 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
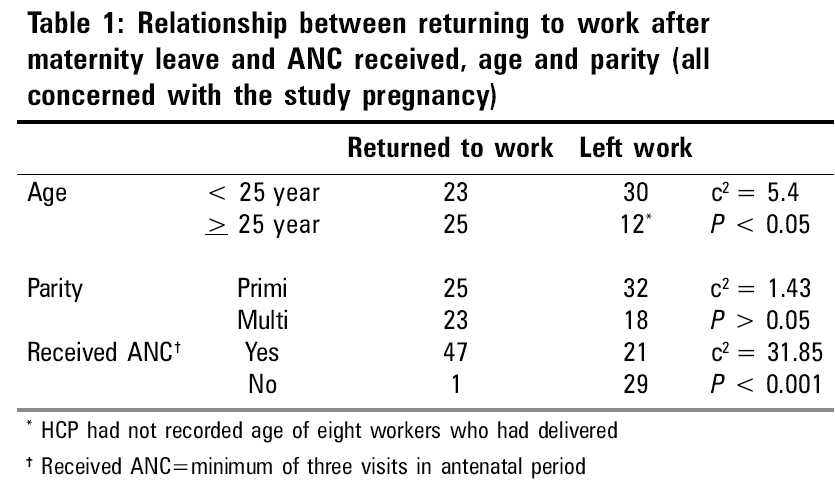
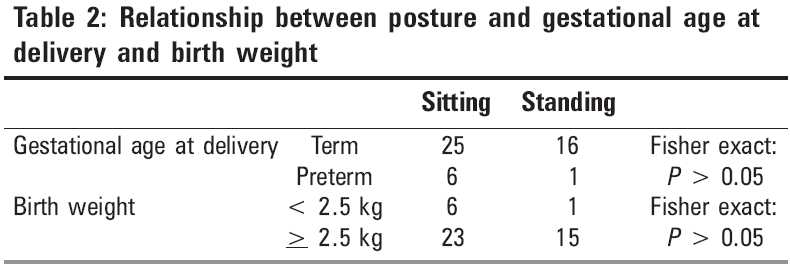
Indian Journal of Occupational and Environmental Medicine, Vol. 9, No. 3, September-December, 2005, pp. 107-110 Original Article Utilization of antenatal services in apparel manufacturing factories in Bangalore Joseph B, Charles S, Clement Prakash TJ, Vikas Sudan ML, Jasmine G Department of Community Health, St. John's Medical College, Bangalore, Karnataka, India Code Number: oe05024 Abstract The apparel manufacturing industry in Karnataka has assumed gigantic proportions. A large majority of the workers in this industry are women in the reproductive age group. Some companies have recognized this situation and are taking proactive steps in providing a range of services to the women employees. The objective of this study was to identify the outcomes of the services that are provided to the pregnant women in seven factories belonging to one such company. The study attempted to contact all registered pregnant women who had returned to work, in an attempt to identify the positive features and lacunae in the services that were provided. The results showed that half the workers who had been provided services in the antenatal period had not returned to work. A majority of the workers had availed of adequate antenatal care and most of them had delivered in the local Employees State Insurance (ESI) Hospital. Knowledge of antenatal care was generally good and most information had been received from the Health Care Providers (HCPs). The positive role of the HCPs in these factories has to be recognized and they should be provided with adequate support and training to perform their functions optimally.Keywords: Antenatal services, Apparel manufacturing industry, Outcome, Pregnancy Introduction The garment industry in the State of Karnataka, in South India, is considerably well-organized and is the employer of the largest number of women workers after, perhaps the beedi industry. Officially there are nearly 800 garment manufacturing units in Karnataka out of which more than 90% are in Bangalore. The total number of workers statewide is 1 53 978 out of whom 1 46 835 are working in Bangalore units. The number of women workers statewide in the industry is 1 10 019 out which 1 03 039 are in Bangalore (statistics from Department of Labour, Government of Karnataka, 2002). The factories (units) mentioned above fall within the purview of the various laws that have been enacted in our country. The Department of Community Health has been providing a variety of services to the garment manufacturing industry over the past 5 years. The following study is based on the services provided by the Department to one of Bangalore′s largest apparel export houses which has under it′s flagship a number of factories employing about 10 000 workers in all. Briefly the services provided to this industry included the training of Health Care Providers (HCPs) (nurses) and doctors employed by the company, instituting a health information system, providing input on general environmental conditions within the factory and invariably providing an annual medical check for the workers of individual factories belonging to the company. During the recent past the Department has conducted annual periodic medical examinations for 3858 workers of the company. Of these 3287 (85.2%) were female workers and of these 3235 (98.42%) were women who were in the reproductive age group of 15-44 years. Given the large numbers involved the provision of antenatal services by the nurses and doctors was part of the interventions provided by the company. At the end of a year of providing these services, the company wanted to identify the successes and failures of this programme. This descriptive study was an attempt to evaluate the outcome of interventions targeting the pregnant women working in the company. Materials and Methods As part of this study, the HCPs in each of the factories were asked to identify and separate out the health records of antenatal women that is part of the health information system in the company. A schedule of questions was developed and where possible a personal interview was conducted with the women who had returned to work after delivery. All women who had returned to work in the factory after delivery were interviewed - on occasions this required multiple visits to the factory. In case a beneficiary of the antenatal services had left the job, her antenatal card was perused to elicit relevant data. The schedule of questions attempted to identify aspects related to knowledge about maternal health (common practices, complications that could occur, contraception, etc.) outcome of the pregnancy and their working conditions in the factory. The results obtained were tabulated and analysed using simple statistical packages. Results As per the information provided by the factory nurses there were a total of 103 