 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
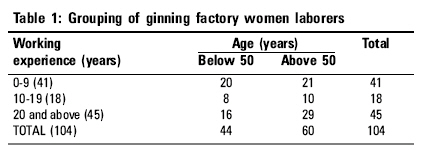
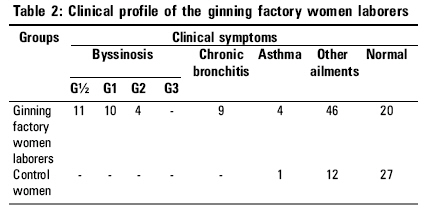
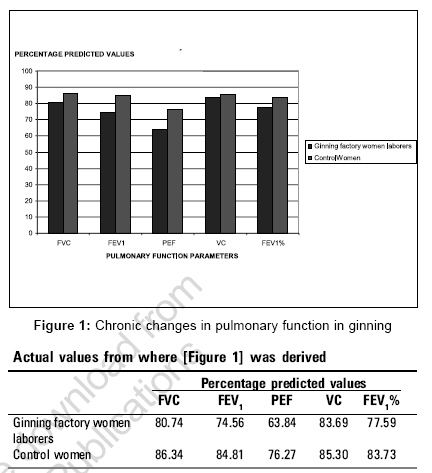
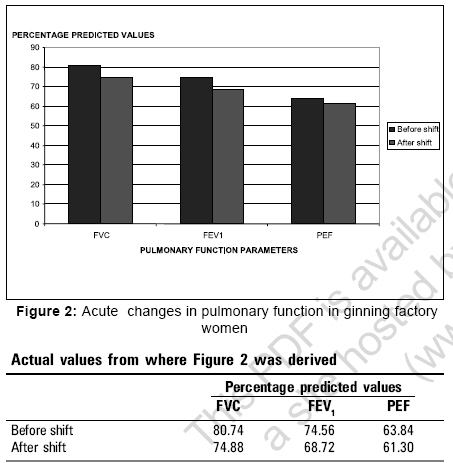
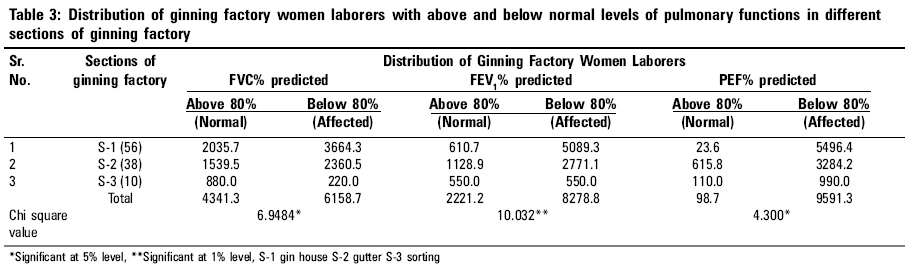
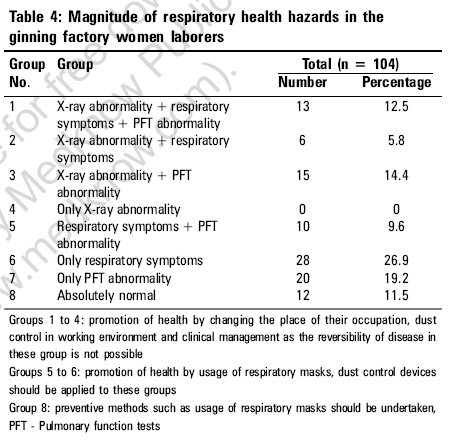
Indian Journal of Occupational and Environmental Medicine, Vol. 10, No. 3, September-December, 2006, pp. 116-120 Original Article Pulmonary health status of ginning factory women laborers in Tirupur, India Jannet JV, Jeyanthi GP Department of Bioinformatics, School of Biotechnology, Karunya Deemed University, Coimbatore - 641 114, Tamilnadu Code Number: oe06028 Abstract Ginning factories discharge large amounts of cotton dust, which leads to decreased pulmonary function in the exposed subjects. An attempt was made to study the pulmonary functions of women laborers employed in ginning factory located in Tirupur, a textile based city in Coimbatore district of Tamilnadu, India. The women were subjected to spirometric analysis and chest X-ray examinations. Occupational lung disorders that included byssinosis, chronic bronchitis and occupational asthma were studied in these women by assessing their pulmonary function tests, clinical symptoms, age and duration of exposure to cotton dust. Standard normal distribution, Chi-square analysis and multiple correlation analysis were the statistical methods applied in this study. Significant occupational acute and chronic pulmonary changes were observed in these women. Both age and duration of exposure together had a significant impact on their pulmonary function as per the results of the multiple correlation statistical analysis. There was a significant distribution of women with pulmonary impairment in all the sections of the ginning factory. Some recommendations were also suggested for controlling the occupational lung diseases caused by cotton dust.Keywords: Byssinosis, ginning process, pulmonary function tests, spirometry Introduction Byssinosis and other related respiratory abnormalities are well-known occupational respiratory diseases in textile mill workers caused by cotton dust pollution.[1] Cotton ginning and pressing have been identified as traditional industries under the unorganized sector which functions on a seasonal basis. The employees in ginning factories do not get registered under the Employees Security Insurance act. Till date in India, only a limited number of studies have been conducted to highlight the occupational hazards in ginning factories and there are hardly any studies conducted on the employees of ginning factories in Coimbatore district, Tamilnadu. Tirupur being a textile city in Coimbatore district, is the major exporter in cotton garments and ranks second to Coimbatore city where 18 ginning factories are situated employing 1500 laborers. Women are the major employees in these ginning factories. Although the textile industry in India has a large population for many years, health hazards in the women laborers in these ginning factories have been overlooked. Moreover all the studies conducted so far, were in late 1980s and there is no recent study, which portrays clearly the health status of ginning workers especially in Tirupur. Working women have multiple roles to play as a wife, a mother and an employee. Being subject to dual demands of home and workplace, they are liable to face crisis of adjustment which may cause stress and strain.[2] The present study was therefore undertaken to assess the pulmonary function of women laborers in a selected ginning factory at Tirupur. Materials and methods Selection of subjects A ginning factory located at Tirupur was chosen for the study. 