 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
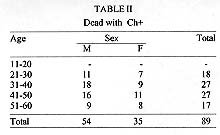
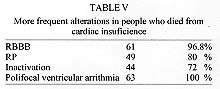
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 94,Suppl. I: pp. 317-320, 1999 Risk of Death Due to Chronic Chagasic Cardiopathy Enrique C Manzullo+, Roberto ChuitCentro de Investigaciones Epidemiológicas, Academia Nacional de Medicina, Argentina Paraguay 2028 4º piso, Buenos Aires, Argentina +Corresponding author. Received 9 June 1999 Code Number:OC99191 In this longitudinal study 5,710 people were included. The inclusion criteria were two positive serological results for Trypanosoma cruzi infection, 15 and 50 years old and no other demostrable diesease at the time of study. In the five year follow up 1,117 patients were lost. The follow up involved yearly evaluation of serology, clinical examination, X-ray of torax, and ECG, for 4,593 patients and 263 were contacted at home because they did not assist for their clinical consultant. Time average of follow up was 5.3 years. Eighty nine (1.5%) of the 4,593 patients died during the follow-up period, 63 (71%) by cardiac insufiency (CI) and 26 (29%) by severe ventricular arrithmias. Diagnosis of cardiomegaly was present in all the patients with diagnosis of CI and in 15 (5%) of the patients with diagnosis of arrithmias.The ECG alterations of these pacients show 61 right bundle brunch block (RBBB), associated or not with left anterior hemiblock (LAHB), 47 pathological Q wave and 70 primary repolarization alterations; 61 had polyfocal ventricular arrithmia. The death rate was similar in the sexes and was more frequent between 40 and 50 years of age. Information on 1,380 recuperated patients shows that 15 died with no previous symptoms and without medical assistance and were interpretate as sudden death. The latest ECG in three follow-up of these pacients indicates (before death) that only one had normal study and 14 presented 12 RBBB; 9 LAHB; 7 isolated ventricular arrithmia; 10 repolariz alterations; 2 patological Q wave, 10 patients of them with RBBB and repolariz alterations. In all the cases we had people between 35 and 43 years old, 9 men and 6 women. This study shows that in Chagas disease is possible to differenciate two risk groups. A low risk death group that have normal ECG and clinical evaluation during the follow up, and a high risk group associate ECG with RBBB and primary alterations of repolarization and/or inactivation zones with not anual clinical evaluation. Key words: Chagas disease - death chagasic - sudden death in Chagas Despite numerous studies examining the parasite vector host and environmental factors involved in Chagas disease (Alderete 1982, Prata et al. 1983) our knowledge of this condition is not yet complete. Taking in account the longitudinal study is the best method to make apports to the acknowledge of this sickness, of its risks, evolutive tendences and way of manisfestation,we have done it in the Cátedra de Enfermedades Infecciosas de la Facultad de Ciencias Médicas de la Universidad de Buenos Aires, Argentina, this study about chagasic cardiopathy. The investigation was due to the acknowlegde of chronic chagasic evolution cardiopathy, for residents outside the endemic zone with the following studies: clinical medical, X- ray, and ECG after a follow-up of 10 years. It was considered that a longitudinal study out side an endemic zone was possible and useful, because it can address the issue of "urbanization" of this sickness and possibly give us more information to confront it, in combination with the knowledge we have from endemic zone. To make possible this purpose, we should start with the basic questions that makes definition by itself and its escence, they were already considered when the project was made and were respected during the development. They are the following: (1) sample characterization; (2) definition and application of criteria for inclusion and exclusion; (3) details of the technique utilized and criteria for the interpretation; (4) presentation of advanced stage; (5) periodic evaluation of the results from the different national and international organizations vinculated with these subject. In this case we can mention the Instituto Nacional de Investigaciones Cardiovasculares, la Secretaría de Ciencia y Técnica de la Nación, WHO and OPS. The Doctors Romeu Cançado and Vanize Macêdo agreed to assess us because of an OPS request. Their presence made us scientifically stronger, permiting us to make corrections on time and they gave us their talent and friendship until today. In the present report we only consider those patients who died during the study. MATERIALS AND METHODS Two cardiologic consultories were installed with a secretary looking after them 5 hr per day from Monday till Friday. Two specialists were required from the professionals: specialist in cardiology and in infection sickness. The