pregnancies recorded in the health information system during the period starting 1st January 2003 to 31st December 2003. The study was undertaken in the months of March-April 2004. Of the 103, we were able to contact 51 women - those who returned to work in the same factory after the completion of their maternity leave. Key informant interviews conducted with the nurse and few workers revealed that most of them stayed back at home to take care of their newborns. Further analysis of this phenomenon [Table - 1] revealed that a significant number of workers who had discontinued work following delivery were under 25 years of age. In comparison those who were more than 25 years of age were more likely to resume work in the factory after their maternity leave. Although only 44% of those who had two children or more had quit the job in comparison to 64% of those who had delivered their first child, the difference was not statistically significant. It was also noted that a significant number of workers who had received adequate antenatal care from the HCP returned to work after their maternity leave when compared to those who had not accessed any or adequate antenatal care from the HCP [Table - 1]. To briefly describe the demographic details of the women interviewed - the ages of the women ranged from 20 to 31 years with the mean age being 24.7 years. The age at marriage ranged from 15 to 30 years with the mean age at marriage being 19.9 years. Of the 51 women, 34 (66.6%) had studied up to 10th Standard and above. For 24 women the studied pregnancy was their first pregnancy. Of the 51 registered women who were interviewed, two had medical terminations of pregnancy because of problems detected during the ante-natal period and one woman had a spontaneous abortion. The analysis that follows pertains to the details provided by the 48 women who had delivered and returned to work after their maternity leave. All the women spent a minimum of 8 h at work. Most of the women were employed as tailors (25 out 48-52.1%), the others were employed as helpers or in ironing, checking or any of the other processes in the manufacture of apparel. Of these 48 pregnancies, five delivered of their babies by caesarean section. The indications for caesarean sections were breech presentation (two cases); with one case each of cephalo-pelvic disproportion, decreased foetal movements and previous caesarean section accounting for the remaining five. One of the pregnancies resulted in delivery of twins. Ten out the 48 women (20.8%) did not take even a minimum of 100 tablets of iron and folic acid. The precise reasons for this were not forthcoming - most women did not have a logical reason for discontinuing the prophylactic. On the other hand all the women had taken the required dosage of Tetanus Toxoid (TT). Among 48 women who delivered, 34 (70.83%) had utilized the services of the Employees State Insurance (ESI) Hospital, 11 (22.9%) had utilized a private hospital, while two (4.2%) delivered in a Government Hospital and only one had a home delivery. Seven of the deliveries (14.6%) had occurred preterm, one woman delivered postterm and the remaining were all term deliveries. The analysis of the data obtained from our small study did not show any significant difference in the gestational age or birth weight of the babies at delivery between those working in standing posture and others [Table - 2]. Details were available for 46 of the 49 children born. The mean birth weight of the children is 2.71 kg. Only seven children (14.58%) were born with low-birth weight (weighing less than 2.5 kg). Mean birth weight of study pregnancies is 2.74 kg as compared to 2.7 kg, which is the mean birth weight in Karnataka.[1] On questioning the women about the special foods that need to be taken during pregnancy, 36 of them (75%) were able to mention at least one special food such as green leafy vegetables, fruits, milk and others - most of them mentioning two items and above. Forty-five women (93.7%) were able to mention at least one method of contraception, once again with a large number mentioning two or more methods. In most cases (70.33%) the source for the information was found to be the HCP (nurse) who was posted in the factory. However, many women (31 out of 48-64.6%) were unable to list even one complication that was likely to take place during pregnancy. Discussion In the factories that we studied it was seen that nearly 50% of the pregnant women discontinued working after their delivery. This fact underlines the importance providing information and education regarding the postnatal period as and when the women arrive for the antenatal services. If this practice is not followed we will be losing a good opportunity to provide women about knowledge about their impending delivery and the events thereafter. The content of this education could include aspects related to breastfeeding, immunization and care in illness among other topics. From the data