 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
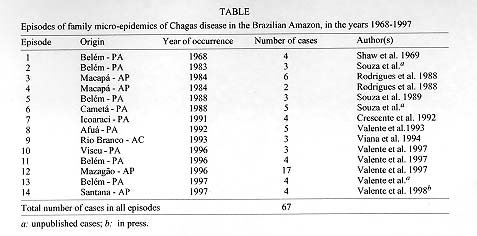
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 94, Suppl. I: pp. 395-398, 1999 Considerations on the Epidemiology and Transmission of Chagas Disease in the Brazilian Amazon Sebastião Aldo da Silva Valente+, Vera da Costa Valente, Habib Fraiha Neto Rodovia BR 316, km 7, s/no., 67030-070 Ananindeua, PA, Brasil Key words: Chagas diseasse - epidemiology - transmission - Brazilian Amazon + Corresponding author.Fax: +55-91-266.2016. E-mail: avalente.bel@zaz.com.br Received 9 June 1999 Code Number: OC99208 The Brazilian Amazon has long been considered a non-endemic area for Chagas disease, in spite of the well-known enzootic cycle involving a variety of wild mammals and triatomine bugs of this region (Rodrigues & Melo 1942, Deane 1964, 1967), whose natural environment has already been much altered by human activities in ways that are important for vector-host balance (Coura 1990, Fraiha Neto et al. 1995), necessiting attention and specific programs of epidemiological vigilance (Feitosa 1995). Chagas disease merits close attention at this time: there is growing number of cases that now exceeds one hundred cases in the past few years, the peri-domestic cycle of Trypanosoma cruzi is still in the adaptation phase in the region, and the time is opportune for the adoption of vector control measures. Chagas disease in the Brazilian Amazon is on the rise. Data from January of 1998, reveal 148 cases of which 121 were acute with 5 resulting in death (67 cases were associated with family episodes and 54 were not so associated) and 27 chronic cases. In terms of occurrence by state, 71 were in Pará (47.9%), 51 in Amapá (34.5%), 14 in Amazonas (9.5%), 9 in Maranhão (6.1%), and 7 in Acre (4.7%), not considering serological screening done in the region. It must be remembered also that these data represent only those notifications that came to the notice of the Instituto Evandro Chagas (IEC) and surely represent only the tip of the epidemiological `iceberg'. The State of Pará shows the greatest number of cases because it has in Belém facilities for diagnosis, while no cases were reported from the states of Roraima and Rondônia, possibly because of the lack of a notification system and of qualified medical personnel to recognize acute cases of Chagas disease. Of the types of transmission already observed, such as vectoral (Valente et al. 1993a, 1996) or transfusional (Valente et al. 1993c), transmission associated with family micro-epidemics merits further attention. This modality suggests transmission by ingestion. Episodes involving whole families, in the absence of triatomine vectors in the dwellings, make up a curious aspect of the disease in the Amazon region. Of the 121 cases recognized as acute, 67 (55.4%) are associated with family micro-epidemics and now account for 17 episodes ( Table). The possibility of infection by ingestion, although a mechanism still not well elucidated, appears to be the best hypothesis with which to explain the increasing number of these episodes (Fraiha Neto et al. 1995). This hypothesis finally appears to have explained in a recent episode studied in the State of Amapá (Valente et al. 1997) where 17 people became infected by drinking assai palm fruit juice. Sylvatic triatomine bugs attracted to electrical lights possibly fell into the machine used to process the juice consumed by the patients. A similar episode was related from the State of Paraíba (Shikanai-Yasuda et al. 1991). All of the patients reside at the Monte Castelo sawmill, locality called Rio Bispo, municipality of Mazagão, State of Amapá , and belong to four families that live in a villa within 50 m of each other. One resident recognized a triatomine bug in