technical operation staff were trained to obtain information, obtain ECG and back up. Clinical histories and cards were designed and numbered as complementary information. This number was given to the patient. We had books with double entries: by correlative number, by date of entrance and surname of father and mother of the patients. People came in, by blood bank diagnosis, because they were relatives of the people assisted and had positive serology for Chagas disease confirmed by our center. They were not assisted by cardiological derivation. All of them had at least two positive serological reaction for Chagas disease: one of them was immunofluorescence. They were asked: sex, age, birth place (country, province, department, city); other resident place (three years or more in the same place); employee functions; personal and family backgrounds specially with relation to Triatoma infestans; epidemiologic, cardiologic, neurologic, endrocrinologic and digestive background; home characteristics and ecological aspects, and other sickness; basal ECG of 12 derivations. For the electrocardiographic diagnosis we began using Minessota (Rose & Blackburne 1968) code adding to it hemiblocks (Rosembaum et al. 1965). For the final analisys of these ECG the parameters became from "nomenclatura criterios de diagnóstico electrocardiográfico. Programa de Salud Humana" (Rosembaum et al. 1995). Chest X-ray (1.80 m distance): maximum cardiac silhuette accepted as normal was the relation cardiothoraccic less than 0.5; electroencefalogram when headache was present; oesophagus transit, gastrointestinal or colon in dysphagia, regurgitation and constipation of 3 or 4 days with interval egest as minimun; everybody was called for consultant at least once in a period of six months, even those who had non apparent disease; serological and electro-cardiographical studies were done twice. Periodically the results were statistically validated. Data that were not in the original project (new technique, concommitant sickness, new therapeutic) were the basis for other investigations without modifying the original scheme of this study. To have a better characterization of the population sample, a social study was performed, with predesigned interviews that were made by a sociology professional with experience in Chagas disease. In the larger follow-up of an open population, movement of the
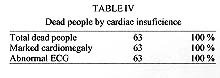
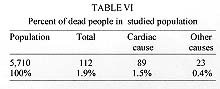
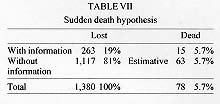
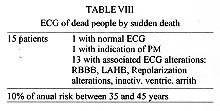
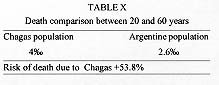
population is a reality we can Trying to loose less people and obtain more information from them we had several strategies, for example, giving them complete health assistance, and not only the follow-up of their Chagas disease, giving them all the medicine they needed free of charge, and giving them assistance cerficates, making appointments by letter to their homes or to their working place, therefore obtaining more effective attention on all the familiar group. This let us have more information on patients that abandoned follow-up, to each person we insisted to bring with him living family members with Chagas disease or to do the serological study when they were born in endemic zones, teaching them the importance of a periodic control. We asked them at each opportunity about the people they know in the follow-up, making appointments to those who were not being assisted or at least having information about people who had left the study. We studied the evolution of electrocardiografic alterations of those infected people that began with normal ECG and those that presented alterations in their first consult; they were identified by sex and age, the groups of highest risk by electrocardiographical evolution and risk of death. We've done a study of hospitalized dead people in our center, and in other institutions too and we elaborated a sudden death hypothesis; the death results of our population were compared with those of the "Programa Nacional de Salud para la Argentina"; evolutive similarity was established between the group of positive people treated with parasitological medicine and the group without treatment. RESULTS Five thousand seven hundred and ten persons were included and should have completed the five years of follow-up; 4,330 among those did it and 1,117 did not Table I). From the total follow-up 89 hospitalized patients died according to the distribution shown in Table II. Among those, 26 died from arrhythmias and 63 from cardiac insuficiency refractory to conventional treatments ( Table III). All of them had cardiomegaly in chest X-ray and pathological ECG ( Table IV). In Table V we distinguish that 89 dead patients represent 1.5% of the total population studied. Indeed 23 persons died during the follow-up by other causes than Chagas disease (accidents, tumours, and