 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Vol. 94(1): 13-18 Risk Factors for Human T Cell Lymphotropic Virus Type I among Injecting Drug Users in Northeast Brazil: Possibly Greater Efficiency of Male to Female Transmission Inês Dourado/+, Tarcísio Andrade*, Catherine L Carpenter**, Bernardo Galvão-Castro*** Instituto de Saúde Coletiva Universidade Federal da Bahia, Rua Padre
Feijó 29, 4o andar, 40110-170 Salvador, BA, Brasil *Centro
de Estudos e Terapia do Abuso de Drogas, UFBA, Salvador, BA, Brasil **Department of
Preventive Medicine, USC School of Medicine, Los Angeles, CA, USA ***Centro de
Pesquisas Gonçalo Moniz-Fiocruz, Salvador, BA, Brasil Received 24 June 1998; Accepted 3 November 1998
Code Number:OC99006
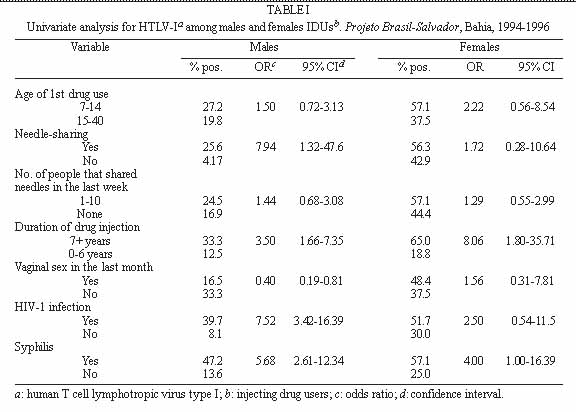
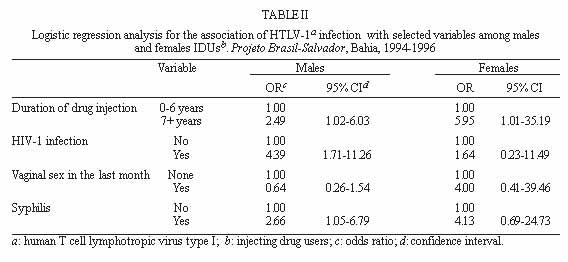
It was observed in the city of Salvador, State of Bahia, the highest seroprevalence of human T cell lymphotropic virus type 1 (HTLV-I) infection in Brazil as demonstrated by national wide blood bank surveys. In this paper, we report results of an investigation of drug use and sexual behavior associated with HTLV-I infection among male and female injecting drug users (IDUs) in Salvador. A cross sectional study was conducted in the Historical District of Salvador from 1994-1996 (Projeto Brasil-Salvador) and 216 asymptomatic IDUs were selected using the snowball contact technique. Blood samples were collected for serological assays. Sera were screened for human immunodeficiency virus (HIV-1/2) and HTLV-I/II antibodies by ELISA and confirmed by Western blot. The overall prevalence of HTLV-I/II was 35.2% (76/216). The seroprevalence of HTLV-I, HTLV-II and HIV-1 was for males 22%, 11.3% and 44.1% and for females 46.2%, 10.3% and 74.4% respectively. HTLV-I was identified in 72.4% of HTLV positive IDUs. Variables which were significantly associated with HTLV-I infection among males included needle sharing practices, duration of injecting drug use, HIV-1 seropositivity and syphilis. Among women, duration of injecting drug use and syphilis were strongly associated with HTLV-I infection. Multivariate analysis did not change the direction of these associations. Sexual intercourse might play a more important role in HTLV-I infection among women than in men. Key words: human T cell lymphotropic virus type I/II (HTLV-I/II) - human immunodeficiency virus type 1 (HIV-1) - injecting drug use - snowball sampling - Bahia - Brazil Human T-lymphotropic viruses (HTLV-I/II) and human immunodeficiency virus (HIV) were identified during the years 1979-1985 (Poiesz et al. 1980). HTLV-I and most likely HTLV-II can be transmitted through sexual contact, blood transfusion, sharing of injecting equipment, and from mother to child primarily through breast feeding (HTLV European Research Network 1996). Individuals infected with HTLV-I develop antibodies to the virus and become lifelong carriers. In addition, HTLV-I is associated with multiple pathologies such as adult T-cell leukemia and lymphomas, HTLV-I associated myelopathy or tropical spastic paraparesis, arthrits and uveites (Poiesz et al. 1981). However, there is no clear evidence until now of diseases associated with HTLV-II (CDC 1990, Hesran et al. 1994). It is well known that injecting drug use (IDU) is an important risk factor for infection with known human retroviruses. Approximately 80 countries have documented HIV infection associated with the use of drug injection and 40 other countries have reported patterns of injecting drug behavior (Stimson 1995, Des Jarlais et al. 1996). HTLV-I/II were first recognized among IDUs in 1984 (Tedder et al. 1984). Reported seroprevalence rates of HTLV-I/II among this group range from as low as 0.4% to 53% in the United States. In Europe, a recent review article on the epidemiology of HTLV-I reported a wide variation across selected groups and higher rates up to 18% among IDUs (Taylor 