 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Occupational and Environmental Medicine, Vol. 9, No. 3, September-December, 2005, pp. 115-117 Original Article Assessment of health profile of daily wage labourers Gurav RB, Kartikeyan S, Wayal R, Joshi SD Department of Preventive and Social Medicine, Rajiv
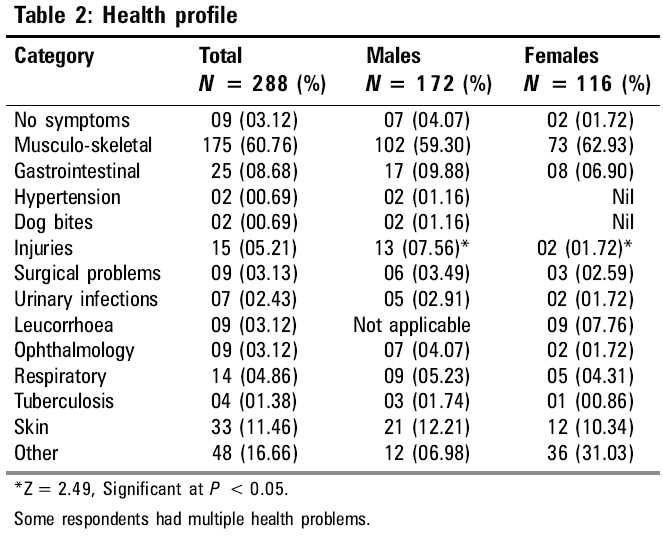
Gandhi Medical College, Thane, Maharashtra, India Code Number: oe05026 Abstract A cross-sectional study conducted in Thane district (Maharashtra) on 172 males and 116 females daily wage labourers revealed that none of them had access to occupational health services or any type of social security. Nearly one-third of the participants were 26-40 years old. The average number of health problems per participant was 1.22. Nearly two-thirds of the workers had musculo-skeletal problems, while 11.46% had various dermatological problems. These labourers were working in diverse environments and the nature of their jobs was always changing. Hence, it was not possible to pin point the causes of their health problems.Keywords: Daily wage workers, Health problems, Migrant workers, Unorganized sector Introduction In the past, the nature of work undertaken by daily wage labourers in the unorganized sectors of the economy was based on caste and tradition. Nowadays, daily wage labourers are forced to take up any type of job due to the forces of socio-economic development, population growth, employment-related migration and decrease in job opportunities. In many urban areas, groups of daily wage labourers wait at market places, road junctions and outside railway stations in order to be hired for any type of semi-skilled or unskilled work. In Mumbai and adjoining cities, these workers who belong to the unorganized sector and accept any type of chore like carrying loads, painting, plumbing, assisting in building construction, working on farms and cleaning. Their daily wages are paid at the end of the day or after completing the assigned task. The duration of the task depends on the type of work. Those workers who do not get hired return to their homes or their place of rest. The next day, they again queue up, waiting to be hired. Since these labourers are engaged in several types of tasks, they are exposed to multiple physical, chemical and biological agents, which make them vulnerable to various health problems that include - injuries, respiratory problems, dermatitis, musculo-skeletal disorders and gastro-intestinal diseases. The nature of work, hours of work, low pay, poor housing and separation from family, lack of job security and lack of access to occupational health services cause anxiety in the minds of the workers.[1] These factors affect the health of the workers, as also their efficiency and work productivity. The purpose of this study was to determine the socio-demographic and health profile of these daily wage labourers. Materials and methods This cross-sectional one-time prevalence study was conducted at Shivaji Chowk Naka, in Kalyan (Maharashtra), which is a waiting place for daily wage workers. Volunteers from a nongovernmental organization and local social workers explained the purpose of the study to prospective participants and helped in selecting an appropriate place for interviewing and clinically examining the workers. The interviews and clinical examinations were conducted between 8 a.m. and 10 a.m. so that their daily income was not affected. A pretested formatted proforma was used to record information. The personal particulars included age, sex education, marital status, religion, place of residence and personal habits/addictions. A participant who was staying in the study area for < 5 years was considered to be a ′migrant′. A person using any tobacco product on a daily basis for more than 1 year was determined to be a tobacco user. A daily intake of > 75 g of alcohol for > 2 years was labeled as ′heavy alcohol consumption.[2] The respondents were also queried about their current health problems, which were recorded on the proforma. Each subject was examined clinically. The blood pressure was recorded using a mercury sphygmomanometer. The procedure for recording systolic and diastolic blood pressure and the diagnostic criteria for diagnosis of hypertension were as per recommendations of the World Health Organization.