 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
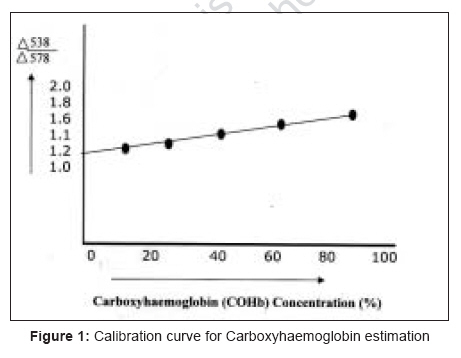
Indian Journal of Occupational and Environmental Medicine, Vol. 11, No. 2, May-August, 2007, pp. 56-60 Original Article Methylene chloride exposure and carboxyhemoglobin levels in cabinetmakers Banjoko, Sunny O.; Sridhar Mynapelli, K.C.; Ogunkola, Isiah O.; Masheyi, Olatunde O. Department of Chemical Pathology, College of Health Sciences, Obafemi Awolowo University, Ile-Ife Code Number: oe07012 Abstract Methylene chloride (MeCl 2) is a clear colorless volatile sweet smelling lipophilic solvent used as a constituent of wood vanishes and paints. Human exposure is mainly due to inhalation and its biotransformation by the hepatic mixed function oxidases (MFO) leads to formation of carbon monoxide (CO). Simultaneous exposure to MeCl 2 and increased ambient CO results in undesirably increased carboxyhemoglobin (COHb) formation, which predisposes to carboxyhemoglobinaemia with the central nervous system as the primary target organ of toxicity. In this study, ambient CO levels were determined using a CO personal monitor in different pasts of Ibadan Nigeria and work place microenvironment of 50 Cabinet makers (test group) and 50 volunteer (control) in non-furniture making occupations. Mann Whitney U and Kruskaal Wallis were the statistical methods of analysis used. Questionnaires were administered to both groups carboxyhaemoglobin levels were determined in venous blood drawn from individuals in the two groups by differential spectrophotometric method. Ambient CO levels in Ibadan were observed to be between 4 and 52 ppm with a mean of 20 ppm. Work environment CO levels were significantly higher in test subjects than controls at 5.2 ± 1.08 ppm and 2.08 ± 0.91 ppm respectively ( P <0.001). COHb in cabinetmakers with mean working hours of 9.48 ± 2.9 per day was 3.95 ± 1.35 (%) while that of controls with mean working hours of 8.0 ± 0.8 per day was 2.08 ± 0.91 ppm ( P <0.001). Smoking however did not significantly affect the COHb levels within the two groups ( P >0.05). It is therefore imperative to substitute MeCl 2 for safer chemicals in wood vanish and paints and the use of protective gas masks and adequate ventilation should be mandatory whenever MeCl 2 is used.Keywords: Carbon monoxide, carboxyhaemoglobin, methylene chloride Introduction Methylene chloride (MeCl 2), also known as dichloromethane (DCM), methylene dichloride, methylene bichloride (CH 2 Cl 2) is a chlorinated hydrocarbon of relatively low flash point, widely used in modern industry as a solvent for cellulose esters, fats, oils, resins and rubber. It forms a large proportion of certain proprietary paint removers and has also been used in the paint trade to raise the flash points of lacquers. [1] MeCl 2 is a volatile, clear, colorless, hypophilic solvent. It has a mild sweet odor with an olfactory threshold of 100 - 300 ppm. [2] It is also an anesthetic with a pleasant chloroform-like smell, slightly more toxic and irritant them chloroform. [2] The primary target organ of methylene chloride toxicity is the central nervous system (CNS). [4],[5] These effect results from both direct solvent related narcosis and endogenous promotion of CO with subsequent carboxyhemoglobin (COHb) formation. [6],[7],[8] Human subjects exposed to concentration of 550 ppm or less for one hour (1 hr.) have COHb levels of 1-4%. These levels increased to an average of 10%. saturation within one hour after exposure to 1000 pm for two hours. [9] COHb in excess of 10% was reported following exposure to 250 ppm of CO for 7.5 hours. [10] If CO is inhaled from either the environment or from tobacco smoke; this exogenous CO exposure leads to additional COHb formation in additive fashion. [10] The most serious manifestations of MeCl 2 poisoning are headache and nausea in the healthy and sufficient cardiovascular stress in the patient with coronary heart disease to cause cardiac ischemia and unconsciousness, which could be fatal. [9],[11] Level of COHb in the blood following exposure to MeCl 2 are both dose and times-dependent. Human exposure to MeCl 2 is mainly due to inhalation and it is usually occupational in nature. [12] MeCl 2 has a wide variety of application and these include; cleaning, degreasing, paint and vanish thinning, manufacturing of synthetic fibers and plastic, uses as aerosol propellant, blowing agent for food and spices uses as grain fumigant low pressure refridgerant uses in certain inks, adhesives, pharmaceuticals and photographic films. It has been estimated that more than a million people are at risk of occupational exposure. Physical exercise performed during exposure to MeCl 2 will produce higher blood - carboxyhaemoglobin levels than those found in sedentary workers. [13],[14] Under a moderate workload, an exposure to 10 ppm for 7.5 hours may cause a COHb saturation of about 5% at the end of the exposure period. [14] Other factors, including smoking and exposure to combustion and automobile exhaust is expected to increase COHb levels. Symptoms of CO toxicity and poisoning include: loss of consciousness, neurological abnormalities, myocardial ischemia, pulmonary edema, metabolic acidosis, headache, nausea and delayed neuropsychological features [Figure - 1]. [15] This study was to assess the extent of risk of the use of MeCl 2 coupled with the ambient CO level in the environment. Materials and Methods Chemicals and instrument Subjects Fifty age-matched individuals who were students and workers within the University College Hospital, Ibadan, Nigeria were recruited as controls. Smokers were not included in the study to reduce confounding factors. Questionnaire Blood sample Determination of carboxyhaemoglobin levels Preparation of calibration curve
