 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
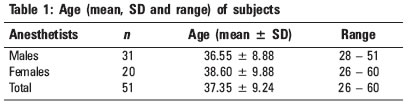
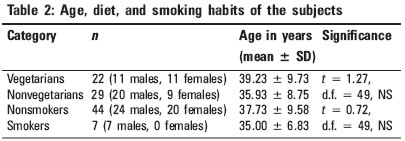
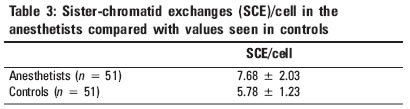
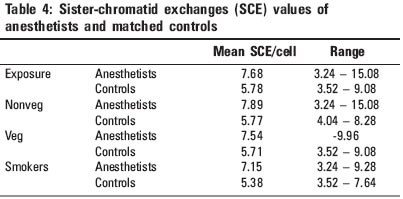
Indian Journal of Occupational and Environmental Medicine, Vol. 9, No. 2, May-August, 2005, pp. 86-89 Original Article Sister-chromatid exchanges in anesthetists Jayakaran F, Thomas IM Department of Anatomy, St. John's Medical College, Bangalore, India Code Number: oe05020 Abstract A number of reports indicate that waste anesthetic gases (AG) that are ambient in the operation theater (OT) are responsible for producing effects in anesthetists like headaches, dizziness, nausea, heart and liver diseases, cancer as well as poor obstetric history for the female staff. To evaluate the presence or absence of genotoxicity. Because sister-chromatid exchanges (SCE) are sensitive indicators of exposure to mutagens, the blood of 51 anesthetists and 51 stringently matched controls were cultured and harvested and analyzed. (1) Descriptive statistics - mean, range and standard deviation. (2) Inferential statistical procedures: (a) univariate procedures and (b) multivariate procedures (step-wise multiple regression analysis). The results showed a significantly higher level of SCE (7.68 ± 2.03/cell) in anesthetists when compared to that of controls (5.78 ± 1.23/cell), demonstrating that a genotoxic effect is present. There is a strong case for installing scavenging devices and leak-proof apparatus in the OT to lower the level of ambient AG, because the health of all OT staff is at risk. Keywords: Anesthetic gases, Anesthetists, Genotoxicity, Sister-chromatid exchanges Introduction Several surveys have been conducted in Europe and in the USA to establish whether anesthetic gases (AG) may be held responsible for various symptoms suffered by anesthetists after a period spent in the operation theater (OT). These adverse reactions include headaches, nausea, dizziness, nervousness, increased cancer rate, hepatic and renal diseases, as well as infertility, and fetal loss.[1] The villain here is believed to be the presence of low-ambient levels of waste AG, which have accumulated in the OT over a period of time in the absence of effective scavenging systems and efficient leak-proof ventilators. The aim of the present work is to evaluate the presence or absence of chromosomal effects in anesthetists as a consequence of this chronic exposure to halothane and nitrous oxide and occasionally to ether and trilene. The parameter chosen is sister-chromatid exchanges (SCE), which is a sensitive indicator of genotoxicity.[2],[3] Elevated SCE levels indicate exposure to genotoxic agents.[4],[5] In principle, SCE can be seen in any cell that has replicated twice in the presence of 5-bromo-deoxy-uridine (BrdU).[6] It is known that SCE represent the interchange of DNA replication products, which maintain their polarity,[7],[8] at homologous loci. The precise molecular mechanism is not known. Materials and Methods The project proposal had been submitted to the Ethical Committee and clearance had been obtained before the commencement of the work. The collection of data was done over a period of 2 years. Fifty-one healthy Indian anesthetists (31 male and 20 female) in active service were selected for this study. They had a minimum of at least 2 years as an anesthetist. They were matched 1 : 1 with healthy Indian physicians (controls) of the same age (± 1 year), sex, diet, smoking habits, and lifestyle. Four milliliters of blood was collected from each subject and control in heparinized disposable syringes and cultured according to the technique of Arakaki and Sparkes[9] with minor modifications. About 5 mg/ml of BrdU (Sigma Chemicals Co. Inc, USA) was added to the culture vials at the time of setting up culture before incubation, which was maintained for 72 h. All subjects and controls had filled up and signed the informed consent form. All procedures were made under sterile conditions. After harvesting, the slides were stained by the FPG method of Perry and Wolff[10] for differential staining of sister chromatids. Twenty-five metaphases (with 46 chromosomes each) of each subject and control were scored for SCE. The results obtained were subjected to statistical evaluation. Statistical analysis Results [Table - 3] shows the mean SCE/cell in anesthetists and controls. Age, as is to be expected, was significantly and positively correlated with the years of exposure to anesthesia (r = 0.29, d.f. = 49, P < 0.001). Univariate procedures were used to establish the influence of different dependant variables (age, sex, diet, and smoking habits) on SCE levels of anesthetists, but they did not significantly predict the number of SCE. Because subjects and anesthetists were stringently matched for dependant variables such as age, sex, smoking, diet, and lifestyle, univariate procedures were used here. Multivariate examination (step-wise multiple regression analysis) was also done. The regression equation explained 23.84% of the variance in the total number of SCE (F = 32.61, d.f. = 1,100, P < 0.001). The significant increase in SCE was not related to the years of exposure to AGs. Just being an anesthetist was associated with a higher number of SCE. [Table - 4] shows the mean SCE/cell of the various groups examined among anesthetists and controls. Discussion Although inhalation anesthetics have been suspected of genotoxicity, the amount of evidence obtained from the few cytogenetic studies on humans are limited and conflicting. The limiting factors for a conclusive study are the difficulties in establishing the degree of occupational exposure and the confounding variables like age, sex, diet, and smoking habits to name a few. The anesthetists chosen for this study worked in OT, where there were no scavenging devices. Circulation was effected more usually by air conditioners or less frequently by pedestal fans. Only anesthetists have been chosen as subjects for this work, because they have the most exposure to waste gases emanating from the apparatus. If ventilators are not used, the level of AGs in the OT is 76% higher near the apparatus than elsewhere.