 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
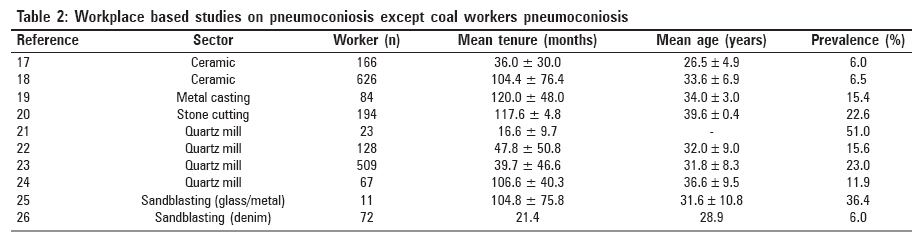
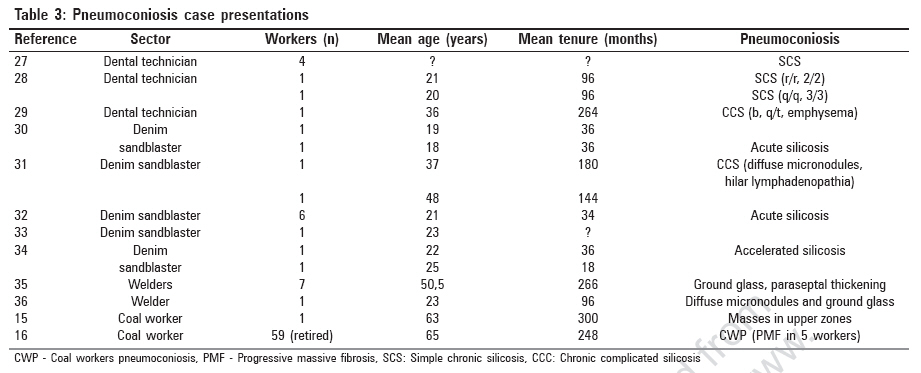
Indian Journal of Occupational and Environmental Medicine, Vol. 11, No. 2, May-August, 2007, pp. 50-55 Original Article General aspect of pneumoconiosis in Turkey Cimrin, Arif; Erdut, Zeki Dokuz Eylul University, Medical School, Chest Dept., Izmir Code Number: oe07011 Abstract During the past 20 years number of definitive occupational diseases has not increased above 1500 case/year according to official statistics in Turkey. Although pneumoconiosis is the most diagnosed occupational disease, incidence of pneumoconiosis is very low. The present paper aims at reaching conclusions on the true dimension of the pneumoconiosis problem by evaluating whole the studies and case presentations related to coal mine dust and crystalline silica exposure within occupational environment. Regarding the results of the workplace-based studies it could be predicted that 20,000 out of 220,000 workers in mining sector could have pneumoconiosis and approximately 5,000 new pneumoconiosis cases might have occurred each year. Case presentations show high-level dust exposures present at the work places. These working conditions might cause acute pneumoconiosis. Poor working conditions exist especially at small and micro scale establishments. In Turkey, infrastructural and superstructural problems on workplace supervision and follow-up, legal processes on workers' health are complicated. Turkey has to provide healthy working conditions to those small-scale workplaces. Providing relevant assistance with activating people of the developed countries should be on top of the global efforts.Keywords: Coal workers pneumoconiosis, occupational lung disease, silicosis Introduction Pneumoconiosis, different from bronchitis and asthma, is basically defined as lung′s non-neoplastic response to inhaled minerals and organic dust where structural changes are present and chemicals are included. [1] However mostly used to define the lung disease formed by accumulation of mineral particulates or fibers. [2] In industrialized countries, development of crystalline silica and coal mine dust-related classic pneumoconiosis has been taken under control by prevention of exposure or dynamic dust control precautions. However in developing countries, development of pneumoconiosis continues being a problem. In Takala′s opinion, developing countries constitute 60% of universal labor force and 80% of this force works at small-scale companies where heavy and dangerous duties are done and in unregistered economy. Five to 15% of those workers can benefit from occupational health services. Within this picture, traditional occupational problems such as industrial accidents and occupational diseases still maintain their importance in developing countries. [3],[4] Moreover, in developing countries, within the process of global structuring owing to establishment of new business areas and increase in demand, it can be said that the risk has increased for pneumoconiosis-development among the workers doing heavy jobs. Looking at the socioeconomic profile of Turkey with the data of 2005 the population is estimated to be 72,006,000. 21,928,000 of the population are employed. Sector-wise breakdown of the labor force employment is as follows; 27% agriculture, 20,3% industry, 5,5% construction, 47,2% services. Unregistered employment is a peculiarity of Turkey. It is estimated that as of December 2005, 48% of the total labor force is working unr egistered. According to official data there are 10,239,000 unregistered employees as of the same date. It is informed that unregistered employment in agricultural sector is 87.1% while it is 34,5% in non-agricultural sectors. [5],[6],[7] According to the statistics of 2002 general industry and place of employment census < 10 workers are employed at 94,9% and < 50 are employed at 3,09% of the total 2,139,289 places of employment. On the other hand, in the year 2004 the added value created at the 500 largest manufacturing companies is 37,9% percent of the total value while these companies employ only 2,32% of the total laborers. In other words, small companies where labor-intensive working is dominant are creating the actual employment. Average number of workers per enterprise is 3,68. [5],[7],[8] In Turkey, which is a developing country according to statistics of Ministry of Labor in the past 20 years, number of definitive occupational diseases has