 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Response to Heterologous Leishmanins in Cutaneous Leishmaniasis in Nigeria - Discovery of a New Focus Simon M Agwale/^+, Dockha D Duhlinska, Gabriel Grimaldi Jr*
Department of Zoology, University of Jos, P.M.B. 2084, Jos, Plateau State,
Nigeria
^*Departamento de Imunologia, Instituto Oswaldo Cruz, Av. Brasil 4365,
21045-900 Rio de Janeiro, RJ, Brasil
Received 13 January 1997; Accepted 17 September 1997
Code Number:OC98005
Sizes of Files:
Text: 26.2K
Graphics: Line drawings and photographs (jpg) - 13.7K
Tables (jpg) - 28.8K
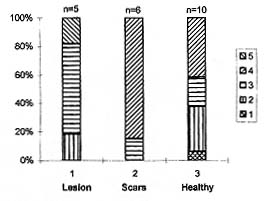
A pilot study was undertaken to preliminary illustrate the leishmanin skin test (LST) positivity to distinct antigen preparations (derived from promastigote of either Leishmania major or L. amazonensis, or pooled L. mexicana, L. amazonensis and L. guyanensis) in cutaneous leishmaniasis (CL) patients and healthy subjects living in two endemic foci in Nigeria. The study was designed to provide insights into whether cross-species leishmanin, such as that prepared from New World Leishmania could be useful to detect cases of Old World leishmanial infection and to compare the results with LST using L. major-derived leishmanin. The overall LST positivity in individuals from Keana tested with the cross-species leishmanin was 28.7% (27/94), while the positivity rate in the subjects from Kanana tested with the same leishmanin was 54.5% (6/11). Lower positivity values were obtained when L. major (12.5%; 11/88) or L. amazonensis (15.8%; 9/57) was tested as antigen in grossly comparable populations. Moreover, the pooled leishmanin identified most of the subjects (13/14; 92.9%) with active or healed CL, and the maximum reaction sizes were found among positive subjects in this group. No healthy controls (10 total) showed specific DTH response. The LST was useful for assessing the prevalence of subclinical infection and for measuring CL transmission over time. We report for the first time the occurrence of CL in Kanana village of Langtang South local government area of Plateau State. Key words: leishmaniasis - cutaneous leishmaniasis - Leishmania major - immunoprevalence - Nigeria Cutaneous leishmaniasis (CL) has been observed in the population of northern Nigeria by a number of workers (McCulloch 1930, Elmes & Hall 1944, Jelliffe 1955, McMillan 1957). Despite the presence of CL in the country, only scanty information is available on the epidemiology of the disease. Until the discovery of Keana village in central Nigeria as an endemic focus of CL (Agwale et al. 1993), leishmaniasis was thought to extend from northern Nigeria to the north, between 10 degrees N and 17 degrees N and probably much further (Jelliffe 1955, Obasi 1991). The LST, which measures the cutaneous delayed-type hypersensitivity (DTH) reaction to Leishmania-derived antigens, is an important tool in the epidemiological study of leishmaniasis. In CL the LST will become positive 2-3 months after the appearance of the lesion and may remain positive for life (Furtado 1980, Manson-Bahr 1987). Moreover, specific LST reactivity has often been associated with acquisition of immunity to reinfection and skin test cross reactivity is usually paralled by comparable cross immunity (reviewed in Bryceson 1976, Grimaldi & Tesh 1993). T cell responses correlate with recovery from and resistance to human leishmaniasis, thus a positive LST associated with protection might be a valuable tool for evaluating vaccine trials. Periodic boosting in humans using inactivated parasites promotes a DTH response to leishmanial antigen, which seems to increase the recipient's chance of being protected (Mayrink et al. 1979, Castes et al. 1994). At present, however, there is no standardized antigen preparation available for the determination of DTH response in leishmaniasis patients, and whole killed promastigotes have been widely used for evaluation of various immunization trials (reviewed in Grimaldi 1995). The present study was designed to illustrate the efficacy of distinct leishmanin antigens in skin testing patients and healthy subjects living in endemic foci (which primarily involved school girls residing in Keana village), in order to obtain information on some epidemiological features of CL in Nigeria. This paper also reports, for the first time, the occurrence of CL in Kanana village of Langtang south local government area of Plateau State. MATERIALS AND METHODS Study