a sample collection shown to her, although she could not remember the species she had seen that year in one of the residences. None of the residents had ever been out of the state. The first symptoms appeared in November of 1996 in a child who showed fever, headaches, swelling of the legs, and yellowish discoloration of the skin. His mother took the child to the health posts at Porto de Santana and Macapá where no definite diagnosis could be given and where the patient was treated symptomatically. Shortly afterwards in January, two neighboring families, composed of eight people including both adults and children, sought health care at the Macapá municipal health service, complaining of high fevers, intense headaches, pain in the joints, and edema in the legs. They showed cutaneous reddening of the whole body, principally of the face, and swelling of the eyelids of both eyes. The reddening of the skin was most intense during the first week and later regressed until it took the form of violet spots that came and went at day intervals. A third family showed the same symptoms and sought the UMSM in Macapá. With the support of the IEC, several parasitological and serological examinations were done: QBC, blood smear, hemoculture, xenodiagnosis, IF and ELISA. Initially in17 people and later in two others forms identical to T. cruzi were seen. The IEC in Belém later confirmed this finding and the patients were treated. A fourth family, although residing at the same villa, was away at the probable time that the contamination took place. Among these families a common food habit is to consume assai palm fruit juice prepared daily at 20:00 hr in an electric machine and distributed to the families. The houses are surrounded by palm trees called urucuri (Attalea phalerata), recognized to be a habitat for wild triatomines in the region _30% of the examined trees (6/20) were infested with the triatomines Rhodnius pictipes and R. robustus, infected with trypanosomas identical to T. cruzi. The hypothesis of oral transmission now proposed for 14 episodes in the Brazilian Amazon was initially questioned because of the difficulty in demonstrating this type of transmission. This is because in most cases, patients were sent to us only long after initial infection and when epidemiological conditions were no longer favorable for investigation. In the Magazão episode, the largest in the region to come to our attention, transmission probably took place at night when on or more triatomines attracted to the electric lights fell into the juice being prepared in the machine and were ground up with the fruit pulp. Then the people who drank the juice became infected. The presence of metacyclic forms of T. cruzi in anal gland secretions of the opossum (Didelphis marsupialis), an animal with wild and peri-urban habits, can not be overlooked as an element favoring the possibility of oral transmission in some outbreaks (Lenzi 1984, Naiff et al. 1987). The traditional mechanism of transmission of Chagas disease involving contact with metacyclic forms in the feces of wild triatomines may not be the most common type of transmission in the Amazon where several other types of transmission appear to be occurring. The diversity of wild mammal reservoirs of the parasite in the region, such as D. marsupialis, Philander opossum, Dasypus novencinctus, Tamandua tetradactyla, Saimiri sciurius, Chiropotes satanas and bats of the genus Phylostomus (Deane 1964 1967, Deane et al. 1984, Valente et al. 1996) and of triatomines of the following species: R. pictipes, R. robustus, Panstrongylus geniculatus, P. lignarius, Eratyrus mucronatus and Microtriatoma trinidadensis, often found with high indices of natural infection with T. cruzi (Lainson et al. 1979, Miles et al. 1981), have suffered