 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
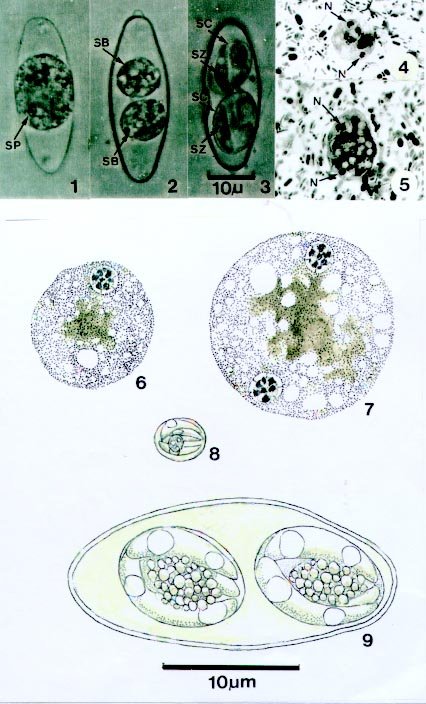
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 94(5),Sept./Oct. 1999: pp 611-613 RESEARCH NOTE Intestinal Parasites of Some Diarrhoeic HIV-Seropositive Individuals in North Brazil, with Particular Reference to Isospora belli Wenyon, 1923 and Dientamoeba fragilis Jepps & Dobell, 1918 Ralph Lainson/+, Beatriz AM da Silva/* Seção de Parasitologia, Instituto Evandro Chagas, Av. Almirante Barroso 492, 66090-000 Belém, PA, Brasil *Unidade de Referência-Aids, Secretaria Estadual de Saúde Pública, Rua Barão de Mamoré 271, Belém, PA, Brasil + Corresponding author. Fax: +55-91-226.1284.Received 30 October 1998 Code Number:OC99112 Supported by grant 049426 of the Wellcome Trust, London (RL). Key words: Isospora belli - Dientamoeba fragilis - Cryptosporidium - HIV seropositives - Pará - Brazil Faecal samples were examined from 34 adult HIV-seropositive individuals suffering from persistent diarrhoea in Belém, Pará, north Brazil. They were screened using a combination of direct microscopic examination (with and without Lugol's iodine), bright-field and phase-contrast microscopy of zinc sulphate flotation concentrates, and Giemsa-stained faecal smears. Of the protozoal parasites known to be causative agents of human diarrhoea, Isospora belli was detected in eleven individuals (32.3%), and Cryptosporidium parvum, Dientamoeba fragilis, Entamoeba histolytica, and Giardia lamblia each on single occasions (3%). Yeast cells were present in eight faecal samples (33%). The combinations of different protistans and helminths found in the 34 patients were as follows: seven with oocysts of I. belli, only; three with I. belli and yeast cells; one with I. belli, D. fragilis and eggs of Ancylostoma/Necator; one with G. lamblia and eggs of Trichuris trichiura; one with E. histolytica, Escherichia coli, Endolimax nana, G. lamblia and oocysts of C. parvum; three with T. trichiura, only; one with T. trichiura and yeast cells; one with Ancylostoma /Necator, only; one with larvas of Strongyloides sp., only; one with larvas of Strongyloides sp., eggs of Ascaris lumbricoides and Ancylostoma/Necator; four with abundant yeast cells, only. Ten had no detectable parasites. Diarrhoea in Aids patients has been attributed most frequently to C. parvum, and less frequently to I. belli. Cryptosporidiosis is a zoonotic disease, with reservoirs of C. parvum in domestic and wild animals: man-to-man transmission is of great importance, however, and oocyst-contaminated water can be a major source of infection. Among immunocompetent persons the prevalence of this coccidian has been shown to be highest (3-20%) in developing countries, whereas in Europe and North America it is in the region of only 1-2% and 0.6-4.3% respectively (R Fayer & PLB Ungar 1986 Microbiol Rev 50: 458-483). In Aids patients with diarrhoea in Maryland, USA, however, the figure reached 15-16% (BE Laughton et al. 1988 Gastroenterology 94: 984-993, PD Smith et al. 1988 Ann Intern Med 108: 328-333), and in São Paulo, Brazil, oocysts were detected in 19.1% of 131 Aids patients examined (FC Sauda et al. 1993 J Parasitol 79: 454-456). The coccidian I. belli is known only in man and was once regarded as an uncommon and non-pathogenic intestinal parasite. It is now established, however, that even in the immunocompetent individual the infection may be associated with gastrintestinal disturbances, and the advent of Aids has shown us that infection is much more common than previously supposed, particularly in the tropics. In São Paulo, for example, I. belli infection was recorded in 9.9% of the 131 Aids patients examined (FC Sauda et al. loc. cit.). Symptoms in Aids patients include fever, persistent diarrhoea and weight loss. A fatal outcome has been recorded in some cases (JP Dubey 1998 p. 325-326. In FEG Cox, JP Kreir, D Wakelin (eds). Topley & Wilson's Microbiology and Microbial Infections Vol 5, Parasitology, 9th ed. Arnold, London) Due to its amoeboid movement, lack of flagella and absence of cysts in its life-cycle, D. fragilis was originally included as an atypical member of the family Endamoebidae (Order Amoebida). It maintained this precarious position for many years, until RR Camp et al. (l974 J Protozool 21: 69-82) studied the organism's ultrastructure and, as a result, transferred it to the order Trichomonadida, to accompany the genera Trichomonas and Histomonas. D. fragilis appears to be restricted to man