 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 94(4),Jul./Aug. 1999: pp 537-542 Atypical Mucocutaneous Leishmaniasis Caused by Leishmaniabraziliensis in an Acquired Immunodeficiency Syndrome Patient: T-cell Responses and Remission of Lesions Associated with Antigen Immunotherapy Alda M Da-Cruz, Danilo V Filgueiras*, Ziadir Coutinho*, Wilson Mayrink**, Gabriel Grimaldi Jr***, Paula M De Luca, Sergio CF Mendonça, Sergio G Coutinho+ Laboratório de Imunidade Celular e Humoral, Departamento
de Protozoologia ***Laboratório de Pesquisa em
Leishmanioses, Departamento de Imunologia, Instituto Oswaldo Cruz,
Av. Brasil 4365, 21045-900 Rio de Janeiro, RJ, Brasil
*Serviço de Dermatologia, Hospital Universitário
Gaffrée-Guinle, Rio de Janeiro, RJ, Brasil **Departamento de
Parasitologia, Universidade Federal de Minas Gerais, Belo
Horizonte, MG, Brasil Received 4 September 1998
Code Number:OC99099 An atypical case of acquired immunodeficiency
syndrome-associated mucocutaneous lesions due to
Leishmaniabraziliensis is described. Many vacuolated
macrophages laden with amastigote forms of the parasite were found
in the lesions. Leishmanin skin test and serology for leishmaniasis
were both negative. The patient was resistant to therapy with
conventional drugs (antimonial and amphotericin B). Interestingly,
remission of lesions was achieved after an alternative combined
therapy of antimonial associated with immunotherapy (whole
promastigote antigens). Peripheral blood mononuclear cells were
separated and stimulated in vitro with Leishmania
antigens to test the lymphoproliferative responses (LPR). Before
the combined immunochemotherapy, the LPR to leishmanial antigens
was negligible (stimulation index - SI=1.4). After the first course
of combined therapy it became positive (SI=4.17). The antigen
responding cells were predominantly T-cells (47.5%) most of them
with CD8+ phenotype (33%). Very low CD4+
cells (2.2%) percentages were detected. The increased T-cell
responsiveness to leishmanial antigens after combined therapy was
accompanied by interferon-g
(IFN-g
) production as observed in the cell culture supernatants. In this
patient, healing of the leishmaniasis lesions was associated with
the induction of a specific T-cell immune response, characterized
by the production of Key words: human mucocutaneous leishmaniasis - acquired immunodeficiency syndrome - CD8+ cells - interferon-g - immunotherapy American tegumentary leishmaniasis (ATL) is a protozoan disease which affects skin and facial mucous membranes. Leishmaniabraziliensis is the most common species found parasitizing humans in Brazil. Since 1987, several reports of ATL patients with associated acquired immunodeficiency syndrome (AIDS) have revealed unusual immunophatological aspects of leishmaniasis (Coura et al. 1987, Dedet et al. 1995).. The majority of patients suffering from Leishmania-human immunodefiency virus (HIV) co-infection have shown atypical clinical pictures such as disseminated cutaneous leishmaniasis (Coura et al. 1987, Machado et al. 1992), visceral involvement due to dermotropic parasites (Hernandez et al. 1993), cutaneous involvement due to viscerotropic parasites (Rubio et al. 1997), unusual clinical presentation of cutaneous lesions (Daudén et al. 1996, Rubio et al. 1997) and mucosal lesions with abundant amastigote forms (Cimmerman & Gomes 1993, Echevarría et al. 1993, Sasaki et al. 1997). However, those patients may also develop the classical localized cutaneous lesions (Gonzalés-Rupérez et al. 1997). T-cell mediated immune responses have a strong influence on the immunological mechanisms involved in the outcome of leishmaniasis. Resolution of cutaneous lesions is associated with a well modulated T-cell response, while an exacerbated immune response seems to be responsible for severe mucosal lesions (Carvalho et al. 1985, Coutinho et al. 1996). On the other hand, the development of a specific depressed T-cell mediated immune response leads to diffuse cutaneous leishmaniasis (DCL) (Convit et al. 1972). Previous reports from our group describing a DCL-like picture in a patient with AIDS and leishmaniasis suggested that generalized immunosuppression produced by HIV infection was responsible for aggravation of the leishmanial infection, related to the inability of the T-cell-mediated immune response to control the spread of the parasite (Da-Cruz et al. 1992). In this report we present an immunological study of a patient with AIDS-associated leishmaniasis who was resistant to conventional therapy; however remission of lesions occurred after antigen immunotherapy. Convit et al. (1987), Mayrink et al. (1992) and Genaro