[11] Anesthetic assistants and nurses have an exposure one-third or one-fourth that of an anesthetist. Previous reports of SCE studies were made using a mixed sample of anesthetists, nurses, and technicians. Husum and Wulf,[12] Holmberg et al,[13] Lamberti et al,[14] and Bozkurt et al[15] found no significant increase in the number of SCE in a mixed sample of exposed OT personnel. Later, workers like Sardas et al[16] of Turkey and Karelova et al.[17] of former Czechoslovakia and Bilban et al.[18] found diametrically opposite results. They reported a significant increase in SCE in exposed subjects. Natarajan and Santhiya[19] from India found a doubling in the mean SCE by 20% of the exposed subjects. Anesthetists of the present study too showed a significant increase in the number of SCE compared to 1 : 1 matched controls. As all blood samples for the culture were collected from the anesthetists immediately after their operation schedule, it is tempting to assume that the very short period between exposure (damage induction) and culture (DNA replication) is responsible for the number of lesions which have remained unrepaired and which exhibit as SCE.[20] It has been noticed that the SCE levels recorded by the various workers did not show any coincidence. Comparison of results between various studies is difficult because there are differences in the level and duration of exposure to anesthesia in the different hospitals in different countries, as well as differences in the scoring by different individuals. That the results from Denmark, Sweden, and Italy show no significant difference in SCE levels between anesthetists and controls, while reports from Turkey, former Czechoslovakia and India show significantly higher SCE levels for anesthetists, may be a reflection of the use of sophisticated, leak-proof apparatus, efficient scavenging and/or fewer hours of exposure to anesthesia per day in the former group of countries. The anesthetists from the latter group of countries may be overworked in under-staffed, nonscavenged OT, and consequently have more exposure to the waste AGs. Further work on anesthetists working in well-scavenged OT may provide additional answers to the genotoxic effects of AG. Only anesthetists had been chosen as subjects for this work, as they have the most exposure to waste gases emanating from the apparatus. Earlier, workers like Husum and Wulf,[12] Holmberg et al,[13] Lamberti et al[14] and Bozkurt et al[15] found no significant increase in the number of SCE in a mixed sample of exposed OT personnel, which included nurses, as well as technicians. Anesthetic assistants and nurses have an exposure one-third or one-fourth that of an anesthetist. If ventilators are not used, the level of AGs in the OT is 76% higher near the apparatus than elsewhere.[11] Later workers like Sardas et al,[16] Karelova et al,[17] and Bilban et al,[18] found diametrically opposite results. They reported a significant increase in SCE in exposed subjects. Natarajan and Santhiya[19] found a doubling in the mean SCE on 20% of the exposed subjects. Anesthetists in the present study too, showed a significant increase in the number of SCE compared to 1 : 1 matched controls. Conclusion The present study therefore shows that exposure to AG leads to a statistically significant increase in SCE in anesthetists compared to stringently matched controls. This long-term exposure to low levels of ambient AGs has a genotoxic effect, as increased SCE are indicators of exposure to genotoxins, with possible deleterious consequences for the health of the OT personnel and their offspring. This is the second Indian study in Indian conditions in recent times showing similar results and it requires immediate installation of scavenging devices in the OT. It is strongly recommended that steps be taken to reduce the exposure and eliminate the genotoxin from the environment. It is strongly emphasized that it is imperative to the health of the anesthetist and other OT staff, to reduce the level of ambient AG in the OT by the use of leak-proof ventilators and efficient scavenging devices. It may not be out of place either to suggest that all OT personnel wear sampling devices on their caps or around their necks, so that it may be possible to monitor the exposure.Acknowledgments Dr. Chittaranjan Andrade, Professor of Psychopharmacology, National Institute of Mental Health and Neuro Sciences (NIMHANS), Bangalore is thanked immensely for the statistical analysis of the data in this paper. References
Copyright 2005 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe05020t4.jpg] [oe05020t3.jpg] [oe05020t2.jpg] [oe05020t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}