 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
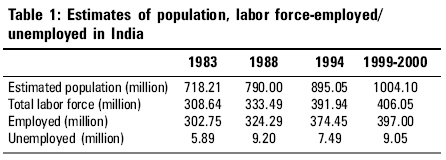
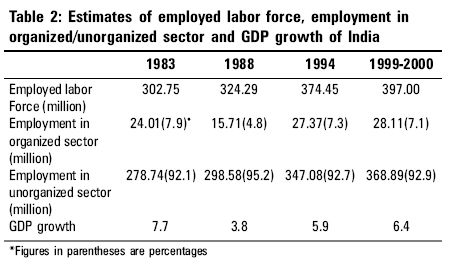
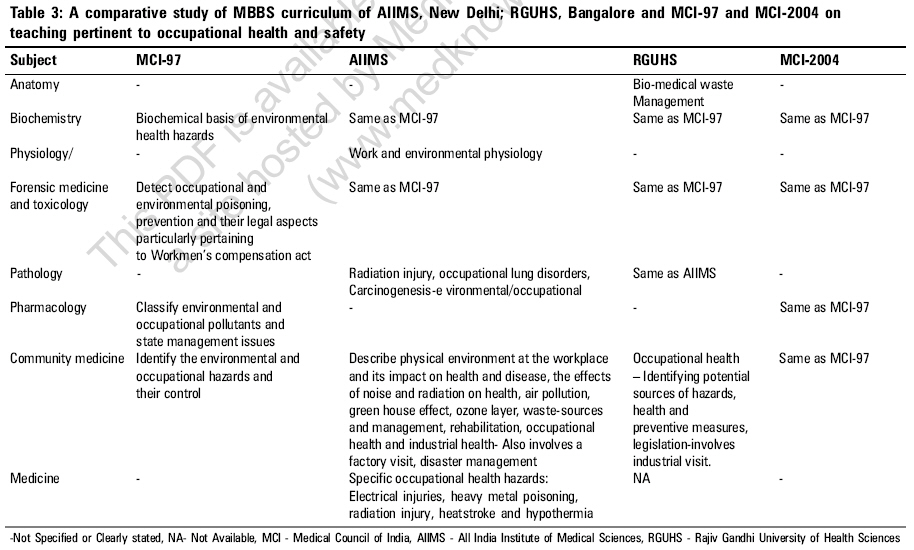
Indian Journal of Occupational and Environmental Medicine, Vol. 10, No. 3, September-December, 2006, pp. 97-101 Review Article Occupational health and safety: Role of academic institutions Jaiswal Abhishek, Patro BinodK, Pandav ChandrakantS Center for Community Medicine, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029 Code Number: oe06024 Abstract The occupational disease burden is growing at an unprecedented rate. The profile of occupational diseases has also changed over the period of time as a result of modernization, market liberalization and globalization which now encompasses minor allergy and injuries, systemic infections and diseases as well as the life-threatening leukemia and cancers. Trained human resources in the field of occupational health and safety are far below the requirement. Training in the area of occupational health and industrial medicine is not keeping pace with the changing industrial growth and technologies. There is an urgent need for strengthening skills, developing newer competencies and broadening our knowledge in occupational health and safety and disaster management. Traditional training in occupational health, needs to be supplemented with techniques of environmental epidemiology, environmental impact assessment and environmental risk assessment. The academic community should take the first step in demonstrating its leadership to address the long neglected concerns of occupational health and safety. Keywords: Academic institutions and India, industrial medicine, occupational health, training Introduction In India, the total work force in industries was six million in 1986. Now, due to tremendous mushrooming of industries, the workforce has increased to the current count of 62 million. Today, the workforce of the South Asian region (Bangladesh, India, Nepal, Pakistan and Sri Lanka) represents more than 20 per cent of the world′s working population.[1] The massive development of industries in this region can be contributed to various factors. Various economic institutions like the World Bank, the International Monetary Fund, the Asian Development Bank have influenced the countries to shed protectionist economics and stimulated them to compete for exports. Liberalization has opened their markets to global investors, who import both obsolete and hazardous industries as well as new technology. The ministry of labor and employment, government of India is the nodal agency for employment and labor-related statistics. The active workforce comprises approximately 440 million working population in India. Agriculture including forestry and fishing is the major sector providing employment to 58% of the workforce, which contributes significantly to the national economy. Service sector comprising community, social and personal activities, electricity, gas and water supply, transport, storage and communication, wholesale and retail trade, financing, insurance, real estate and business service community, contributes to 22% of the total workforce. Industrial sector comprising mining and quarrying, construction, repair and demolition, commerce and manufacturing contributes to 14% of the total workforce. Remaining six per cent of the workforce is engaged in a category which is not a defined one (informal sector).[2] Population Labor Force and Employment Estimates of population, total labor force-employed/ unemployed in India over a period (1983-2000)[3] are described in [Table - 1]. Estimates of employed labor force, employment in organized/ unorganized sector and GDP growth of India over a period (1983-2000)[3] are given in [Table - 2]. This industrial revolution is an amalgam of bliss and concern. Where this has helped in attenuating the growing unemployment, it, also, has brought growing health and safety concern for the workforce. Unlike developed countries, where the industrial development has also taken care of these growing concerns, developing countries are still getting strangled by these ever-increasing problems and insecurities. Specially, when growth has taken place concurrently in the agriculture, service, industries and information technology sectors within a short span of time. Complexity of Occupational Health and Safety Indian occupational health is more complex than being a mere health issue. This includes child labor; poor industrial legislation and a vast informal sector. In addition, it has also received less attention to occupational hygiene and surveillance. Much had been talked about this concern. But, unfortunately least has been done. This slanted industrial growth has some characteristics which are mentioned below: Focus on production: Industrialization in India primarily focuses on production. Health and safety have a very low priority. Except a few major, reputed, public and private industries, other industrialists are not sensitized about the importance of occupational health and safety. Exploitation of workforce: Abundant, low-skilled workforce and high rate of unemployment makes them vulnerable to exploitation. Getting work and a livelihood is more important; as a result hazards involved are ignored. Largely due to poverty, workers continue to work even when sick or injured. Illiteracy, poverty, ignorance and subconscious fear of losing the job (probably being the only earning member of the family) are some of the major factors that prevent the workforce from the required awareness for occupational health and safety measures. Hazardous industries: Global investors import both obsolete and hazardous industries as well as new technology. Traditional labor-oriented markets are changing towards automation and mechanization. However, at the same time, general awareness about occupational health and safety is not being spread