et al. (1996) have shown that immunotherapy with subcutaneous injections of whole killed promastigote antigens, associated or not with BCG, have produced healing of lesions in human ATL, even in drug resistant patients. In this particular patient, remission of lesions was achieved after combined immunochemotherapy. The improvement of the lesions was accompanied by the development of a T-cell response to leishmanial antigens, in which CD8+ cells constituted the majority of the stimulated T-cell subpopulation. Interferon-g (IFN-g ) was also detected in the culture supernatants. MATERIALS AND METHODS Immunochemotherapy - The patient was treated with a combined immunochemotherapy. As an immunotherapeutic agent, we used the LeishvacinÒ (Biobrás, Montes Claros, MG, Brazil) that consisted of a pool of killed promastigotes from five Leishmania strains at a final concentration of 240 m g/ml protein nitrogen (Mayrink et al. 1992). The antigens were injected subcutaneously at a daily dose of 0.5 ml, during three 10-day courses with 10-day intervals. Initially, increasing doses from 0.1 ml up to 0.5 ml were used during the first five days, followed by a 0.5 ml dose during the last five days (Genaro et al. 1996). Antimonial therapy (15mg Sb5+/Kg of body weight of N-methyl glucamine) (GlucantimeÒ , Rhodia) was administrated concomitantly with immunotherapy. Characterization of the T cell responses elicited by
L.braziliensis antigens stimulation in vitro - The
lymphoproliferative response (LPR) assays, measured by
3H-thymidine uptake, were performed as described
elsewhere (Da-Cruz et al. 1994). Results were expressed as
stimulation indices (SI) defined as the mean counts in wells
containing antigen or mitogen divided by the background (mean
counts in non stimulated wells). Indices equal to or higher than
2.5 were considered positive. In parallel, leishmanial
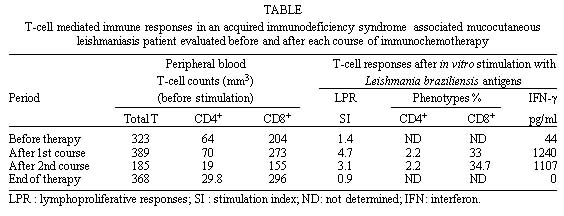
antigen-reactive CASE REPORT A case of mucocutaneous leishmaniasis associated with AIDS in a 53 year-old male patient is reported. He was born in a rural area of Brazil and had an ulcerative lesion on the foot forty years ago. By that time, he was treated with sulphonamides and bismuth. The lesion was healed one year later, but the diagnosis of leishmaniasis was not established. By the time of this report he was living in the city of Rio de Janeiro for 35 years and had recently moved to an endemic area of leishmaniasis localized in the periphery of the city. The patient then presented a papular lesion on the mucous membrane of the nose. The disease progressed to ulcerative and oedematosous lesions on nasopharynx. Thereafter, the lesions extended to soft palate, upper lip and contiguous skin of the nose. The histopathological examination of a nasal lesion biopsy sample stained with haematoxylin and eosin demonstrated a chronic inflammatory infiltrate containing mononuclear phagocytes, plasma cells and lymphocytes. There was accumulation of many vacuolated macrophages laden with amastigotes. Parasites were isolated from the lesion and characterized as L.braziliensis by a radioimmune binding assay using species-specific monoclonal antibodies, as well as by enzyme electrophoretic analysis (Grimaldi Jr et al. 1991). There was no delayed type hypersensitivity (DTH) response to leishmanial antigens (Montenegro´s skin test). Indirect immunofluorescence antibody test for leishmaniasis in the patient´s serum was negative for both IgG and IgM classes. Due to the unusual negative cellular and humoral immune responses to leishmanial antigens, the patient was further investigated for immunological disturbances. The suspicion of AIDS was confirmed by the detection of anti-HIV antibodies by ELISA and immunofluorescence assay (CDC 1993). At that time, the peripheral T lymphocyte counts were 1,418 T-cells per mm3, 158 CD4+ cells per mm3 and 1,059 CD8+ cells per mm3, with a CD4/CD8 ratio of 0.15. Antiretroviral therapy was started with AZT (zidovudine). Six months later DDI (didanosine) therapy was started due to persistence of very low lymphocyte counts. There was no history of symptoms suggestive of any AIDS-related disease. The antimonial therapy, consisting of three 10-day courses of 20 mg Sb5+/kg body weight of N-methyl glucamine (GlucantimeÒ , Rhodia) injected intramuscularly with 10-day intervals was considered unsuccessful, despite an initial improvement, because the lesions relapsed after therapy. A course of amphothericin B (FungizonÒ , Squibb, 2.5 g total cumulative dose) also failed to result in improvement. Due to the partial resistance to the classical chemotherapy (antimony and amphotericin B), with