1996). Differences in study design, and in the testing algorithms are possible explanations for the wide rate variation (Lee et al. 1989, 1990, Khabbaz et al. 1990, Feigal 1991). In the Unites States and Europe, HTLV-II represents the majority of HTLV infections among IDUs (Briggs et al. 1995). Seroprevalence studies in Latin America have identified important geographic areas of HTLV transmission. The reported prevalence in a study with sample from the general population in Venezuela was 6.8% (Merino et al. 1984). In Chile, of 954 samples from blood donors, 7 (0.73%) were confirmed positive for HTLV-I/II (Vasquez et al. 1991). In the Amazon region, HTLV-II has been observed to be endemic among indigenous population of Brazil, particularly between the Kayapo indians with reported infection rate of 32.3% (Ishak et al. 1995). HTLV-I infection and its associated pathologies have been described by many investigators in Brazil (Pombo de Oliveira et al. 1990, Moreno-Carvalho et al. 1992, Moreira et al. 1993, Gabbai et al. 1993). A national survey with samples from blood banks reported the highest rate of 1.35% in Salvador, the capital of the State of Bahia, a city located in the Northeast region (Ferreira Jr et al. 1994, Galvão-Castro et al. 1997). Furthermore, other studies demonstrated the presence of these infections among selected groups in Brazil (Araujo et al. 1994, de Carvalho et al. 1996, Bellei et al. 1996). A seroprevalence study of retrovirus infection conducted in Salvador among IDUs, demonstrated high rates of HIV-1 (49.5%), HTLV-I (25.5%) and HTLV-II (8.8%) (Andrade et al. 1998). In this paper, we report results of an investigation of drug use and sexual behavior associated with HTLV-I infection among male and female IDUs in Salvador. MATERIALS AND METHODS Study population - This is a cross sectional study conducted in the colonial district of Salvador, between August 1994 and September 1996. This investigation is part of a multicenter HIV seroprevalence and behavioral study among IDUs in five Brazilian cities (Projeto Brasil-Salvador). Salvador, the capital of the State of Bahia, is a city with approximately 2.5 million inhabitants. Its population, is roughly 80% black or racially mixed. The colonial district known as Pelourinho, is located in the Historical Center of Salvador, with approximately 20,000 inhabitants of whom 30% were below 14 years old at the time of the study. The area is now being renovated after years of architectural and social deterioration. Despite Pelourinho being an important cultural center, especially for Afro-brazilian culture, it is also surrounded by areas of marginality, prostitution, drug use and drug traffic. The study group was identified among individuals who reside or frequent the Historical District using snowball sampling technique. The snowball technique provides a study sample based on referrals made by individuals who shared or know others who have the characteristics to be considered in the investigation (Biernack & Walford 1981, Lopes et al. 1996). Therefore, drug dealers and drug users were contacted in the streets of Pelourinho by trained research assistants, and were invited to act as mediators between potential participants and investigators. The majority (70%) of the study group were reached on the streets. Thirty percent were brought to the Drug Abuse Center by other IDUs to participate in the study. None of them were in drug treatment. Eligibility criteria for the study participation included reported drug injection in the last six months and age 15 years or older. The participants were interviewed by trained research assistants who looked for "tracks" and/or broken veins in order to confirm the IDU status of the candidate. The interviewer explained the objectives of the study, clarified any doubts and asked for their signature on the consent form. The questionnaires were adapted from the