to the society. Within this milieu, the workers have to join low resource settings including health and safety considerations. This has made them more susceptible to the hazards of technology than their counterparts in developed countries. After the information on gas leak in Bhopal in 1984 from the Union Carbide plant, the works manager said, "The gas just can't be from my plant. The plant is shut down. Our technology can′t go wrong. We just can′t have such leaks." Child labor: India cannot hide her face when it comes to child labor, perhaps, one of the most heinous practices against humanity. An estimated 70 to115 million children, under 14 years, are part of the Indian workforce. Child labor in the agriculture sector accounts for 80% of child labor in India and 70% of working children globally. In, Sivakasi, an estimated 1,25,000 children make the child labor force, comprising 30% of the entire labor force.[4] Impelled commercial sex work in this age group has been on the rise at an alarming pace and at the same time so have the associated risk of sexually transmitted diseases including drug abuse. Unorganized workforce: Workforce is denied the rights of association, as the zones are rarely accessible to trade unions. Only 8.8 per cent of the workforce in India is organized. The existing trade unions are mostly weak, politician-driven, ignorant and reluctant to organize on occupational health and safety. Enforcement and legislation: Although, there is a constitutional provision for occupational health and safety, securing equitable and humane conditions of work, maternity relief and against child labor as cited in article 24, article 39 (e and f) and article 42, the major problem is poor enactment is lack of awareness and poor enforcement of the law. Role of government: It appears that the government does not give high priority to the potential occupational hazards and hence lacks commitment towards the condition. For instance, a less-damaging incident than Bhopal gas tragedy occurred in 1982. However, despite the warning that should have given the company, Mr. T. S. Viyogi, the then labor minister said, "A sum of Rs. 25 crore has been invested in this unit. The factory is not a small stone, which can be shifted elsewhere. There is no danger to Bhopal, nor will there ever be." Although, much effort has been made by the government since then, it still needs to prioritize for thrust in this direction. Under the supervision of Inspector General of India, a small number of 300 Factory Inspectors are responsible to check the industrial safety in this vast country, compared to 3000 factory Inspectors in a much smaller country like Japan. Lack of trained medical professional: "As soon as it was confirmed that the gas was from the Union Carbide plant, the chief medical officer denied the gas was fatal; instead he described it as a minor irritant." In India, there are very few trained doctors in occupational health. Only a few medical professionals are able to diagnose occupational diseases. Silicosis and Bysinossis are often diagnosed as tuberculosis. Burden of Occupational Disease Occupational health does not deals with work-related diseases only but also encompasses all other factors that affect community health within it. The true burden of occupation diseases is largely unknown. There are certain hindrances: Poor surveillance: It has been a major impediment in assessing the true disease burden in the country. This has been also attributed for increased prevalence of occupational diseases and accidents. Under-reporting: The factories act requires notification of occupational diseases to the government, but they are hardly ever reported, allowing official statistics to compare well with developed countries. The official figures in 1994 showed 23 injuries per 1,000 factory workers. This compares with 4 per 1,000 in Japan during 1992; and 10 per 1,000 in Singapore.[5] Again, the factory act does not cover the vast majority of workers who work in the informal sector where accidents are not reported at all. This further invalidates government statistics. Lack of epidemiological evidences: In India, there is a huge gap in the epidemiological evidence from different industry-specific, exposure-specific areas. Most of the studies are small-scale, community-based studies. The methodology used in these studies pose problems both in terms of internal validity and generalizibility of the conclusions about occupational risks. The best available information are mere estimates. According to the international labor organization, in the year 2000, globally, approximately two million people died, at least 271 million people were injured and around 160 million people became ill as a result of occupation-related hazards or injuries.[6] A study (2004) from south India presented a picture of the farming sector, most of the fatal accidents resulted from the powered machinery. These were mainly due to lack of skills to operate them, with an annual fatality rate estimated as 22 per 100,000 farmers. There were 42 thresher accidents per 1,000 mechanical threshers per year.[4] Occupational diseases are also facing a transition. The new disease pattern like cancers, stress, HIV/AIDS, heart disease, geriatric problems, psychological diseases, musculoskeletal disorders and rehabilitation-related problems are showing an increasing trend. This new transition poses several challenges up on the health care system with new concepts of environmental legislation, ethical issues, safety regulations, insurance and high costs to healthcare. Occupational Health and Industrial Medicine Occupational medicine is best defined as specialized practice of medicine, public health and ancillary health professionals in occupational settings. The aim of occupational health being to promote health as well as to prevent related diseases and injuries and the impairments arising from themand to treat these conditions when work relate injury or illness occurs.