sites - The study was carried out in north-central Plateau. The Jos Plateau, situated in the southeast area of the north-central Plateau, is approximately 170 by 90 km in extent; except for the Shere hills (1,800 m), the average elevation is about 1,400 m. It is dominated by granites and volcanic rocks. Keana village, the major area studied, is situated about 262 km southwest of Jos (8 degrees 40'N and 9 degrees 44'E), the capital of Plateau State. Its vegetation is generally Guinea Savannah, which consists of tall grasses and some trees. The annual rainfall of the zone is about 150 cm and lasts between 6 and 8 months. The population in Keana is about 10,000 people. Kanana village, a new focus of CL, is situated about 220 km southwest of Jos (8 degrees 37'N and 9 degrees 44'E). Its vegetation is also generally Guinea savannah. It is a separate focus from Keana and the two villages are about 350 km apart. The population in Kanana is about 1,000 people. Study population - The three instances in which different leishmanin antigens were used to test schoolgirls were performed in different individuals from the same school community. Study 1 (1995) in Keana (using the pooled leishmanin), consisted of 83 schoolgirls (5 with active cutaneous lesions, 7 with scars and 71 healthy), 6 teachers (2 with active lesions, 1 with scars, 3 healthy) and 5 health workers (n=94). In addition, two persons (the principal investigator and his colleague) were tested as "negative controls". Furthermore, 11 individuals (2 with active lesions and 9 healthy) from Kanana village were tested to prove the existence of leishmanial infection in this locality. Study 2 (1996) in Keana (using L. major-derived leishmanin), consisted of 4 schoolgirls with active lesions, 5 with scars and 79 healthy residents in the school community (n=88). "Negative controls" were 4 students from Jos who have never lived in the endemic leishmaniasis foci of Nigeria. Study 3 (1996) in Keana (using L. amazonensis-derived leishmanin), consisted of 2 schoolgirls with active lesions, 6 with scars and 49 healthy residents (n=57). Again 4 students from Jos were selected as "negative controls". Clinical and laboratory diagnoses - Suspected leishmaniasis cases were seen by the collaborating health centre in Keana. Also during an active search of the prevalence of CL in Nigeria, active lesions were seen in a 25 year old girl who was born and lives in the village of Kanana, Langtang South local government area of Plateau State. After obtaining the consent of the village head, a cross sectional survey was carried out in an attempt to discover more cases of leishmanial infection in the local population. Data regarding age, sex, duration of living in the locality, and of infection (for individuals with lesions or scars) were collected. Diagnosis was based on microscopic detection of amastigotes in lesion biopsy smears, and/or isolation of the parasite in culture media, a positive LST, and clinical appearance of the lesions. In order to identify the causative agent(s) of CL in these villages, an attempt was made to isolate Leishmania from 6 human cases (5 and 1 patients with lesions in Keana and Kanana villages, respectively). The primary isolation was made by in vitro culturing of samples from the cutaneous lesions of BALC/c mice, previously inoculated with triturated fragments of lesions from patients with CL. The material from the animals was obtained by aspiration and inoculated, aseptically, directly into tubes of NNN blood-agar medium overlaid with either Schneider's Drosophila medium (Gibco) (Hendricks et al. 1978) supplemented with 20% heat-inactivated foetal bovine serum (FBS) or RPMI 1640 (Gibco) supplemented with either 4% FBS or 20% FCS as overlay. Leishmanin skin test - The leishmanin antigens used for skin testing of the local population were prepared at (1) the Oswaldo Cruz Foundation/Fiocruz, Rio de Janeiro, Brazil (consisting of pooled heat-killed L. mexicana, L. amazonensis and L. guyanensis promastigotes suspended in PBS with 0.5 % phenol), (2) the Federal University of Minas Gerais/UFMG, Belo Horizonte, Brazil (heat-killed L. amazonensis promastigotes), and (3) the Institute Pasteur, Tehran, Iran (L. major-derived antigens). Patients and controls in study 1 were tested with leishmanin (Lot number 05111194) from Fiocruz (which was a generous gift from Dr AG Ferreira, Biomanguinhos). The leishmanin derived from L. major (Lot number 110) and from