 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Vol. 93(6): 827-829 RESEARCH NOTE Laryngeal Papillomatosis in an AIDS Patient Ledy HS Oliveira/+, Silvia MB Cavalcanti, Denise D Andrade/*, Eliene C Fonseca/** Departamento de Microbiologia e Parasitologia, Instituto Biomédico,
Universidade Federal Fluminenese, Rua Prof. Ernani Melo 101, 24210-130 Niterói,
RJ, Brasil Received 1 April 1998; Accepted 24 August 1998
Code Number:OC98219
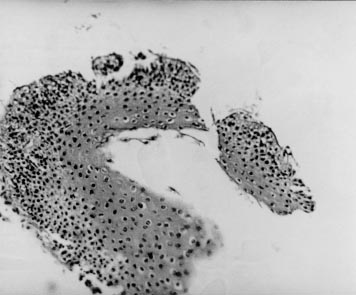
Key words: human papillomavirus - respiratory tract - AIDS - in situ hybridization RESEARCH NOTE Human papillomavirus (HPV) are small DNA viruses that present diverse oncogenic potential. Data have accumulated to support a role for specific HPV types in the development of cancer, mostly cervical carcinoma. Genital HPV 16 and 18 have been predominantly found in malignant lesions and are called high risk HPV whereas HPVs 6 and 11 are related to benign warts of the genital and oral mucosa (EM de Villiers 1994 Curr Topics Microbiol Immunol 186: 1-12). In recent years, atypical HPV lesions of the genital tract are frequent in HIV-infected patients and can be used as markers for disease progression. Nevertheless, few authors describe HPV infections of the respiratory tract associated to AIDS. We describe here a case report of a non-characteristic respiratory HPV lesion. A woman 38 old years was HIV infected by sexual transmission and diagnosed since 1992. Opportunistic diseases have begun one year before the study (1997) with two episodes of Pneumocystis carinii, which were treated. After wards, she presented symptoms of disphony, disphagy and progressive dispnea. Thorax RX was normal. At broncofibroscopy exam, it has been showed infiltrate subglottis lesion, which caused 50% of tracheal lumen reduction. The lesion had clinical aspect of lymphoma. During broncoscopy, a biopsy was taken but the remission of the lesion was tried unsuccessfully twice because of its hiding localization. Finally the patient had the lesion taken off by laser surgery under general anesthesia. Histopathological findings have included acanthosis, papillomatosis and koilocytosis. The case was diagnosed as squamous cell papilloma. It was compatible with HPV infection and showed absence of malignancy. To detect and type HPV, in situ hybridization assay was done. Biotinyled probes 6/11, 16/18 and 31/33/35 were used. HPV 6b, 11, 16 and 18 DNAs were kindly provided by Dr EM de Villiers (Referenzzentrun für Humanpathogene Papil-lomviren, Heidelberg, Germany). HPVs 31, 33 and 35 probes were available in a hybridization kit (Pathogene -DNA Probe Assay for Identification of HPV - Enzo Diagnostics Inc, NY, USA). Briefly, 5 µm sections were cut onto Aminopropyl triethoxysilane (Sigma) coated slides, heated at 60oC for 2 hr and stored at room temperature (RT). Sections were deparaffinized in two changes of xylol and two changes of 100% ethanol. Nucleic acids were unmasked by digestion with 0.5 mg/ml proteinase K (Sigma) at 37°C for 15 min. The hybridization mixture contained 5xSSC, 5% polyethileneglycol, 0.1 mg/ml denatured carrier DNA (herring sperm), biotinylated probes (1 µg/ml) and 50% deionized formamide for high stringent conditions. Each section was layered with 20 µl of hybridization mixture under a coverslip, denatured by heating at 92°C for 10 min on a heating block, and hybridized at 37°C for 2 hr. Coverslips were removed by soaking the slides in 4xSSC at RT for 10 min. The slides were further washed in 0.1xSSC/50% formamide, 4xSSC and phosphate buffered saline pH 7.2 (PBS) at RT for 10 min each. The DNA-DNA hybrids were visualized by using streptavidin-alkaline phosphatase complex at RT for 30 min. Unbound conjugate was removed by two washes in Buffer 1 (0.1 M Tris HCl, 0.15 M NaCl, pH 7.5) for 10 min and once in Buffer 3 (0.1 M Tris HCl, 0.1 M NaCl, 50 mM MgCl2, pH 9.5) for 5 min at RT. The slides were then incubated in Nitro Blue Tetrazolium-Bhrome Clore Indolyl Phosphate (NBT-BCIP) dissolved in Buffer 3 at RT for 30 min in the dark. Slides were rinsed in distilled water to stop reaction, air dried and mounted in glycerin jelly without counterstaining. HPV-positive and negative tissue biopsies were used as controls in every experiment. The patient was infected with HPV 16/18. The importance of these findings is related to the fact that respiratory papillomatosis are rarely found even in the normal population. H Lindbergh and O Elbrond (1990 Clin Otolaryngol Allied Sci 15: 125-131) found a prevalence of 3.8/million in a Danish subpopulation. The most frequent site of the infection is the larynx. Because of its recurrent nature, laryngeal papillomas are also referred as recurrent respiratory papillomatosis. The most common presenting symptom of respiratory papillomatosis is hoarseness or voice changes. Several studies proposed that genital infected mother probably transmits the virus to child during birth, and appearance of the warts can occur at any age, although children under the age of 5 years are at the highest risk of developing disease (M Strong et al. 1979 p. 88-98 in GB Hearly & TJI McGill (eds), Laringo-tracheal Problem in Pediatric Patient, Tomas, Ilinois). The adult onset cases occur between 20 and 40 years of age but probably the infection is not related to birth. Despite the age, HPV 6 and 11 types are detected from nearly all respiratory papillomas (P Mounts & K Shah 1984 Prog Med Virol 29: 90 -114). Our findings involving a lesion caused by HPV have many unusual aspects: its uncommon appearance, rare localization (epiglottis), and HPV types rarely found in respiratory tract. The possibility of maternal or self-transmission is unlikely because the patient did not report HPV infection in her mother's genital tract or in herself. However, infection by HPV 16/18 types could be established in the respiratory tract due the immunodeficient condition of the patient by sexual transmission. It is worth to emphasize the importance of the specific laboratory diagnosis to elucidate these new pathologies associated to AIDS in order to establish an accurate management of the patients. Fig. 1: papillomatosis aspect of the respiratory epithelium biopsy with intense koilocytosis. Magnification: 400X. Fig. 2: epiglottis tissue showing nuclear signs of HPV 16/18 type infection detected by in situ hybridization. Magnification: 400X. Arrows indicate HPV DNA detection. Financial support: CNPq Copyright 1998 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc98219b.jpg] [oc98219a.jpg] |
| |||||||||

{kind=link}
{kind=link}