 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 94(4),Jul./Aug. 1999: pp 543-547 Drug Resistance Patterns among Hospitalized Tuberculous Patients in Rio de Janeiro, Brazil, 1993-1994 FCO Fandinho, AL Kritski*, C Hofer*, H Conde Jr**, RMC Ferreira*, MG Silva***, LS Fonseca***/+ Departamento de Desenvolvimento Tecnológico e Produtos
Imunobiológicos, Fiocruz, Rio de Janeiro, RJ, Brasil
*Hospital Universitário Clementino Fraga Filho, Universidade
Federal do Rio de Janeiro, Rio de Janeiro, RJ, Brasil **Instituto
Estadual de Doenças do Tórax Ari Parreiras,
Niterói, RJ, Brasil ***Instituto de Microbiologia, Centro de
Ciências da Saúde, Bloco I, Universidade Federal do
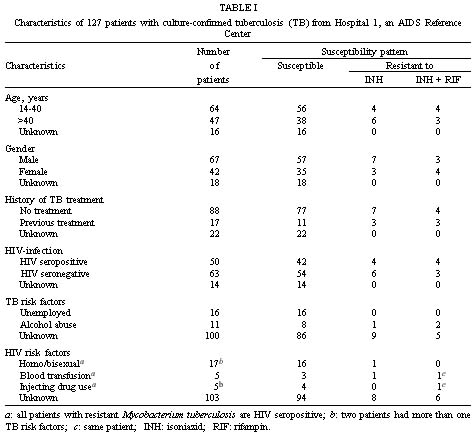
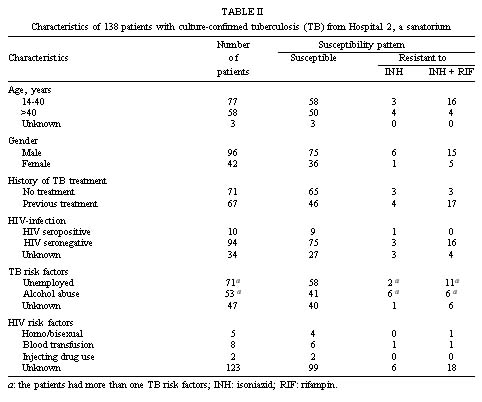
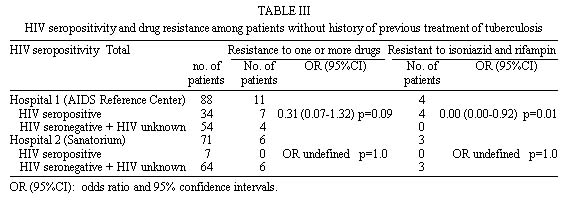
Rio de Janeiro, 21941-590 Rio de Janeiro, RJ, Brasil Grant support: CNPq, Faperj and Finep (Brazil). Received 26 October 1998 Code Number:OC99100 The purpose of this study was to analyze the prevalence and risk factors for drug resistance among hospitalized patients in two tertiary care centers, an acquired immunodeficiency syndrome (AIDS) reference center and a sanatorium, in Rio de Janeiro, Brazil. From 1993-1994, 389 patients were diagnosed as having tuberculosis (TB). Isolates from 265 patients were tested for in vitro susceptibility to rifampin and isoniazid. Resistance to one or more drugs was detected in 44 patients (16.6%) and was significantly more common among recurrent cases in both hospitals (p=0.03 in the AIDS center and p=0.001 in the sanatorium). Twenty seven patients (10.2%) had isolates resistant to both isoniazid and rifampin. Multi-drug resistance was associated with human immunodeficiency virus (HIV) infection among patients who had never been treated for TB. In conclusion, drug-resistant TB is high in hospitalized patients in Rio de Janeiro, especially among HIV infected patients. Therefore, measures to control TB and prevent nosocomial transmission need urgently to be set up in the Brazilian hospitals. Key words: tuberculosis - drug resistance - human immunodeficiency virus (HIV) infection - inpatients Tuberculosis (TB) continues to be a major threat to health throughout the world, with an estimated 8-10 million new cases and 3 million deaths annually (Kochi 1991). The global resurgence of TB has been accompanied by an increased frequency of multi-drug resistant Mycobacterium tuberculosis (MDR-TB) (Frieden et al. 1993, Pablos-Méndez et al. 1998). In the last years, the number of cases and institutional outbreaks of MDR-TB has dramatically increased in the United States and Europe, mostly involving human immunodeficiency virus(HIV) infected persons (Beck-Sagué et al. 1992, Edlin et al. 1992, Fischl et al. 1992). In developed countries HIV infection has been associated with primary drug resistance. In New York city, HIV infection is the main risk factor of primary MDR-TB (Riley 1993, Fujiwara et al. 1997). However, both the magnitude of this problem and the associated factors with drug resistance may vary considerably from country to country. In Brazil, the TB annual incidence rate is 58.4/100,000 inhabitants, with 90,664 new cases of TB diagnosed in 1995 (Ministério da Saúde 1996). Furthermore, the country has the second notified number of acquired immunodeficiency syndrome (AIDS) cases in the world (USAID 1996). In a recent national survey, including only outpatients, the prevalence of primary resistance to isoniazid and rifampin was 1% (Pablos-Méndez et al. 1998). However, little information is available on the resistance rate in patients treated in hospitals and the influence of HIV infection and other risk factors on the resistance of M. tuberculosis. We report here the analysis of the prevalence and risk factors for drug resistance among tuberculous patients hospitalized in an AIDS center and in a sanatorium in Rio de Janeiro, Brazil, during the period of 1993-1994. MATERIALS AND METHODS Patients - All patients with M. tuberculosis positive culture from any anatomical site between September 1993 and September 1994 from two Rio de Janeiro hospitals were included. Hospital 1 (Hospital Universitário Clementino Fraga Filho/Federal University of Rio de Janeiro), is a tertiary-care, 500-bed teaching hospital that serves as an AIDS Reference Center, whereas Hospital 2 (Instituto Estadual de Doenças do Tórax Ari Parreiras) is a sanatorium and a reference center for TB with 150 beds. Clinical data and