devastation of their habitats, giving rise to their attraction to artificial lights and invasion of human habitations. Extensive areas of babassu palm forests (Orbignia phalarata) are the habitat of triatomines such as R. pictipes, R. robustus and P. geniculatus. Constant burning and deforestation of these areas promotes dispersal of these vectors that may enter houses by flying (Barrett & Guerreiro 1991). Climatic modifications in the Amazon that involve a decrease in the amount of rain create dryer habitats such as those of central Brazil and favor the adaptation of triatomine species from these areas where Chagas disease is endemic. Ecosystem changes and modifications in the habitats of triatomines can lead to episodes such as those seen along the middle Rio Negro, municipality of Barcelos, State of Amazonas, with attacks of triatomines on cutters of piaçava palm fibers or as on Marajó Island in the mouth of the Amazon where triatomines have become associated with domestic animals and have invades human dwellings (Coura et al. 1994a, Valente et al. 1996). The ecological pressure of deforestation, with the destruction of the natural habitats of these vectors, may force these triatomines to change their behavior, as has already happened in several parts of tropical America, and may lead them to become adapted to human dwellings. The importance of sylvatic or secondary species in Chagas disease and the possibility of their adaptation to human habitations have been little studied and few data are available. At this time we have only isolated reports of sylvatic triatomines colonizing houses. These species that are candidates for vectors are: P. rufotuberculatus, found colonizing houses in Bolivia (Noireau et. al 1994), E. mucronatus seen in Peru and Bolivia (Torrico et al. 1946, Lent & Wygodzinski 1979, Valencia-Telleria 1990, Noireau et al. 1995, 1997), R. stali found in Cochabamba in Bolivia (Tibayrenc & Le Pont 1984) with various degrees of importance in the transmission of Chagas disease, and P. geniculatus, the most widely distributed species in South and Central America, especially in the Brazilian Amazon region (Valente et al. 1994). The importance of the accidental introduction of domesticated species of triatomines coming from areas endemic for Chagas disease should not be underestimated, especially for Triatoma infestans, a species now under control. This species that was introduced into Brazil at the beginning of this century needs to be well policed at the borders of the Amazon region, especially because it has already been reported for the state of Maranhão as well as the northern part of the state of Tocantins (Filho & Silveira 1979). Noireau et al. (1996) has referred to the geographical expansion of sylvatic foci of this species into areas of hot and humid climates such as those of the Amazon where it has yet to penetrate. This makes imperative a permanent entomological vigilance for this species, along the Trans-Amazon Highway, for example, where colonists live in precarious houses that could easily be colonized by this triatomine. Because of its tenacious nature, combating T. infestans in the region would entail great operational difficulties and high costs. The much needed implantation of an Epidemiological Vigilance Program for Chagas Disease in the Brazilian Amazon (Valente et al. 1995, Feitosa, 1995) should be seen as a measure that recognizes the region's priority for vigilance due to its geographical and human characteristics. In this manner, preventive actions should be undertaken and the region's ample potential for endemicity should be recognized. Those areas with relatively high serological prevalence (Coura et. al 1994b) should be mapped by means of an ample serological screening program. New serological