[7] Occupational health services in India have gained momentum in the last two decades. The earlier practice of occupational medicine used to be purely clinical with little or no emphasis on epidemiological approach to workplace monitoring and control. The Royal Commission of Indian Labor made initial inquiries into occupational diseases in India between 1929-31 and reported no diseases. However, the commission recommended setting up an agency for research into industrial health. The commission also recommended creation of a cadre of medical inspectors for investigating the incidence of diseases in miners and instituting preventing measures. In 1942, under Indian Research Fund Association, the Government of India established Industrial Health Advisory committee. The Industrial Health Committee recommended creation of educational and research facilities in Industrial Health. In 1952, Department of Industrial Health was created under chief advisor of factories. Then in 1966, Central Labor Institute was established in Mumbai. National Institute of Occupational Health was established at Ahmedabad in 1969 to focus on the promotion and improvement of the total health of the working community and to provide safe and comfortable environment for work and living.[8] Critical Gaps between Medical Education and Occupational health and Safety Medical schools: At the time of Independence in 1947, India had 22 medical schools with a student intake of 1983 and without any specialized training in occupational health and disaster management.[9] Since then medical colleges have increased in number for instance the figure was 52 with an annual intake of 5874 undergraduates in 1960, this increased further in 1980 to 109 with annual student intake of 11,431. In year 2006, there are 242 Medical Council of India (MCI) certified medical colleges with around 27,000 undergraduate students. Still, they are not sensitized on occupational health and disaster management. The concentration has been on either short certificate courses or post-graduate degree, with no provision for training at the undergraduate levels. At present in India, the training in occupational medicine is scarce. Only six medical institutions in India offer specialized training at postgraduate level in occupational health/ industrial health. Short certificate courses in occupational medicine are also offered by various organizations like Indian Medical Association (IMA), Bharat Heavy Electricals Limited (BHEL), etc. Medical curriculum: Though, some medical institutions like: All India Institute of Medical Sciences (AIIMS) New Delhi, Rajiv Gandhi University of Health Sciences (RGUHS), Bangalore have taken initiatives to bridge the gap [Table - 3],[10],[11],[12] it is a small beginning. However, much needs to be done to modify the existing curriculum and most importantly to spread to other medical colleges on a fast track. Medical and health graduates: Health-care professionals are at a high risk of infection if they ignore safety measures and universal precautions. Indian health care providers are poorly trained to deal with occupation health and safety. Not many medical schools are specialized in faculty and specialized training. At present 8,000 occupational health specialists are needed against the current cadre of 100 to 150 occupational physicians getting qualified every year from central labor institute.[13] It is the need of the hour to train all health professionals, para-medics and industrial hygienists in occupational health safety and exposure to hazardous material at all levels of hierarchy in the health sector. Conclusion Occupational disease burden in India is growing at an unprecedented pace. As a result of market liberalization and globalization, the profile of occupational diseases has changed. Proportionate training of human resources in occupational health and safety has not taken place in our country. The medical fraternity has systematically ignored the importance of occupational health and safety and disaster management in teaching, training and epidemiological research. The government has not been playing a proactive role. Also, unemployment, poor hygienic conditions prevalent in the society, illiteracy and ignorance have further compounded the problem. There is an urgent need for strengthening skills, developing newer competencies and broadening our knowledge in occupational health and safety and disaster management. For those who are already attached with a company or industry, a blended or distant -learning module can be developed. Distance-learning is widely used in teaching of occupational health and safety and occupational medicine in developed countries like UK and USA. Already there is a one-year distance education course in occupational medicine conducted in Chennai. A ′blended course model′ should include contact phases and self-learning phases. In this way the time issue and availability of company doctors could be solved without compromising the quality of the course.[1] Apart from the traditional training in occupational health the need is to train occupational health physicians in the techniques of environmental epidemiology, environmental impact assessment and risk assessment modules. It is also worthwhile to look at the competency profile of the occupational health professionals. And therefore necessary to look at the competency model from legislative requirements, industry needs, employee demands, geographical demands and occupational physician′s technical and behavioral competencies. The academic community should take the first step in demonstrating its leadership to address the long neglected concerns of occupational health and safety. References
Copyright 2006 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe06024t1.jpg] [oe06024t2.jpg] [oe06024t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}