasitological and seroepidemiological surveillance study in a suburban shanty town ( Fig.) between 1989 and 1996. To date, we have clinically and parasitologically diagnosed three aditional cases, and established a seroprevalence of 17.8% (128 seropositives of 718 individuals tested) using the ELISA test, from a population of 842 inhabitants. So far, most of the seropositive persons have remained asymptomatic or oligosymptomatic, as described by R Badaro et al. (1986 J Inf Dis 154: 639-649). For the evaluation of the zoonotic character of the disease already confirmed by JW Torrealba et al. (1961 Rev Venez Sanid Asist Social 26: 342-349) in the central focus of Venezuela, we carried out a census of 81 dogs (Canis familiaris), house by house, and blood sampling for serology by indirect fluorescent antibody test, according to S Coutinho et al. (1985 Mem Inst Oswaldo Cruz 80: 17-22), resulting in 27.3% positives (21/77). We searched for parasites in 13 dogs with positive serology, after auptopsy, finding amastigotes in Giemsa stained samples of ear pinna, bone marrow and/or liver in eigth dogs. An indoor and outdoor capture strategy using a Shannon trap, during one year of capture (August 1992 - July 1993) was captured a total of 1757 species: 1280 (72.9%) Lu. evansi, 23 (1.3%) Lu. longipalpis and 454 (25.8%) the other species. So much Lu. longipalpis and Lu. evansi are considered species vectors in Venezuela (ADF Amaral et al. 1961 Gac Med Caracas 70: 389-408, MD Feliciangeli et al. 1993 Acta Cientif Venez 44: 262). Dissection of the digestive tract of collected sandflies resulted in the detection of abundant promastigotes in the midgut in one Lu. evansi specimen. Parasites were isolated from bone marrow of two patients by inoculation of hamsters (Mesocricetus auratus) and subculturing spleen and liver tissue from these infected animals in NNN medium. Species identification of parasites isolated from humans, dogs and Lu. evansi by immunological and molecular biology techniques, are already in progress.
The data obtained indicate the presence of a real autoctonous suburban hypoendemic focus of american visceral leishmaniasis in the studied area. The local inhabitants have been resident of the locality for the last 20 years. The group at highest risk lived in the lowland area with climate features of tropical dry forest, where the sandflies live and frequently invade the human dwellings. In this way, a new ecological niche has been activated for visceral leishmaniasis in the metropolitan area of the city of Valencia, as it has been pointed out in Brazil by S Cunha et al. (1995 Trans R Soc Trop Med Hyg 89: 155-158). The present data should encourage health authorities to carry out control measures to avoid further spread of the disease. Acknowledgements To Licenciada Mercedes Pacheco de Montesinos (Universidad de Carabobo) for help in colleting human blood samples, Dr Irma Lara (Ministery of Health, Venezuela) for support in carrying out the field work and Dr Nino Incani (Universidad de Carabobo, Venezuela) for suggestions in preparing the manuscript. Financed in part by grants of CODECIH, Universidad de Carabobo and CONICIT (S1-2462), Venezuela. Copyright 1998 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc98003a.jpg] |
| |||||||||

{kind=link}