104 women laborers working in different sections of the selected ginning factory namely the sorting house, gin house and gutter formed the experimental group. Sorting involves the sorting of cotton according to quality. The seeds are separated from cotton in the gin house and collected in the gutter. Among the 104 women laborers, 56 were employed in the gin house section, 38 in the gutter and 10 in the sorting section. Working hours of these workers were from 8 am to 5 pm for all week days during seasonal times, without using any self-protective measures. These women were grouped based on their age and working experience [Table - 1]. Assessment of pulmonary health A questionnaire (based on the British Medical Research Council recommendation and modified for the use in India) was used to collect information regarding their name, age, economic background, work-experience in the present occupation, anthropometric measurements, clinical conditions and dietary habits. Forty age and sex matched control women of similar economic status were selected for the study. Physical examination of respiratory health of workers and control group were conducted in accordance with recommendations outlined in the declaration of Helsinki. Four types of clinical symptomatic conditions were taken in to account to view the health conditions of ginning factory women laborers. They included byssinosis, chronic bronchitis, asthma and other ailments. Byssinosis is a condition observed in cotton dust exposed worker.[3] Byssinosis is an asthma-like condition in cotton workers worse at the beginning of the working week and most severe on returning to work after a longer period away from works. Therefore byssinosis is also ascribed as "Monday morning syndrome". The byssinotics in the selected ginning factory were graded according to their degrees of clinical symptoms suggested by Schilling.[4] Grade ½ - Occasional tightness of the chest on the first day of the working week, Grade 1 - Tightness of the chest and /or difficulty in breathing on each first day only of the working week, Grade 2 - Tightness of the chest and /or difficulty in breathing on the first and other days of the week and Grade 3 - Permanent respiratory disability from reduced ventilatory capacity. Chronic bronchitis was defined as coughing and phlegm for at least three months each year for not less than two successive years.[5] The chronic bronchitic women laborers were distinguished from byssinotics by showing lesser decrease in pulmonary function.[6] Occupational asthma is a chronic respiratory condition characterized by airway inflammation and intermittent episodes of bronchospasm that can be provided by a variety of stimuli at work.[7] It is usually witnessed whenever the subject is exposed to dust and is reversible. The occupational asthmatic workers were differentiated from byssinotics as they do not exhibit Monday morning chest tightness. Pulmonary function tests (PFT) Both the experimental and control group participants were subjected to PFT. Pulmonary function tests included spirometry and chest X-ray analysis. Assessment of pulmonary function by spirometry is a routine practice in epidemiological surveys in subjects exposed to toxic dusts and air pollutants.[8] Computerized portable vitalograph spirometer was used for conducting pulmonary function tests. The spirometry included the parametric indices of forced vital capacity (FVC), forced expiratory volume in one second (FEV 1 ), peak expiratory flow (PEF), vital capacity (VC) and FEV 1 /FVC%. The apparatus was calibrated every day and operated within the ambient temperature range of 20-25o C. The techniques in executing various lung function tests for the present study were based on the operation manual of the instrument with special reference to American Thoracic Society of Standardization of Spirometry.