and was for long regarded as an uncommon and harmless inhabitant of the colon lumen. More recent observations, however, recorded an infection-rate of 115/219 (53%) in a religious community in Los Angeles, USA (V Millet et al. 1983 Digest Dis Sci 28: 335-339), and that 79% of 237 cases of D. fragilis infection in Washington, USA, were symptomatic and mostly with diarrhoea or loose stools (JH Grendon et al. 1995 J Trop Med Hyg 98: 309-315). On the other hand, workers in the University Hospital of Fortaleza, Ceará, Brazil detected only a single infection with D. fragilis among 2,605 patients showing other intestinal parasites (OO Riedal et al. Rev Med Univ Fed Ceará 26/27: 29-33. There are reports of D. fragilis present in the diarrhoeic faeces of Aids patients although, as is the case with Giardia and the intestinal amoebae, there is no conclusive evidence that it is any more pathogenic in these patients than it is in normal individuals. The yeast cells detected in eight of the faecal specimens in the present study were morphologically similar and budding was observed in all cases. Although the number of cells was low in the faeces of four individuals, the elevated number of yeast cells in four other individuals, in the apparent absence of other parasites, raised the suspicion that the fungus might be a cause of diarrheoa. Taxonomy of the yeast remained undetermined. The number of individuals examined in this survey is small, but we feel it important to draw attention to the high prevalence (32.3%) of I. belli compared with the low figure (3%) for C. parvum. Of the eleven I. belli infections, eight were diagnosed only after concentration of the oocysts by zinc sulphate flotation, an indication that this technique should always accompany other methods of examination. Whether or not the diarrhoea of the patient with D. fragilis was due to this parasite or I. belli is questionable. We feel it likely, however, that D. fragilis was at least a contributary cause, in view of the very large numbers of this parasite present in the faeces, and because D. fragilis may produce severe diarrhoea in immunocompetent persons. For these reasons, clinicians should include D. fragilis in the list of possible causes of diarrhoea in HIV-seropositive individuals and Aids patients. Many laboratory technicians, however, are unfamiliar with the appearance of this parasite, either living or in stained preparations, and it is still frequently mis-diagnosed as an amoeba. Furthermore, degenerating forms become motionless and full of small vacuoles which coalesce into a single large vacuole surrounded by a thin layer of protoplasm containing the two nuclei: such forms bear a striking resemblance to Blastocystis. Living D. fragilis are distinguished from trophozoites of E. histolytica by their smaller size (4-12 µm for rounded forms), absence of ingested erythrocytes, and `snail-like' locomotion. In stained smears they may appear larger, due to flattening. The most characteristic feature of D. fragilis is the predominance of bi-nucleate forms. Following iron-haematoxylin staining the nuclei are seen as spherical bodies, from 1-2.5 µm in diameter, with a central group of granules surrounded by a delicate nuclear membrane. The absence of a protective cyst means that D. fragilis is usually destroyed or severely distorted by flotation concentration methods _ one reason why fresh, Giemsa stained faecal smears are of utmost importance in diagnosis. Normal Giemsa staining (as for a blood film) is usually adequate for identification of D. fragilis by the experienced eye, but better results are obtained following fixation with aqueous Bouin's fluid and the use of a modified Giemsa method (R Lainson 1958 Trans R Soc Trop Med Hyg 52: 396-407). Pathogenic protozoa in the diarrhoeic faeces of some HIV-seropositive individuals. Figs 1-3, 9 - Isospora belli. Fig. 1: newly passed, unsporulated oocyst. Fig. 2: oocyst with two sporoblasts, one day later. Figs 3, 9: mature oocysts, after two days. Figs 4 -7: Dientamoeba fragilis. Figs 4, 5: binucleate forms in Giemsa-stained faecal smears. Figs 6,7: uninucleate and binucleate forms in iron haematoxylin stained smears. Fig. 8: mature oocyst of Cryptosporidium. SP: sporont; SB: sporoblasts; SC: sporocysts; SZ: sporozoites; N: nuclei. In the photomicrographs the 10 µ bar applies to Figs 1-5: in the line drawings the 10 µm bar applies to Figs 6-9. Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99112a.jpg] |
| |||||||||

{kind=link}