not gone above 1500 cases/year. During the recent years it is in between 300-500 cases/year. [5] Within the years 2000 to 2004, among all definitive occupational diseases, pneumoconiosis is the most diagnosed occupational disease as in the previous years. Between the years 2002 to 2004 the ratio of the diagnosed number of occupational diseases coming from mining sector to total occupational diseases are; 313/601, 301/440, 131/384 respectively. Within the same period numbers of diagnosed pneumoconiosis cases are 179, 288 and 131. [6] Pneumoconiosis constitute major portion of the occupational disease cases coming from the mining sector. In Turkey since 2000, permissible exposure limit for respirable mine dust has been limited to 5.0 mg/m 3 if SiO 2 content is less than 5%. If SiO 2 content is more than 5%, then the cut-off level is calculated with a formula: 25/SiO 2 % mg/m 3 . [9] What is the size of the population under risk of pneumoconiosis in Turkey? With respect to statistics of social security administration, there are 12,263 work places in mining sector, 440 of which are coalmines. Total number of insured workers at these work places is 221,938 of which 38,492 are working in coal mining. Among workers close to a million are working in business areas that have silicosis risk such as metal, machinery and textile. The size of the group under silicosis risk is not known. High unregistered employment ratio is another reason for the population under risk could not be estimated. In respect of these figures, occupational disease incidence in Turkey is %0,006. It is calculated that in coal mining occupational disease incidence is %0,002 and in non-coal mining sector %0,0005. As the picture defined above, Turkey is a country having serious socioeconomic restrictions. Whereas with an optimistic view taking %0,3-0,5 occupational disease incidence of European Union in 2002, in Turkey having over six million registered workers in the industrial sector, annually over around 20,000 new occupational disease has to be diagnosed. In Turkey, although the pneumoconiosis group is the most diagnosed occupational disease, incidence is very low in the official statistics. On the other hand, both the sudden expansion in the number of pneumoconiosis case notifications in the recent years and the results of the studies on pneumoconiosis frequency at coal and non-coal mining work places are very attention-attracting. Examination of this data could help forming an opinion on the topic of occupational disease in Turkey and shall contribute to the studies on control of pneumoconiosis in developing countries like Turkey. The present paper aims at reaching conclusions on the true dimension of the problem by evaluating as a whole the studies exploring the pneumoconiosis frequency related to coal mine dust and crystalline silica exposure and factors causing pneumoconiosis and case notifications within occupational environment. Materials and Methods The data on working life and socio-economy in Turkey are obtained from the printed statistics material and web site of social security administration ( www.ssk.gov.tr ) and Turkish statistical institute ( www.die.gov.tr ) as well as web site of ministry of labor and social security ( www.csgb.gov.tr ). For reaching the studies on pneumoconiosis published in peer review journals and non-peer review journals, searches were made using key words pneumoconiosis, coal miners pneumoconiosis, silicosis, occupational lung disease in Turkish and English at internet sites www.turkishmedline.com , www.ulakbim.gov.tr , www.akcigerarsivi.com , www.ataturksanatoryumu.com , www.pubmed.com . Separately, all issues of peer review journals and non-peer review journals national pulmonary medicine periodicals which could be found issued within last 10 years period and abstract books of national and international congresses were examined. Pneumoconiosis case presentations and studies systematically carried out at the work places on pneumoconiosis frequency, demographic features of workers and their work stories, data on work place dust measurements were evaluated. It has been tried reaching to the complete texts of the studies by conversing with the authors. Results Coal workers pneumoconiosis (CWP) Case presentations related to CWP are at very low levels. These are cases presented because of interesting clinical peculiarities accompanying pneumoconiosis. [14],[15] Other study is the group of cases in which at 59 cases′ bronchoscopic findings were evaluated