[9] The test was performed with subjects in sitting position with nose clip. The test was repeated three times to obtain appropriate values. The spirometry was carried out on the first day after a weekend holiday at the beginning of the shift and after the shift with a minimum of seven hours exposure to cotton dust. This is because the chest tightness, an important symptom of byssinosis - a cotton dust induced pulmonary disorder, is most commonly manifested after a holiday.[10] For assessing chronic changes, the observed values of FVC, FEV 1 PEF, VC and FEV 1 /FVC% were expressed as a percentage of the predicted values by using the regression equation developed by Vijayan.[11] Reduction of these values below 80% of predicted value was diagnosed as chronic obstruction in airways. The pre and post shift differences in FVC, FEV 1 and PEF were determined to find out acute changes over shift. The chest X-ray was also carried out for 104 experimental group and 40 control women to check for any radiographic abnormalities. Statistical analysis Standard normal distribution (two-tailed test) was used to assess the significance of chronic changes with the percentage predicted values of pulmonary function parameters (FVC, FEV 1 , PEF, VC, FEV 1 /FVC%) between exposed and control women. Standard normal distribution was also performed to assess the significance of acute changes by reviewing post shift pulmonary changes of PFT in the exposed women. Multiple correlation and regression analysis were carried out to find the impact of age and duration of exposure to cotton dust on PFT. Prevalence of respiratory impairments observed in these women employed in different sections of the ginning factory were statistically compared using Chi-square test. Results Physical characteristics The ginning factory women laborers recorded mean values of following physical parameters: Age - 51.8±8.3 years, weight - 45.1±8 Kg, height - 149±6.6 cms and blood pressure 117/76±10.7/1 mmHg. The mean values of weight and height were non-significantly lower than the control women. Pulmonary morbidity The clinical profile of the ginning factory women workers is shown in [Table - 2]. Among the 104 experimental group participants, 38(37%) reported symptoms of respiratory symptoms. Among them, 65.7% were byssinotic symptomatic, 23.7% were chronic bronchitic symptomatic and 10.53% were occupational asthmatic symptomatic. The prevalence of asthmatic symptoms was in accordance with earlier reports of asthma among cotton mill textile workers.[12],[13] 44% of experimental group participants reported other ailments like body aches, headaches, soriasis, defective eye sights, dental problems, hypertension and diabetes. This might be due to aging, poor nutrient diet, low hemoglobin content and heavy work. Nineteen per cent of the experimental group were normal. [Figure -1] illustrates the chronic pulmonary changes in ginning factory women laborers. There was significant reduction in FVC (Z = 2.02, significant at 5% level), FEV 1 (Z = 3.45, significant at 1% level), PEF (Z = 4.76, significant at 1% level) and FEV 1 /FVC ratio (Z = 3.36, significant at 1% level) in these women when compared to the control women which suggests chronic lung obstruction. Although the VC of these experimental women were different when compared to the control group, the Z value was not statistically significant. Four types of maneuver were recognized in ginning factory women laborers using spirometry based on spirometric assessment by Chattopadhyay.