persistence of lesions, we decided to start a combined immunochemotherapy (antigen + antimony). RESULTS Clinical follow-up - After the first course of combined immunochemotherapy, there was clinical improvement of the mucosal lesions, with a striking reduction of oedema and nasopharyngeal obstructive symptoms. At the end of therapy, the leishmanial lesions displayed only slight signs of activity, although the patient presented oral candidiasis. Table shows the results of peripheral blood lymphocyte counts before the combined immunochemotherapy and at the end of the therapy. Four months later, the patient died due to AIDS-related diseases (including central nervous system cryptococcosis) without any lesion indicative of leishmaniasis. Immune responses to L.braziliensis antigens - The analysis of LPR to L.braziliensis antigens before the combined immunochemotherapy showed very low T-cell stimulation indices ( Table). After the first course of the combined therapy, the LPR to leishmanial antigens became positive (SI = 4.7). A similar result, although showing a small decrease (SI = 3.1), was observed after the second course of combined therapy. After the third course of combined therapy, the stimulation index returned to the low level found before therapy ( Table). The mean background (non stimulated cultures) was cpm = 213 ± 198. The LPR indices to concanavalin A remained very low (SI<2.5) during the whole observation period. After the first course of the combined therapy, the L.braziliensis stimulated PBMC cultures showed 47.5% of leishmanial-reactive T-cells with the majority being CD8+ cells (33%) and very low percentage of CD4+ cells ( Table). Similar results were found when the phenotypic analysis was performed after the second course of combined therapy. Before the onset of the combined therapy and after the third course, no phenotypic analysis was performed because the number of responder cells in the cultures were too low. The IFN-g levels in the Leishmania stimulated PBMC culture supernatant were 44pg/ml before the onset of combined therapy and increased to 1240pg/ml after the first course, remaining at this level after the second course ( Table). The increase of IFN-g levels in the culture supernatants were accompanied by an increase in the lymphoprolif-erative responses. However, the results of both assays showed a marked decrease after the third course ( Table). Increasing LPR indices and IFN-g production after the first and second course apparently were not associated with CD4+ cell stimulation, since very low percentages of these cells (2.2%) were observed in stimulated cultures during the whole period of study. DISCUSSION In HIV-infected subjects there are few descriptions of ATL patients with mucosal involvement associated or not with cutaneous lesions (Machado et al. 1992, Cimmerman & Gomes 1993, Echevarría et al. 1993, Sasaki et al. 1997). In the case reported here, the mucocutaneous leishmaniasis was apparently the first infectious disease to develop during immunodeficiency, even before the common AIDS related-diseases (CDC 1993). It was not possible to establish whether the Leishmania infection was a result of reactivation of a previous infection or due to a primary infection, because the patient had one skin scar suggestive of cutaneous leishmaniasis but had also recently moved to an endemic area of leishmaniasis transmission. The presence of abundant amastigote forms parasitizing lesions and the absence of a DTH to leishmanial antigens seem to be related to a generalized immunosuppression. These features are not observed in immunocompetent L. braziliensis ATL patients where parasites are seldom observed in the mucosal lesions and are not commonly isolated in cultures. Moreover, a strong hypersensitivity to leishmanial antigens is usually observed in mucosal leishmaniasis patients (Carvalho et al. 1985). Some authors (Echevarría et al. 1993, Daudén et al. 1996) have described patients refractory to classical antimonial therapy. The reported patient displayed mucocutaneous lesions that did not recover completely when conventional drugs, such as antimonial or amphothericin B, were administered. The combined therapy of antimonial associated with immunotherapy (whole leishmanial promastigote antigens) was considered successful since the lesions improved and remained healed until the death of the patient caused by other AIDS-associated infections. In immunocompetent ATL patients, the use of crude leishmanial antigens as immunotherapy has also yielded good results, leading to lesions healing (Convit et al. 1987, Mayrink et al. 1992). However, the mechanisms by