available it appears that younger women, who probably have only one child, are more likely to leave their jobs. This is probably because they are more anxious and concerned this being their first pregnancy. Further studies should identify the precise reasons for this phenomenon. If our postulation is true, then emphasis has to be placed on the availability and the utility of the factory crθches and the workers should be encouraged to take advantage of these facilities. This finding also has an important bearing on the maternity leave available to workers in India. As per the Maternity Benefit Act,[2] only 84 days (12 weeks) of leave are eligible for pregnant women in our country. This compares poorly with most other countries of the world, especially those in Europe.[3] It is possible that many workers have resigned from work after delivery because of this short duration of maternity leave. The utilization of antenatal services was very high in the group surveyed. All the women had benefited from at least one antenatal visit as evidenced from the 100% coverage for TT immunization as against data produced by the National Family Health Survey 2[4] (NFHS2) from Karnataka, which shows that 81.4% of the women had received TT in the state. However, the compliance with regard to iron and folic acid was relatively poor - the reasons for this were not easily forthcoming though intolerance to the medication was mentioned as a common problem in the key informant interviews. While the immediate benefits of regular and adequate ante-natal care visits are evident, it must be noted that benefits also accrue to the worker in terms of postnatal care. Data for Karnataka (NFHS2) indicates that 86.7% were provided with adequate ante-natal care. Once again in Karnataka,[4] only 27.8% of the women had delivered in a government setting. This appears to indicate that at least women who were employed in the organized sector availed of services provided by a governmental agency; no doubt they had contributed a significant part of their income for the services. Our finding that the utilization of the ESI Hospital was high was probably due to the fact that the services here are free of cost and because they would get all maternity benefits more easily if they delivered here. The high cost of having a delivery in a private hospital may have also played a role in this phenomenon. Meta-analysis of literature has shown that women doing physically demanding working, especially those working in standing posture and shift or night work delivered prematurely more often.[5] Adverse maternal working conditions also have a role to play in low birth weight of children.[6],[7] Once again the numbers in our study are too small to comment critically on the situation in the garment industry. While most women appeared to have a fair amount of knowledge regarding diet during pregnancy and contraception after delivery, the knowledge with regard to complications that can occur during pregnancy was poor. Most women had received information on different aspects of pregnancy from the HCP. This shows the importance of having such a cadre of workers in factories that are dominated by women in the work force. The role of Occupational Health Nurses in promoting optimal preconceptual and pregnancy health practices, using community resources and maintaining current knowledge about high-risk pregnancy prevention and care has been elaborated in some studies.[8] Our finding that they had not concentrated adequately on aspects related to complications during pregnancy, indicates that the content of the communications from the HCP to the workers has to be monitored and any lacunae or areas that were missed out had to be reinforced in subsequent trainings. Conclusion With a large number of women in the reproductive age group being employed in the garment manufacturing units in Bangalore and other parts of the country, it is imperative that a workplace-based intervention for antenatal women is instituted in these factories. The large attrition rate of workers in these factories, inclusive of women who have recently been pregnant, calls for focused interventions in the form of prophylactics and health education for these workers. It is heartening to know that a majority of the workers in Bangalore utilize the services of the ESI Scheme for their intra-natal care. While our limited data shows no association between posture at work and the outcomes of pregnancy, further studies will have to be conducted in this area, especially in light of the fact that many studies from abroad appear to indicate a negative outcome. In the setting where the study was conducted, the role of the HCP in the antenatal services has to be appreciated, although the quality and content of their health promotion activities has to be improved.References
Copyright 2005 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe05024t1.jpg] [oe05024t2.jpg] |
| |||||||||

{kind=link}
{kind=link}