[3],[4] The respondents with health problems were prescribed medicines, which were dispensed with the help of volunteers. Those requiring further investigations and/or specialized treatment were referred to municipal tertiary health care hospitals in the vicinity. The data were analyzed and presented. Results Demographics Only 12.50% of the respondents had no addictions. All the others were habitual consumers of tobacco products and/or alcohol and the differences in the distribution between males and females were not statistically significant. About 42.71% workers (all males) were heavy consumers of alcohol [Table - 1]. About 62.15% were natives of Maharashtra state, while 48 (16.67%) were from Andhra Pradesh, 25 (8.68%) were from Rajasthan and the rest were migrants from other states [Table - 1]. Nineteen male workers were staying at Shivaji Chowk Naka itself. Health problems Fifteen respondents (5.21%) reported injuries of various types. The sex difference in the distribution of injuries was statistically significant at P < 0.05 [Table - 2]. A majority of these daily wageworkers were hired by the construction industry, which is particularly known for a high incidence of accidents.[1],[6] More than 90% of these accidents are preventable.[1] According to Ramsay[7], the risk of accidents increases with extremes of temperature. Age, sex, personal habits (like working under influence of alcohol), personality traits (risk-taking behavior) and physical and mental state of the worker play an important role in the occurrence of accidents.[1] Fourteen respondents (4.86%), who were periodically working in the construction industry, reported diverse types of respiratory complaints. Inhalation of cement dust can cause respiratory disorders (like silicosis) and difficulty in breathing.[6] Exposure to silica also occurs during activities like sand blasting, polishing, grinding, stone cutting, dry wall finishing[8] [Table - 2]. Nine (3.12%) were suffering from ophthalmic problems, which included one male with traumatic cataract. The incidence of ocular injuries has reportedly escalated due to growth in jobs like stone crushing. Cement is known to cause ophthalmic problems by direct eye contact[6] [Table - 2]. Twenty-five (8.68%) respondents complained of gastro-intestinal problems such as abdominal pains, constipation and haemorrhoids. Workers may be exposed to chemicals, infective or parasitic agents at the place of work.[1],[6] Toxic substances like lead, arsenic, chromium, cadmium and phosphorus may be ingested with water and food by these workers and symptoms of poisoning may manifest many years later [Table - 2]. Thirty-three (11.46%) had several types of skin problems like eczematous dermatitis [Table - 2]. Direct contact with wet quick-setting cement can cause thermal injuries (called ′cement burns′) and dermatitis.[5],[6] Contact with cement and lime may lead to irritant dermatitis. The presence of chromate and cobalt in cement is known to cause allergic contact dermatitis.[9] Scarcity of water, limited availability of cleaning facilities and climatic conditions hasten the development of dermatitis in construction workers.[9] Cement workers and their supervisors ought to be informed about the health hazards posed by this widely used construction material through information, education and communication (IEC) activities. They need to be trained in safe working practices in order to minimize the risk.[5] Since the participants in the present study belonged to the unorganized sector, none of them had access to employer-provided health care services or any type of social security. It was not possible to pin point the causes of their health problems due to the ever-changing nature of their jobs. A healthy occupational environment is beneficial to worker′s health and is also conducive to higher work productivity.[1] Similar studies on different categories of workers in unorganized sector would help in devising interventional strategies. Acknowledgment The authors thank Shri. P. S. Mokashi, Chairman, Janhit Vaidyakiya ani Samajik Sanstha , Kongaon, Taluka Bhiwandi, Dist. Thane (Maharashtra), who helped in conducting this study.References
Copyright 2005 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe05026t1.jpg] [oe05026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}