demographic and social information, including previous TB treatment were obtained by assessment of medical records, patient examination and interview. After written consent was given, blood specimens were collected for HIV-1 testing. The serological tests were performed at Hospital 1 by Elisa (Organon Teknica, Boxtei, the Netherlands) with confirmation by Western blot (DuPont, Wilmington, DE, USA). Bacteriological procedures - Isolates on Loewenstein-Jensen were sent to the laboratory of the Institute of Microbiology of the Federal University of Rio de Janeiro. Only one isolate was included per patient. M. tuberculosis identification was carried out by standard biochemical and enzymatic tests (Vestal 1975, Ministério da Saúde 1995). Drug resistance tests were performed on Loewenstein-Jensen medium by the standard proportion method of Canetti et al. (1963) for isoniazid and rifampin. Resistance was reported when the percentage of colonies exceeded 1% of the growth on a drug free medium (control) as critical concentrations of 0.2 m g/ml for isoniazid and 40 m g/ml for rifampin. Multi-drug resistance was defined as resistance to the two anti-TB drugs tested. Statistical analysis - Analysis of data and significance tested by Yates and two tailed Fisher,s exact tests were performed by Epi Info version 5. RESULTS In total 389 patients were diagnosed as having TB by positive culture of M. tuberculosis. Isolates were available from 265 patients (68%); the other isolates had been either discarded due to contamination or were not viable. The overall prevalence of patients with resistant M. tuberculosis was 16.6% (44/265). Clinical and demographic data of the patients are given in Table I and Table II. Almost half of the patients were between 20 and 40 years of age in both hospitals. The male to female ratio was 1.6 (67/42) in Hospital 1 and 2.2 (96/42) in Hospital 2. HIV infection was detected in 50 patients (39.3%) from Hospital 1 and in 10 patients (7.2%) from Hospital 2. The association between patient characteristics and resistance to at least one drug (total resistance) or to both isoniazid and rifampin (multi-drug resistance) is also presented in Table I and Table II. Mono-resistance to rifampin was not observed. Prevalence of resistance did not differ significantly in the age or gender groups, except for MDR in patients with 14-40 years old in hospital 2 (p=0.04). Resistance to one or more drugs was approximately three times as common among patients with recurrent TB compared to those with no previous history of the disease in both hospitals (Hospital 1: 35.3% versus 12.5%, p=0.03; Hospital 2: 31.3% versus 8.4%, p=0.001). However, only in Hospital 2 a history of previous treatment was statistically associated with mdr (p=0.001). Twenty seven patients from Hospital 1 and 92 from Hospital 2 had an identified risk factor for drug resistance, such as belonging to a group known to be non compliant with therapy (unemployed and alcohol abuse), but no significant association between drug resistance and risk factors was observed. The comparative analysis between the two hospitals showed no difference in the resistance rate (p=0.52), (hospital 1: 17/127, 13.4%; Hospital 2: 27/138, 19.5%), although in Hospital 2 48% of the patients had recurrent TB, while in Hospital 1 only 13.3% of the patients had a history of previous treatment for TB. Also, the rates of primary (12.5% versus 8.4%; p=0.41) and secondary (35.3% versus 31.3%; p=0.63) resistance did not show any statistical difference between the two Hospitals. No difference was found between the resistance rates of the HIV negative or positive patients from the two hospitals. Among patients who had never been treated for TB ( Table III), drug resistance to at least one drug in Hospital 1 was more common in patients with HIV infection (7/34 versus 4/54), although with no statistical significance (p=0.09). However, at the same hospital, it was found a statistical correlation with MDR and HIV infection, the four patients with MDR isolates were all HIV positive (p=0.01). Among the 71 patients from Hospital 2 who had never been treated for TB, only 7 were HIV positive and their isolates showed no resistance to the drugs tested. DISCUSSION The emergence of M. tuberculosis strains that are resistant to antimycobacterial agents, although not a new problem, has recently received increased attention due to the dramatic outbreaks of MDR in HIV-infected patients (Beck-Sagué et al. 1992, Edlin