several other causes). These add 0.4% to the general mortality rate of the group ( Table V). As stated in Materials and Methods, we made every effort to ensure that patients attended their consults or at least to determine the reasons for their abandonment; 1,117 did not complete the five years follow-up (19.5%). Of 263 we know the causes of their abandonment: change of geographical place, non intereste, attended in other places and 15 died, we were told by their relatives ( Table VI). They did not need medical assistance during the previous 24 hr before death and is interpretated as sudden death ( Table VII). The results of the analysis performed on people who died by sudden death are shown in the Table VIII; where only one had normal ECG and this represents the 0.0017 of the sample and a mortality rate of 0.004%/ year. Another patient with pacemaker indication refused to be treated. The 13 patients left had in their last obtained ECG: right bundle branch block (RBBB), left anterior hemiblock (LAHB), repolarization primary alterations, inactivation zones, and in some cases isolated ventricular arrhythmias and low voltage. All of them died between 35 and 45 years of age. DISCUSSION Infected people with normal ECG presented a low risk of death (0.0045). We believe that this electrocardiographical result is a good prediction indicator, but periodic controls must be done. Indicator of bad prediction resulted to be for the people with the following associated ECG alterations: RBBB, LAHB, repolarization primary alterations, inactivations, with or without arrhythmias having or not low voltage. This group of patients had a yearly mortality rate of 10% and is defined as a high risk group. We permit ourselves to expose our sudden death hypothesis. We tried to obtain information about the 1,380 people that abandoned the follow-up with social visitors, by letter, by information given by their parents. We received 1,118 letters back due to wrong destination, change of address, and others who could not be encountered. If we consider that this group had the same destination as the other 263 from which we obtained information, we come to 78 possible sudden deaths (1.2 *1000/year). In Table IX to better expose our samples of mortality and letality we compare them with Argentina total mortality in people between 20 and 60 years of age from the "Programa Nacional de Estadìsticas de Salud". In Table X we compare the mortality in the Argentine population (2.6 * 1000/year) with our study (4 *1000/year). This means that people infected with Chagas have a higher risk of death than the rest of the population (53.8%). We made a comparison of our results with longitudinal studies of Macedo (1980), Pinto Dias (1982) and Puigbò (1969). We found coincidence in age of death caused by Chagas disease between 35 and 45 years, also by cardiac insufiency or sudden death and that a normal ECG is indicator of good prediction in chagasic infected people but always needs an additional periodic control. The group that showed severe alterations in ECG may be considered of risk, what comes uppon Reis Lopes (1981) question: sudden death may be expected or not? We believe these patients should be dectected by population studies because many of them are oligosymptomatic. They can be found in the perypheria of great cities where they had migrated from rural zones. Perhaps under such circumstances, our study in non-endemic zone could be useful. REFERENCES Alderete Nieto P 1982. Versión preliminar de Bibliografía Argentina sobre Enfermedad de Chagas. Programa de Formación de Recursos Humanos, Argentina. Macedo VO 1980. Forma indeterminada de doenca de Chagas. JBM. NO.OF THE JOURNAL? PAGES? Pinto Dias JC 1982. Doença de Chagas en Bambui, Minas Gerais, Brasil. Estudo Clinico Epidemioló-gico a Partir da Fase Aguda entre 1940 e 1982, Thesis, Belo Horizonte. Prata A, Pires E, De Sant Anna 1983. Bibliografía Brasileira sobre Doença de Chagas, Brasil. Puigbo JR 1969. Cuatro años de estudio longitudinal de una comunidad rural con endimicidad chagasica. Bol Of Sanit Panam 66: 112. Reis Lopez E 1981. Morte Súbita em Área Endêmica da Doença de Chagas. Sua importância Médico-Legal, Thesis, Facultade de Medicina do Triângulo Mineiro, Uberaba. Rose GA, Blackburne H 1968. Cardio-vascular survey methods, OMS Ser monog Nº 56, Geneva. Rosenbaum MB 1995. Criterios de lectura electro-cardiográficos. Programa de Formación en Recursos Humanos, Ministerio de Salud Pública Argentina, 1982, Reedición Consejo Argentino de Chagas, Sociedad Argentina de Cardiología. Rosenbaum MB, Elizari M, Lazzari J 1965. Los Hemibloqueos, Ed. Paidos, Buenos Aires. Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99191i.jpg] [oc99191d.jpg] [oc99191c.jpg] [oc99191g.jpg] [oc99191j.jpg] [oc99191f.jpg] [oc99191h.jpg] [oc99191e.jpg] [oc99191b.jpg] [oc99191a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}