L. amazonensis, which were employed in studies 2 and 3, were gifts from Dr F Modabber (Tropical Diseases Research, World Health Organization, Geneva, Switzerland) and Dr W Mayrink (Institute of Biological Sciences/UFMG), respectively. All skin test antigens were administered in a dose of 0.1 ml intracutaneously on the deltoid area of the left arm. The tests (reactions measured as skin indurations) were read after 48 or 72 hr using the ball-point pen method (Sokal 1975). An average induration diametre of equal or more than 5 mm was considered as a positive leishmanin test. RESULTS Skin test response to the pooled leishmanin (study 1) - The positivity rate in the 83 schoolgirls tested with this leishmanin was 25.3% (21/83; 5/5 with active lesions, 6/7 with scars and 10/71 "healthy volunteers"). Most of the schoolgirl subjects (11/12; 91.6%) with active or healed cutaneous lesions tested were positive, although there was considerable variation in size. The two healthy controls showed a negative response to the pooled leishmanin, but specific DTH reactivity was detected in 14.1% (10/71) of schoolgirls without history of CL. Several clinical types of the disease were recognized in the local population. The lesions were ulcerative, nodulo-ulcerative, and nodular, which are consistent with the clinical features of CL due to L. major (Griffiths 1987). In addition, BALB/c mice developed nodular lesions after one month of inoculation with one of the six clinical specimens so studied. Fig. shows the distribution of extent of reaction to leishmanin among the positive schoolgirls in Keana village observed in study 1. The results of skin tests analyzed according to duration of living in the focus is also reported (Table). Since the testing concentrated on schoolgirls, the results of other groups of individuals were not included in the illustrations, which refer only to study 1. Of the skin-tested school teachers (2 with active lesions, 1 with scars, 3 "healthy"), 50% (3/6) responded positively to the same leishmanin, with mean diameter of 14.5 mm, 24 mm, and 25 mm respectively. Moreover, 40% (2/5) "health workers" from the Primary Health Care Centre who participated in the study had mean diameters of 17.5 mm and 32 mm.
In Kanana village (new focus of CL), 11 subjects (2 with CL and 9 healthy) were selected for skin testing with the pooled leishmanin, of whom 6 (54.5%) were positive (with an induration diameter of 13-43 mm). Attempts at isolation of Leishmania (by in vitro culturing tissue homogenates in biphasic media) made in 6 cases (5 from Keana and 1 from Kanana) was succesful in only one patient with an active cutaneous lesion from Kanana (who showed the maximum reaction size among the positive subjects) but the parasites were not identified. Skin test response to L. major-derived leishmanin (study 2) - The positivity rate in the schoolgirls tested with the L. major-derived antigens in Keana (1996) was 12.5% (11/88; 2/4 with active lesions, 1/5 with scars and 8/79 healthy), with an induration diameter of 8-53 mm. The 4 healthy controls showed no specific DTH response. Skin test response to L. amazonensis-derived leishmanin (study 3) - The positivity rate in schoolgirls tested with this leishmanin was 15.8% (9/57; 1/2 with active lesions, 3/6 with scars and 5/49 healthy), with an induration diameter of 6-50 mm. The four healthy controls showed no specific DTH response. DISCUSSION The indirect methods currently in use for diagnosing leishmanial infection are based on several serologic techniques, including ELISA, direct agglutination test, immunofluorescence, and immunoblot, which detect anti-Leishmania antibodies (reviewed in Grimaldi & Tesh 1993). The LST (Montenegro test) is still frequently used for clinical diagnosis of the disease and in epidemiological surveys on the prevalence of leishmanial infection. At present, however, there is no standardized antigen preparation available for the determination of DTH responses in leishmaniasis patients, and whole killed promastigotes are still used. The high sensitivity obtained using whole promastigotes in the measurement of DTH response to leishmanial antigens continues to make the LST a widely used technique for assessment of leishmanial infection (Bryceson 1976, Furtado 1980, Manson-Bahr 1987). As immunologic techniques are refined and as highly specific antigens become available, they may prove useful in the development of improved skin tests (Badaró et al. 1990, Weigle