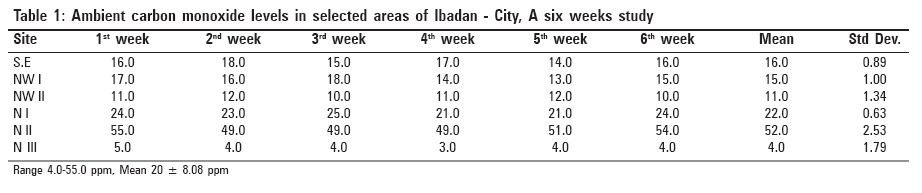
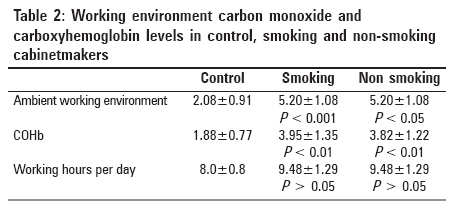
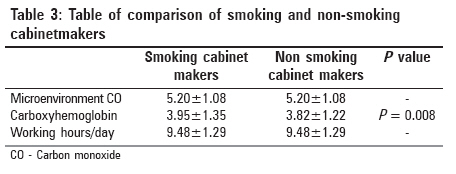
Ambient carbon monoxide estimation The determinations were done using a digital battery operated personal CO monitor. The zero knob was depressed to erase any previous reading and to activate its use. It was then placed in the desired environment for between one and three min at which the readings were stabilized. The stable reading, which was direct CO concentration value was recorded. This same monitor was used for ambient air, the cabinetmaker′s workshops and the offices microenvironment′s CO concentrations. Data analysis Results Ambient CO levels in Ibadan city ranged between 4.0-55.0 pp with a mean rate and standard deviate of 2018.08 mm [Table - 1]. The cabinetmakers were averagely exposed to a significantly higher carbon monoxide levels (P < 0.001) compared to the control group [Table - 2]. COHb in cabinet makers with mean working hours of 9.48 ± 2.9 per day was (3.95 ± 1.35%) while that of controls with mean working hours of 8.0 ± 0.8 per day was 2.08 ± 0.91% (P < 0.001) [Table - 2]. The COhb was significantly raised in both smoking and non-smoking cabinetmakers: P< 0.01 [Table - 2]. There was no significant difference between the COhb levels in smoking and non-smoking cabinetmakers (P = 0.008) [Table - 3]. Discussion In humans, COHb occurs naturally at low concentration as an endogenous pigment derived from the breakdown of red cells. [17] Ambient concentration of COHb have been reported in various studies. [8] These concentrations are influenced largely by environmental factors and practices associated with incomplete combust of carbonaceous fuels constituting CO among others. The majority of the population is invariably exposed to varied ambient background CO levels. The resting level of COHb observed in the control subjects were high compared to 1.5% COHb recommendation of the American Clean Air Acts Quality Standards of 1971, the cabinet workers on the other hand had a still higher value of carboxy hemoglobin [Table - 2]. This is no doubt due to increased background CO level coupled with exposure to methylene chloride, which is bio-transformed to carbon monoxide. Similar results were obtained previously by other investigators in a furniture worker exposed to methylene chloride. [18] The detrimental effect of CO is consequent on the fact that inhaled CO readily combines with hemoglobin (with an affinity of over 200 times) to form COHb. Therefore a low concentration of CO can result in a clinically significant reduction in the oxygen carrying capacity of the blood. In addition, the presence of COHb shifts the oxyhemoglobin dissociation curve to the left so that tissue oxygen tension must fall to lower levels before the remaining oxyhemoglobin can give up its oxygen. Following CO exposure, the resultant decrease in oxygen carrying capacity of the blood together with the unpaired release of oxygen to the tissues lead to a large tissue oxygen deficiency (tissue hypoxia). The resultant effect is that exercise tolerance is reduced. It was however observed that there was no significant difference in the COHb levels of smoking and non-smoking cabinet worker. This could be attributed to physiological adaptation to a constantly raised COHb. Further, in experimental animals, common air pollutants, such as ozone and nitrogen dioxide have been shown to cause shifts in the thymocyte and spleen T-lymphocyte subpopulation at ambient level of exposure. [19] There was a delay in the deoxyribonucleic acid (DNA) turn over in the lymphocytes of these animals. Suggesting there could be immune compromisation due to air pollution. MeCl 2 exposure up to toxic level had been reported to result in rhabdomyolysis. [20] Cabinet workers with undiagnosed or diagnosed cardiovascular disease may be at risk of myocardiac ischemia due to increased exposure to work place CO and combined increased COHb from ambient CO exposure and bio-transformed MeCl 2 . [21] Such workers also have low tolerance to simple exercise like climbing of staircases and walking long distances. Tuntinalli et al ., [22] listed CO as a cause of rhabdomyolysis and myoglobinuria. It is therefore imperative for regulatory public health authorities to enforce the use of facemasks during spray-painting and such places of work should be well ventilated. There is also the need for enlightenment and health education on the use of such chemicals. Effort should also be made by manufacturers to eliminate the use of methylene chloride while replacing it with a less toxic base. Acknowledgement The authors acknowledge the kind gesture of the Oyo State, Nigeria. Ministry of Environment for granting the use of it′s personal CO monitor and CO gas standards for the study. References
Copyright 2007 - Indian Journal of Occupational and Environmental Medicine The following images related to this document are available:Photo images[oe07012t2.jpg] [oe07012f1.jpg] [oe07012t1.jpg] [oe07012t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}