which the immunotherapy can lead to cure remain to be established. Immunization with infectious agent antigens has been associated with an increase, although transient, in HIV viral load (Ortigão-de-Sampaio et al. 1998). Apparently the immunotherapy did not aggravate the immunosuppression state of this patient. When the diagnosis of leishmaniasis was made, the patient already displayed CD4+ counts under 200 cells per mm3. The use of antiretroviral therapy did not improve the immunosuppression since CD4+ cell counts persisted at low levels even when the leishmanial lesions healed after the immunochemotherapy. The importance of cellular immune responses in the outcome of leishmaniasis has been well established in human (Convit et al. 1972, Coutinho et al. 1996) and experimental studies (Scott & Farrell 1998). The inability of T-cell-mediated immune responses to control the spread of the parasite could lead to atypical and severe clinical forms and may contribute to an unresponsiveness to anti-leishmanial drugs (Da-Cruz et al. 1992, Alvar et al. 1997, Badaró 1997). It has also been reported that reactivation of visceral leishmaniasis appears more frequently in patients with CD4+ counts less than 200 cells per mm3 (Alvar et al. 1997, Badaró 1997). Previous studies in human patients infected with L.braziliensis (Da-Cruz et al. 1994) have shown a tendency of an increasing percentages of Leishmania-reactive CD8+ T-cells and IFN-g production after healing lesions. Volunteers vaccinated with crude leishmanial promastigote antigens also had in vitro production of IFN-g and positive LPR to Leishmania antigens. The majority of antigen responder cells in vitro had also a CD8+ T-cell phenotype (Mendonça et al. 1995). Those observations, taken together, indicate that a profile of T-cell responses characterized by higher proportions of reactive CD8+ T-cells and IFN-g production can be associated with cure and protection (Coutinho et al. 1996). In this patient suffering from AIDS-associated leishmaniasis, although LPR to leishmanial antigens became positive after the first course of the combined therapy, the Leishmania-reactive CD4+ cell counts response remained consistently low and the majority of Leishmania-reactive T cells belonged to the CD8+ phenotype. These findings point to the possibility that antigen-responding CD8+ T cells are able to mediate the mechanisms for cure of the leishmanial lesions, even when CD4+ T-cells are practically absent as it was the case in this particular patient. Moreover, the levels of IFN-g in the supernatant of antigen-stimulated cultures after the combined therapy also became positive in association with increasing percentages of CD8+ responding cells. The possibility that other CD2+ cells (e.g., natural killer cells) were involved in the IFN-g production can not be rejected. Although the mechanisms by which Leishmania-reactive CD8+ T-cells contribute to the host defense are not well defined there is little doubt that intracellular microorganisms or soluble antigens can elicit a CD8+ T cell response (Kovacsovics-Bankowski & Rock 1995). It has been proposed that these cells can exert a protective role by direct cytolytic effect on parasitized macrophages (Conceição-Silva et al. 1994) and/or via lymphokine production, mainly IFN-g (Müller et al. 1993). The treatment of choice, the best dosage and the duration for AIDS-associated leishmaniasis therapy have not yet been clearly defined (Alvar et al. 1997). Other alternative treatments combining antimonial compounds with IFN-g have been reported in patients with AIDS associated visceral leishmaniasis, although with variable results (Gorgolas et al. 1993). It is possible that the combined therapy induces a specific T-cell activation with IFN-g production, influencing the outcome of the disease. However, in this case report, we can not be sure whether immunotherapy alone or their association with antimonial was responsible for the healing of lesions, because the previous antimonial therapy provided a partial but not sustained remission of lesions. The present results show that the healing of mucocutaneous lesions after the combined therapy was associated with the induction of a T-cell mediated immune response characterized by production of IFN-g and predominance of the CD8+ phenotype among the Leishmania-reactive T-cells. ACKNOWLEDGEMENTS To Dr Charles Woodrow for revising this manuscript. To
Dr Célia Rangel for contribution and to Mrs Rosangela
Pelegrino and Mrs Angelica Oliveira for their secretarial
assistance. REFERENCES Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99099a.jpg] |
| |||||||||

{kind=link}