World Health Organization Multicity IDU Study (WHO 1993). Data on demographics, sexual behavior, attitudes and drug use practices were obtained and 10 ml of blood collected for serological assays. Laboratory methods - Sera were screened for HIV-1/2 and HTLV-I/II antibodies by ELISA [Abbott HIV-1/2, 3rd generation Plus EIA, Delkenheim, Germany and HTLV-I (rp21e enhanced), EIA, Cambridge Biotech Corporation, Worcester, MA, USA respectively] and confirmed by Western blot [HIV-1 Cambridge Biotech Corporation, Worcester, MA, USA and HTLV Blot 2.4 Genelabs Diagnostics (GLD), Science Park Drive, Singapore respectively]. The GLD HTLV Blot 2.4 also discriminates the seroreactivity to HTLV-I and HTLV-II and consequentely differentiates the type of infection. Evidence for the presence of Treponema pallidum infection was initially evaluated by serum reactivity to non-treponemal cardiolipin antigen (VDRL Behring, Marburg, Germany). VDRL positive samples were further tested by T. pallidum indirect immunofluorescence (FTA, Behring, Marburg, Germany). Data analysis - Frequency distributions were determined for each variable including mean, median and standard deviations for continuous variables. Crude odds ratios (OR) and 95% confidence intervals (CI) that measured the association of selected variables and HTLV-I infection were calculated from 2x2 tables (Fleiss 1981). Multiple logistic regression models computed adjusted estimates of potential risk behavior to HTLV-I infection. The statistical package (SAS 1995) was used to perform the different steps of the analysis. RESULTS Eighty two percent (177) of the study sample were males and 18% (39) were females. They reported injecting mainly cocaine. The seropreva-lence of HTLV-I, HTLV-II and HIV-1 was for males 22%, 11.3% and 44.1% and for females 46.2%, 10.3% and 74.4% respectively. HTLV-I was detected in the majority (72.4%) of HTLV positive IDUs. Further descriptive data analysis was reported elsewhere (Dourado et al. 1998). Briefly, the mean age at enrollment was 24.6 years and 27.4 years for males and females respectively and the mean age at first intravenous drug use was 16 years for both. The median duration of intravenous drug use was six years for males and eight years for females. Most of the study group were low income IDUs with one to two years of education and an illegal source of income such as robbery and/or drug traffic. Table I presents univariate analysis for the association of HTLV-I infection with behavior variables, HIV infection and syphilis. For males, HTLV-I was associated with needle sharing practices (OR, 7.94; 95% CI, 1.32-47.6), duration of injecting drug use (OR, 3.30; 95% CI, 1.60-6.80), no reference to vaginal sex in the last month (OR; 2.52; 95% CI, 1.23-5.18) and syphilis (OR, 5.68; 95% CI, 2.61-12.34). HTLV-I infection was highly associated with HIV-1 infection (OR, 7.52; 95% CI, 3.42-16.39). The OR for number of people that shared needles with in the last week was 1.44 but the 95% confidence intervals included the null value. Men reporting sex with another men ever in their lifetime (72/105) was not associated with HTLV-I infection (data not shown). Among women, HTLV-I was associated only with duration of injecting drug use (OR, 6.58; 95% CI, 1.58-27.78) and syphilis (OR, 4.00; 95% CI, 1.00-16.39). The OR for number of people that shared needles with in the last week, vaginal sex in the last month and HIV-1 infection was in the direction of a positive association with HTLV-I infection (OR=1.29; OR=1.56; OR=2.50 respectively), but the 95% confidence intervals were wide and imprecise. A significant linear trend of HTLV-I infection was demonstrated for increasing duration of injecting drug use for both males and females (Figure). Table II shows multiple logistic regression model results for males and females. Regarding women, duration of injecting drug use remained a correlate of HTLV-I