studies for anti-T. cruzi antibodies should use more modern antigens, considering the past 20 years of human intervention in the region. Special strategies in vector control should be adopted to combat the possible domestication of triatomine vectors in the region. Financed with resources of National Healt Foundation: Center of Control of Transmitted Diseases for Vectors, of Chagas Disease, Brasília, and Instituto Evandro Chagas, Belém, Brazil. REFERENCES Barrett TV, Guerreiro JHG 1991. Os triatomíneos (Hemiptera, Reduviidae) em relação à doença de Chagas, p.119-130. In Bases Científicas para Estratégias de Preservação e Desenvolvimento da Amazônia: Fatos e Perspectivas, CNPq/INPA, Belém. Coura JR 1990. Chagas disease as endemic to the Brasilian Amazon: risk or hypotesis? Rev Soc Bras Med Trop 23: 67-70. Coura JR, Barrett TV, Naranjo MA 1994a. Ataque de populações humanas por triatomíneos silvestres no Amazonas: uma nova forma de transmissão da infecção chagásica? Rev Soc Bras Med Trop 27: 251-253. Coura JR, Junqueira ACV, Giordano CM, Funatsu IRK 1994b. Chagas'disease in the Brasilian Amazon, I - A short review. Rev Inst Med Trop São Paulo 36: 363-368. Crescente JA, Valente SAS, Valente VC, Araújo JEA 1992. Ocorrência de 4 novos casos agudos de doença de Chagas na Vila de Icoaraci-PA. Rev Soc Bras Med Trop 25 (Supl. I): 29. Deane LM 1964. Animal reservoirs of Trypanosoma cruzi. Rev Bras Mal Doen Trop 16: 27-48. Deane LM 1967. Tripanosomídeos de mamíferos da Região Amazônica IV. Hemoscopia e xenodiag-nóstico de animais silvestres da Estrada Belém-Brasília. Rev Inst Med Trop São Paulo 9:143-148. Deane MP, Lenzi HL, Jansen AM 1984. Trypanosoma cruzi: vertebrate and invertebrate cycles in the same mammal host, the opossum Didelphis marsupialis. Mem Inst Oswaldo Cruz 79: 513-515. Feitosa VR 1995. Implantação de um sistema de Vigilância Epidemiológica (VE) de doença de Chagas na Amazônia. Rev Soc Bras Med Trop 28 (Supl. III): 84-87. Filho JC, Silveira AC 1979. Distribuição da doença de Chagas no Brasil. Rev Bras Mal Doenças Trop 31: 85-98. Fraiha Neto H, Valente SAS, Valente VC, Pinto AYN 1995. Doença de Chagas - Endêmica na Amazônia? An Acad Med Pará 6: 53-57. Lainson R, Shaw JJ, Fraiha H, Miles MA, Draper CC 1979. Chagas disease in the Amazon Basin. I . Trypanosoma cruzi infections in silvatic mammals, triatomine bugs and man in the State of Pará, North Brazil. Trans R Soc Trop Med Hyg 73: 193-204. Lent H, Wygodzinski P 1979. Revision of the Triatominae (Hemiptera, Rediviidae) and their significance as vectors of Chagas disease. Bull Am Mus Nat Hist 163: 1-529. Lenzi HL 1984. The recent discovery of what might be a primordial escape mechanism for Trypanosoma cruzi. Mem Inst Oswaldo Cruz 79: 273-292. Miles MA, Souza AA de, Povoa M 1981. Chagas disease in the Amazon Basin. III. Ecotopes of ten triatomine bug species (Hemiptera, Reduviidae) from the vicinity of Belém, Pará State, Brazil. J Med Entomol 18: 266-278. Naiff RD, Barret TV, Arias JA 1987. Trypanosoma cruzi nas glândulas anais de Didelphis marsupialis: primeiro registro de infecções naturais, p. 234-235. X Congresso da Sociedade Brasileira de Parasito-logia, Salvador. Noireau F, Vargas F, Bosseno MF, Brenière SF 1994. Apparent trend to domesticity observed in Panstrongylus rufotuberculatus (Hemiptera: Reduviidae) in Bolivia. Res Rev Parasitol 54: 249-250. Noireau F, Bosseno MF, Carrasco R, Telleria J, Vargas F, Camacho C, Yaksic N, Brenière F 1995. Sylvatic triatomines (Hemiptera: Reduviidae) in Bolivia. Trends towards domesticity and possible infection with Trypanosoma cruzi (Kinetoplastida: Trypanosomatidae). J Med Entomol 32: 594-598. Noireau F, Brenière SF, Cardozo L, Bosseno MF, Vargas F, Peredo C, Medinacelli M 1996. Current spread of Triatoma infestans at the expense of