[14] Normal persons have FVC values above 80.0% and FEV 1 /FVC above 75%. In restrictive defects, FVC is below 79.99% and FEV 1 /FVC is above 75.0%. In obstructive cases FVC is above 80.0% but FEV 1 /FVC is below 74.99 mixed obstructive and restrictive defects express both FVC below 79.99 and FEV 1 /FVC below 74.99. In the present study, 64 normal (61.5%), 35 obstructive (33.7%), 1 restrictive (0.9%) and 4 mixed obstructive and restrictive type (3.8%) conditions were identified in 104 ginning factory women laborers. There was higher prevalence of obstructive conditions 87.5% (35 out of 40 respiratory abnormal cases) in the ginning factory women laborers. Among the 35 lung obstructive cases 33 showed mild obstruction (FEV 1 /FVC percentage between 65.00-74.99%) and 2 exhibited moderate effect (FEV 1 /FVC percentage between 50.0-64.99%). None of the women reported to have severe lung obstruction (FEV 1 /FVC percentage below 50.0%). Lung obstruction was more prevalent among byssinotic symptomatics (60.0%) compared to chronic bronchitic symptomatics (25.7%) and asthmatics (14.3%). Thirty five ginning factory women laborers who showed obstruction were challenged with the bronchodilator salbutamol to explain the nature of reversibility. The obstruction was reversible in 30 (85.7%) ginning factory women laborers and irreversible in 5 (14.3%) women laborers. The irreversibility was more prevalent more among laborers who reported chronic bronchitic symptoms. 86.5% of total 104 ginning factory women (90) laborers showed decline in percentage predicted PEF values. Among them 66.7% (60 out of 90) showed mild to moderate change in PEF i.e., percentage predicted PEF values between 60.0 to 80%. Remaining 33.3% (30 out of 90) showed severe (below 60.0% of predicted value) change in PEF. Significant acute changes in pulmonary function after the work shift (FVC: Z = 3.29, significant at 1% level, FEV 1: Z = 3.74, significant at 1% level) were also observed in these women [Figure - 2]. There was no statistically significant difference in PEF after the shift (Z = 1.402). The multiple correlation analysis conducted to determine the combined effects of age and duration of exposure showed five per cent significant correlation of percentage predicted values of pulmonary function indices with age above 50 years and duration of exposure above 20 years (FVC: r = 0.521; FEV 1 : r = 0.2823; PEF: r = 0.3305). Chest X-rays were taken for all the 104 experimental group participants. Seventy (67.3%) of them revealed normal pattern; thirty (28.8%) of them showed mild variation. The remaining four (3.9%) had severe obstructive lung disease which was clearly indicated in the chest X-rays. The above four women laborers whose X-rays showed severe lung obstruction, also reported to have chronic bronchitic and asthmatic symptoms. As quoted earlier,[3] no specific radiograph abnormalties were observed in women laborers exhibiting byssinotic symptoms. There were also significantly more number of women laborers with pulmonary impairment in all the sections of the ginning factory [Table - 3]. The magnitude of respiratory health hazards in the ginning factory women laborers is shown in [Table -4]. Discussion The present study concluded the high prevalence pulmonary abnormalities together with respiratory symptoms were high in the selected ginning factory. Although the ginning process is seasonal, both acute and chronic pulmonary abnormalities were visualized, which indicates both short-term and long-term effect of cotton dust on lungs. The prevalence of significantly more number of pulmonary impaired women laborers of all the sections of the ginning factory indicated the increased cotton dust in the entire premises of the ginning factory. The following recommendations were suggested for controlling the occupational lung diseases caused by cotton dust in the ginning factory women laborers:
Acknowledgment We kindly acknowledge all the staff members of department of biochemistry, Avinashilingam Deemed University, Coimbatore, Dr. Mahadevan, Pulmonologist, KG Hospitals, Coimbatore and management of Karunya Deemed University, Coimbatore, for their encouragement and support in this study.References
Copyright 2006 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe06028t1.jpg] [oe06028f1.jpg] [oe06028t3.jpg] [oe06028t4.jpg] [oe06028t2.jpg] [oe06028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}