infection for women (OR, 5.95; 95% CI, 1.01-35.19). Also, the association between vaginal sex in the last month and syphilis with HTLV-I was positive (estimated ORs around 4.00), but not statistically significant. On the other hand, duration of injecting drug use (OR, 2.49; 95% CI, 1.02-6.03), HIV-1 infection (OR, 4.39; 95% CI, 1.71-11.25) and syphilis (OR, 2.66; 95% CI, 1.05-6.79) remained statistically significantly associated with HTLV-I infection among males. Vaginal sex in the last month had an estimated OR below the null value, but not statistically significant. Age at enrollment in the study was strongly correlated (60%) with duration of IDU. Age when added to the logistic regression model did not appreciably change the ORs between various risk behaviors and HTLV-I and was therefore not included. DISCUSSION Most studies of IDU have been carried out in clinical settings where generalizability of results to other groups is of limited ability. In order to improve the representativeness of our study, we used the snowball sampling technique, a method extensively used in studies of hidden populations. High levels of HTLV-I, and HIV-1 infection among males and females IDUs was found in Salvador. In the United States (US), Khabbaz et al. (1990), documented seroprevalence of HTLV-I/II among IDUs in eight US cities ranging from 0.4% to 17%. Lee et al. (1989), reported sero-prevalence from 8.3% in Brooklyn, New York, to 24.3% in New Orleans. Furthermore, in the US, HTLV-II represents the majority of HTLV infections among this group whereas our data demonstrated a prevalence of HTLV-I higher than HTLV-II suggesting an endemicity of HTLV-1 in this area of Brazil (Dourado et al. 1998). Incidence data have shown that in addition to injecting drug use activities, sexual behavior also plays a role in increasing the risk for HIV-1 infection. Futhermore, women may have a higher risk of acquiring HIV by means of sexual behavior than men (Nicolosi et al. 1992). These observed features of HIV-1 transmission are probably similar for acquiring HTLV-I infection among males and females. It has been hypothesized that HTLV is transmitted more efficiently from males to females during sexual intercouse which would in part explain the observed excess of prevalence among women relative to men. In Japan, a study on HTLV infection among couples, estimated a transmission efficiency of 60.8% from males to females compared to 0.3% from females to males (Kajiyama et al. 1986). In our study, it is possible that sexual intercourse in addition to drug use activities is playing a more important role in HTLV-I infection among women than in men. Evidence to support this hypothesis are the observations that the seroprevalence of HTLV-I infection was two times higher for women than for men; women had higher rates of syphilis (almost three times) than men and vaginal sex in the previous month was reported more frequently by women. The association of vaginal sex with HTLV-I infection did not reach statistical significant levels but the estimated OR was in the direction of a positive association. Among males the OR was in the other direction but also not statistically significant. Other studies with greater sample sizes are needed to investigate further the role of sexual behavior as a risk factor to HTLV-I infection among male and female IDUs. ACKNOWLEDGMENTS To the participation of the study subjects, to the assistance with data collection of Jane Montes, Monica Coutinho and Arlene Alves, to Noilson Gonçalves technical assistance with the assays. This study was supported by grants from the PNUD/National Coordination of STD and Aids/Brazilian Ministry of Health and the Brazilian National Research Council (CNPq) grant no. 520605/95-0. REFERENCES
Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99006c.jpg] [oc99006a.jpg] [oc99006b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}