Triatoma sordida in Bolivia. Mem Inst Oswaldo Cruz 91: 271-272. Noireau F, Brenière SF, Ordonez L, Cardozo L, Morochi W, Gutierrez T, Bosseno MF, Vargas F, Yaksic N, Dujardin JP, Peredo C, Wisnivesky-Colli C 1997. Low probability of transmission of Trypanosoma cruzi to humans by domiciliary Triatoma sordida in Bolivia. Trans R Soc Trop Med Hyg 91: 653-656. Rodrigues B de A, Melo G de B 1942. Contribuição ao estudo da Tripanosomíase Americana. Mem Inst Oswaldo Cruz 37: 77-90. Rodrigues IRC, Souza AAA, Terceros RO, Valente SAS 1988. Doença de Chagas na Amazônia: I. Registro de oito casos autóctones em Macapá. Rev Soc Bras Med Trop 21:193-197. Shaw JJ, Lainson R, Fraiha H 1969. Considerações sobre a epidemiologia dos primeiros casos autóctones de doença de Chagas registrados em Belém, Pará, Brasil. Rev Saúde Púb 3: 153-157. Souza AA, Pardal PPO, Valente SAS, Boulhosa CF, Lima JAN, Correa ZJC 1989. Doença de Chagas no Estado do Pará: aspectos clínicos e laboratoriais de 4 novos casos autóctones, p. 10. XI Congresso Brasileiro de Parasitologia, Rio de Janeiro. Tibayrenc M, Le Pont F 1984. Étude isoenzymatique d'isolats boliviens de Trypanosoma cruzi pratiques chez Rhodnius pictipes. Données préliminaires sur la transmission de la maladie de Chagas dans l'Alto Beni bolivien. Cah ORSTOM, série Entomol Med Parasitol 22: 55-57. Torrico RA 1946. Hallazgo de Eratyrus mucronatus, infestación natural de "vinchuca" de cerro e Eutriatoma sordida en Cochambamba. An Lab Central, Cochabamba 1: 19-23. Shikanai-Yasuda MA, Brisola Marcondes C, Guedes LA, Siqueira GS, Barone AA, Dias JCP, Amato Neto V, Tolezano JE, Peres BA, Arruda Jr ER, Lopes MH, Shiroma M, Chapadeiro E 1991. Possible oral transmission of acute Chagas disease in Brasil. Rev Inst Med Trop São Paulo 33: 351-357. Valencia Telleria A 1990. Investigación Epidemiológica Nacional de la Enfermedad de Chagas, Ministério de Prevención Social y Salud Pública, La Paz, 184 pp. Valente SAS, Valente VC 1993a. Situação atual da doença de Chagas na Amazônia. Rev Soc Bras Med Trop 26 (Supl.): 68-70. Valente SAS, Crescente JA, ValenteVC, Araújo JEA, Lima JAN 1993b. Observações sobre 5 casos agudos de doença de Chagas no Município de Afuá, Estado do Pará, 1992. Rev Soc Bras Med Trop 26 (Supl. I): 81. Valente SAS, Valente VC, Souza JM de, Pinto AYN, Lima JAN, Araújo JEA 1993c. Doença de Chagas na Amazônia: registro de óbito por transfusão sanguínea no Município de Altamira, Estado do Pará, p. 82. XXIX Congresso da Sociedade Brasileira de Medicina Tropical, Fortaleza. Valente SAS, Valente VC, Neves, AYP Lima, JAN Araújo JEA, Noireau F 1994. Aspectos epidemioló-gicos sobre a possível domiciliação do Panstrongylus geniculatus em Muaná, Estado do Pará. Rev Soc Bras Med Trop 27 (Supl. I): 113. Valente SAS, Valente VC, Feitosa VR 1995. Sobre a implantação de um sistema de vigilância ento-mológica e epidemiológica em doença de Chagas na Amazônia, p. 322. XIV Congresso Brasileiro de Parasitologia, Goiânia. Valente SAS, Valente VC, Pinto AYN, Crescente JAB 1996. Aspectos epidemiológicos dos reservatórios e vetores da infecção chagásica na Amazônia, p. 1501-1503. In R Veronesi, Tratado de Infectologia, Patologia Tropical da Amazônia, Atheneu, São Paulo. Valente SAS, Fraiha Neto H, Leão RNQ, Miles MA 1997a. Doença de Chagas, p. 597-610. In RNQ Leão, Doenças Infecciosas e Parasitárias: Enfoque Amazônico, CEJUP, Belém. Valente SAS, Valente VC, César MJB, Santos MP 1997b. Registro de 15 casos autóctones de doença de Chagas no Estado do Amapá com evidências de transmissão oral, p. 53. XXXIII Congresso da Sociedade Brasileira de Medicina Tropical, Belo Horizonte. Copyright 1999 Fundacao Oswaldo Cruz - Fiocruz The following images related to this document are available:Photo images[oc99208a.jpg] |
| |||||||||

{kind=link}