with suspicion of cancer. [16] As could be seen in the studies primary aim of publication is not pneumoconiosis. When it is taken into consideration that CWP is the mostly diagnosed occupational disease the main reason for scarcity of CWP case publications seems that physicians perceive those cases as routine issues and due to this reason consider these are not worthwhile publishing. Pneumoconiosis except CWP All workplace-based studies on pneumoconiosis except CWP are cross-sectional. Contrary to evaluated workers number was small, highness in pneumoconiosis prevalence is attention attracting. The work places where high pravelence was determined are all small scale businesses. Especially at sandblasting business high concentrated dust exposure is present. Sevinc and colleagues reported 100 mg/m 3 dust concentration at sandblasting work places. [25] Silicosis frequency was found 10% over general average at bituminous coal workers who are thought to be working in more dusty environment with respect to work done and it is calculated that working in a dusty environment increases silicosis risk three times. [20] Except the study of Simsek and colleagues in workplace-based studies complicated pneumoconiosis cases were not mentioned. [37] In the studies carried out in recent years it is attention attracting that workers are in young age group and their total working period is short. It can be said that this situation is related to employers frequently changing workers in order to avoid legal obligations with regard to pneumoconiosis. For example, in the study of Polatli and colleagues, while the average working period of pneumoconiosis diagnosed workers was eight years, in the study of Öztürk and colleagues, carried out five years later, the average working period of quartz mill workers was five years and 25% of the workers mentioned that they worked in the same sector previously. [23] This situation is the proof that by an important ratio workers have worked at other similar work places in the same area. It is also emphasized that in spite of high silicosis frequency the reason for not seeing complicated silicosis could be related to frequent change of workers. Also the case presentations covering pneumoconiosis related to non-coal inorganic dust being silica on top accumulate in a few line of business [Table - 3]. The first group case presentations is simple pneumoconiosis cases among dental technicians in 1991. [27] There are case notifications beginning from 2003 doing sandblasting at young ages. Within these cases morbidity and even mortality connected to acute/accelerated pneumoconiosis is subject matter. Within the last few years, sudden expansion of silicosis among sandblasting workers is being experienced. Akgün and colleagues determined eight new silicosis cases [38] doing denim sandblasting in addition to eight cases they notified in 2006. [30],[32] One of the common peculiarities of these cases is that pneumoconiosis diagnosis was fixed not while working but following their application to health institutions due to complaints. Major reason for this situation is that they have been employed unregistered at small-scale companies. The workers employed unregistered were laid off following short working period in poor working conditions being exposed to dust and within a short period following being laid off pneumoconiosis was diagnosed. The situation could be defended by saying this is due to ignorance of the employers and employees in Turkey. Whatever the reason, the presence of such cases show the uncontrolled and poor working environment at small scale companies. In two articles covering workers doing welding, micro nodular changes harmonious with pneumoconiosis and pulmonary parenchymal inflammation were determined. [35],[36] Discussion In Turkey according to official statistics occupational disease incidence is very low during the last 20 years. Whereas, workplace-based studies and notified acute silicosis cases show that workers in coal and non-coal mining areas are under serious pneumoconiosis risk. According to the results of these studies it could be predicted that 20,000 out of 220,000 workers in mining sector could have pneumoconiosis and approximately 5,000 new pneumoconiosis cases would appear each year. With respect to workers′ health security precautions, although present respirable dust levels would be determined within legal limits at well-organized and state-operated coal mines it is seen that new CWP cases come into