 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
RESEARCH NOTE Diagnosis of Mucocutaneous Herpetic Infections by PCR without DNA Extraction
Mauricio L Nogueira, Alex F Carvalho, Edel F Barbosa, Claudio A Bonjardim,
Paulo CP Ferreira,
Laboratorio de Virus, Departamento de Microbiologia, ICB/UFMG, Av. Antonio
Carlos 6627, 31270-901 Belo Horizonte, MG, Brasil Received 8 September 1997; Accepted 8 January 1998
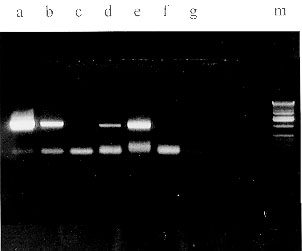
Code Number:OC98040 Key words: herpesvirus - diagnosis - PCR RESEARCH NOTE The mucocutaneous herpetic infections are common in a variety of clinical conditions and can be presented as vesicles, ulcers, crusts and pustules. When clinical diagnosis is not evident, as in immunossupressed hosts, viral cultures and Tzank smears could be used for diagnosis (GT Nahass et al. 1992 JAMA 268: 2541-2544). In AIDS patients the emergence of acyclovir resistant strains are not uncommon and the development of atypical herpetic lesions could drive to incorrect diagnosis and therapeutic (PA Chatis et al. 1989 N Engl J Med 320: 297-300). The PCR has been used as a rapid and specific method for the diagnosis of some viral infections including herpesvirus. Several authors show that PCR could be used for diagnosis of herpetic infections in a variety of conditions and that it is so efficient or superior to viral cultures and to the Tzank smears to establish and confirm the diagnosis of herpetic infections. They used samples from swabs, vesicles, crusts, archival tissues and virological cultures (S Kido et al. 1991 J Clin Microbiol 29: 76-79, CA Thomas et al. 1994 Am J Dermatopathol 16: 268-274, Nahass et al. 1992 loc. cit., 1995 J Am Acad Dermatol 32: 730-733). All of these authors used a DNA extraction step with organic reagents in their protocol. In attempt to improve a rapid diagnosis method based on PCR assay for mucocutaneous herpetic infection we proposed a PCR assay without DNA extraction from clinical samples of herpetic infections. In nine patients with mucocutaneous herpetic lesion, these were washed out with sterile saline, and a sterile swab cotton was rubbed onto the base of the ulcers and immersed in Eagle's minimal essential medium plus penicillin, amikacin, amphotericin B and 1% fetal bovine serum. A tenfold dilution of the clinical specimen was submitted to 100 C for 10 min and 8 ul were used as DNA template. The conditions of the reaction were as follow: 2mM MgCl2, dNTPs (dATP, dCTP, dTTP, dGTP, 1mM each), glycerol (1%), Taq polymerase (PROMEGA^R), buffers, primers (10 pM each, HSV1TK3 5'TCAGTTAGCCTCCCCCATC and HSV1TK5 5'ATGGCTTCGTACCCCTGCC or VZVTK3 5'AGGAAGTGTTGTCCTGAACGGC and VZVTK5 5'ATGTCAACGGATAAAACC GATGT), DNA template and water to a final volume of 20 ml. PCR amplification was carried out as follows: 35 cycles of 1 min at 94 C, 55 C and 72 C, and one cycle of 15 min at 72 C for HSV. For VZV the annealing temperature was 57 C. A DNA fragment of 1130 bp or 1025 bp were amplified corresponding to the TK gene of HSV-1 or VZV, respectively. The amplified product was visualized on 1% agarose gel stained with ethidium bromide. To confirm the specificity of the reaction a southern blot was performed and the hybridization and wash conditions were carried out according to GM Church and W Gilbert (1984 Proc Natl Acad Sci USA 81: 1991-1995). A DNA fragment containing the HSV or VZV TK gene (HSVTK or VZVTK) was labeled by "Nick Translation System"(PromegaA) as described by the manufacturers. We studied nine patients. In four samples the VZVTK was amplified. These patients presented facial and ocular zoster (two cases), one child with chickenpox and a immunossupressed adult with zoster. No amplifications with HSV primers were visualized in these cases. In three of these cases the southern blot confirmed the specificity of the reactions. In one case the southern blot was not performed. In five patients with HSV infections the PCR assay were positive. Samples from two patients with blister, one child with recurrent herpetic keratitis, one child with herpetic keratitis and blepharitis and a young female with stomatitis were PCR positive for HSV-1. No VZV amplification was detected when VZVTK primers were used. The southern blot assay was performed in two cases and was positive in both. All controll reactions were performed. Our findings without DNA extraction are in agreement with other reports of PCR amplification of HSV-1 and VZV from clinical samples like Kido (1991 loc. cit.), Thomas et al. (1994 loc. cit.) and Nahass et al. (1995 loc. cit.) Our results also show that PCR assay without DNA extraction has clinical application. The phenol-chloroform extraction is a standard method to extract viral DNA for PCR assay. Our approach show an advantage in time to perform the PCR assay, can prevent DNA from contamination of specimens by management and has not organic reagents that could inhibit the PCR assay. We conclude that PCR assay without DNA extraction is a good methodological tool for the diagnosis of mucocutaneous herpetic infections. The use of a multiplex HSV/VZV PCR or a HSV/VZV general primer as described by JM Baron et al. (1996 J Med Virol 49: 279-282) can improve our approach. The TK gene are the most common locus of mutations in acyclovir-resistant strains of VZV and HSV (G Boivin et al. 1994 J Infect Dis 170: 68-757, HJ Field & SE Goldthorpe 1992 Res Virol 143: 120-124). The amplification of this gene could give a methodological approach to determine the acyclovir-resistant strains.
Supported in part by CNPq, CAPES and FAPEMIG. The authors (MLN, PCPF, CAB and EGK) are recipients of CNPq fellowships.
Copyright 1998 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc98040a.jpg] |
| |||||||||

{kind=link}