et al. 1992, Fischl et al. 1992, McGowan Jr 1995). Besides, MDR-TB is a worldwide problem in both immunocompetent and HIV-infected populations (Kochi et al. 1993, Pablos-Méndez et al. 1998). MDR-TB particularly presents challenges for therapeutics options and successful outcome. Resistance to multiple drugs varied by geographic region and acquired MDR is more common than primary MDR (Pablos-Méndez et al. 1998). In the city of Rio de Janeiro, TB incidence is very high, 160/100,000 inhabitants in 1995, similar to some African countries (Ministério da Saúde 1996). Recently, a survey of M. tuberculosis resistance among TB outpatients diagnosed in Primary Health Services of the city of Rio de Janeiro showed 17.2% of resistance to at lest one drug and 0.9% of MDR (Natal et al. 1997) and a national survey showed the same rate of MDR (0.9%) (Pablos-Méndez et al. 1998). However there is few information regarding drug resistance among inpatients and on the relationship between drug resistance and HIV infection (Pinto et al. 1996). The present survey represents the first attempt to describe drug-resistance patterns in patients from an AIDS reference center and from a TB sanatorium in Rio de Janeiro. The high resistance rate observed in this study could be explained by the characteristics of the patients which included HIV seropositivity, recurrent TB, diabetes and other co-morbidities. The relevance of the high rates of drug resistance and particularly of MDR lies in the subsequent management problems. Rifampin and isoniazid are the two most effective anti-tuberculous agents and the clinical response of the patients with MDR is poor and the mortality is high particularly in patients co-infected with HIV (Ellner et al. 1993, Jacobs 1994). The higher proportion of inpatients having MDR-TB is worrying also because of a high risk of nosocomial transmission, especially if the patients are hospitalized in setting where they are in close contact with immunocompromised patients with no biosafets procedures (Edlin et al. 1992, Beck-Sagué et al. 1992). We did not find a significant association between resistance to at least one drug and age and gender groups, HIV seropositivty, unemployment and alcohol abuse, however a significant association between MDR-TB and HIV infection in Hospital 1 and MDR-TB and recurrent TB in Hospital 2 was observed. These results could be due to the high prevalence of TB in the city of Rio de Janeiro or due to selection bias of the study: the study was performed in hospitals and may not represent the local pattern of drug resistant. Furthermore, the establishment of risk factors was based on the retrospective assessment of medical records and only one interview at the admission in the hospital. Considering the differences in the characteristics of patients from the two hospitals, an unexpected observations in this study was the finding of no statistical difference in the primary and secondary resistance rates between the two hospitals, although the high prevalence of HIV infection in Hospital 1 (39.3%) and the great proportion of patients with recurrent TB in Hospital 2 (48%). As found by others (Girardi et al. 1996, Fujiwara et al. 1997, Liu et al. 1998), a previous history of TB was associated with a significantly increased prevalence of drug resistance, but surprisingly this association was not found for multi-resistance in Hospital 1, an AIDS reference center, probably due to high rate of primary multi-resistance in HIV infected patients (11.7%; 4/34). Studies from the United States suggest that HIV infection may be a risk factor for MDR-TB, and could reflect recent infection with resistant organisms in immunosuppressed patients who may rapidly progress to overt disease (Frieden et al. 1993, Fujiwara et al. 1997, Liu et al. 1998). The high rate of primary resistance found in HIV patients should be the result of ongoing transmission from inadequately treated patients in the community. In conclusion, the level of resistance observed in our study suggests that MDR-TB is quite present in hospitals in Rio de Janeiro, and so, all isolates from tertiary care centers should be tested for drug susceptibility. Because of the high risk of nosocomial infection, there is an urgent need for a control program of TB and surveillance system in these Hospitals. REFERENCES Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99100b.jpg] [oc99100a.jpg] [oc99100c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}