et al. 1991) and serological assays (Jaffe & Zalis 1988, Andrade et al. 1992, Burns et al. 1993, Shreffler et al. 1993) for clinical diagnosis and epidemiological surveys. Vaccination may prove to be the easiest and most effective intervention method for the prevention of leishmaniasis at a population level, but prophylatic immunization using killed promastig-ote vaccines is currently only in experimental stages (Modabber 1990, Grimaldi 1995). A DTH response manifested as a positive LST, which correlates with protection (Mayrink et al. 1979, Castes et al. 1994), might be a valuable tool for evaluating vaccine trials. Therefore, standardized antigens are desirable and testing the quality of commercially available leishmanin preparations in different areas of the World is important, because of the widespread use of the skin test. In this study we have compared three different preparations of leishmanin in two endemic foci of leishmaniasis in Nigeria. The results showed that New World Leishmania-derived leishmanin was effective for detecting Old World CL in humans. This is in agreement with the findings of Akuffo et al. (1995) where leishmanin prepared from L. major was capable to detect CL caused by L. aethiopica or L. braziliensis. In addition, in terms of sensitivity, the pooled heat-killed L. mexicana, L. amazonensis, and L. guyanensis promastigotes was apparently superior to both the other products (L.major or L. amazonensis-derived leishmanin). The Fiocruz mixed leishmanin is produced in adequate quantities on a regular basis, and is available on request to other workers. An explanation for these differences could be antigen related or due to the fact that the heterologous leishmanins were tested in roughly comparable populations of, but different schoolgirls from the same school community in Keana. Comparison of these and previous studies in which skin testing was used is difficult because of the lack of uniformity in type inoculation site and dose of antigen used (Zijlstra & El-Hassan 1993). The LST allows one to estimate the extent of contact with the parasite and to detect cryptic infections (Pampiglione et al. 1975, Kadaro et al. 1993, Marty et al. 1994). The schoolgirls in Keana village who reacted positively to the pooled leishmanin (14.1%; 10/71), without evidence of past or active CL probably indicate a subclinical infection. Most reactions were probably induced by subclinical leishmanial infection (Badaró et al. 1986). Two normal controls from nonendemic areas and not known to have been exposed to leishmaniasis were skin tested with the same leishmanin preparation and did not respond. The individuals with history of CL who were leishmanin negative (studies 1-3) may not as yet have been sensitized or, otherwise, these could be due to false-negative test results (Kadaro et al. 1993). The distribution of positive subjects according to duration of living in the focus indicated the occurrence of continuing transmission at a relatively high rate. Asymptomatic human leishmaniasis cases (Schaefer et al. 1995), in particular reactivation of Leishmania infections in individuals infected with the human immunodeficiency virus (Alvar et al. 1992) could play a role in transmission. Xenodiagnosis of subclinical cases and cured VL patients has been suggested in order to establish their role in the transmission of infection (Schaefer et al. 1995). This procedure is also recommended for CL since visceralization of dermotropic Leishmania spp. may occur (Gradoni et al. 1990). In conclusion, as reported in another study (Akuffo et al. 1995), our data indicate that there is enough cross-reactivity between Leishmania species to warrant successful use of available leishmanin antigens for studying the epidemiology of leishmaniasis in endemic foci. Our study also confirmed that LST is a useful tool for assessing the prevalence of subclinical infection and for measuring CL transmission rate over time. ACKNOWLEDGEMENTS To the Village Heads for their co-operation throughout the study. To Mr J Sule, Mr B Dondji and Mr G Nga for help during field work. Financial support from the UNDP/WORLD BANK/WHO special program for Research and Training in Tropical Diseases (TDR). This study fulfils part requirement for the award of a Ph.D degree to SM Agwale by the University of Jos, Nigeria. REFERENCES Copyright 1998 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc98005b.jpg] [oc98005a.jpg] |
| |||||||||

{kind=link}
{kind=link}