scene. According to this low density chronic exposure is present. In a study carried out in the USA, relation between growth of rapid progressive CWP cases and poor working conditions at small scale companies has been emphasized. [39] In Turkey within the process of current economic restructuring by privatization and authorizing subcontractors, enterprises are made smaller. Insufficiency of workers′ health and security practices at small-scale companies is known. Because of that whatever the size is at all mining companies′ labor health and security practices have to be actively realized. Present legal respirable dust concentration levels should be re-determined and dust measurement-observance standards reviewed. When looked at non-coal mining area, determined pneumoconiosis cases are simple pneumoconiosis cases. However case presentations show that high level dust exposures are present at these work places. And these working conditions can cause acute pneumoconiosis. Poor working conditions exist especially at small and micro scale establishments. Turkey′s domestic and foreign debt payments restrict new investments and new business areas could not be created. 98% of the business places are small scale and labor-intensive working conditions prevail. Added value created is small because traditional products are produced at those business places. Low profits limit remuneration of labor. On the other hand there is a huge potential of work force and approximately half of the work force is employed unregistered. Unemployment rate is very high especially among unqualified work force. Total inactive work force ratio is 14,2%. 25,6% of the total population is living below poverty level. Domestic migration caused by unemployment and poverty increases demand for employment and work force gets more and more cheaper. In Turkey, the ratio of work force to salary earners is only 5,65%, which is the determining point of arranging working conditions through collective bargaining. A serious process of de-unionizing and de-organizing is going on. That is to say those workers in an organized way do not have the power to bargain on their working rights. In Turkey, the infrastructural and superstructural problems at work place, supervision and follow-up, legal processes on workers′ health are also complicated. For example, between 1994 and 1996 High Health Committee of Social Security Administration, the deciding entity on the subjects of disability and compensation by evaluating occupational health problems examined total 5000 files in which 59,8% of them were examined with respect to pneumoconiosis and it is informed that for 48,3% of those files definite pneumoconiosis diagnosed. [40] That is to say approximately 2,500 suspected pneumoconiosis cases were evaluated at the Committee and pneumoconiosis diagnosis on about 1,200 of them was decided. However, the fact that those were not reflected in the official statistics could be explained by bureaucratic issues. All this picture reveals why young age unqualified work force has pneumoconiosis, why occupational diseases are not diagnosed at unregistered workers and why these cases do not get reflected in the statistics. Present situation could be evaluated as usual problems of a developing country. However, Turkey made its preference in favor of small-medium sized companies and it has to provide modern working conditions at those business places. On the other side, under prevailing conditions it is not seen possible that working conditions of individuals living under heavy socioeconomic problems which are not in conformity with human rights could get better spontaneously. However, it is known that small-scale companies where denim processing, dental prosthesis, metal casting and glass embroidery are done make production for exports as subcontractors. Economically developed countries where these goods are consumed pave the way for misuse of the laborers themselves. Naturally persons and institutions using the product are responsible from the health of the workers regardless of country of production. For this reason informing and activating the consumer masses of developed countries who do not sufficiently notice they use the produces of the workers working at health threatening dirty jobs should be on top of the national and global corrective efforts. [41],[42] References
Copyright 2007 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe07011t2.jpg] [oe07011t3.jpg] [oe07011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}